Nearly 1 billion people globally1 are served by health care facilities that do not have regular or consistent power. Unreliable energy disrupts routine and emergency care—from running diagnostic tests to ensuring vaccines stay cold. As heatwaves, floods, and other extreme weather events become more common, energy disruptions are expected to increase due to events like power outages and heat stress on existing infrastructure. To address these challenges in the last mile of polio eradication and reduce its carbon footprint, the GPEI and partners have turned to solar power, a more affordable, reliable and climate-resilient energy source to power polio vaccination and surveillance activities.
Solar powered vaccine refrigerators
For decades,2 refrigerators powered by fossil fuels like kerosene or petrol were essential to maintaining vaccines at just the right temperature. Yet, these refrigerators emitted greenhouse gases (GHGs), were relatively expensive to operate and were vulnerable to disruptions in the national energy supply. Now, the GPEI and its partners significantly rely on solar power, specifically, Solar Direct Drive (SDD) vaccine refrigerators.3 SDD refrigerators can run for days without power if needed, not only making them more dependable, but also extending the programme’s reach in some of the most difficult yet critical areas to end polio.
In the Democratic Republic of the Congo,4 a country the size of Western Europe with difficult terrain and longstanding security challenges, millions of children have missed out on polio and other life-saving vaccines in part because vaccines could not be kept cold on the trip to reach them. In 2016, just 16% of health centres in the country had a working refrigerator. Between 2018 and 2021, Gavi and its partners helped address this gap by delivering over 5,500 new solar-powered fridges across the country.
On the remote islands of Lake Chad,5 the introduction of solar powered refrigerators means that parents and health workers can simply go to the community center on the island, rather than travelling long distances by boat to receive or administer polio vaccines. Meanwhile, in Somalia, a country that experiences frequent interruptions in power supply, all vaccine refrigerators from the regional storage points down to the community-level administration are now powered by SDD refrigerators.
Solar powered surveillance
During surveillance, stool and environmental samples travel through the vaccine cold chain in reverse – from the field site or clinic to the regional and global laboratories for testing. In January 2021, an insurgency in Borno state, Nigeria, showed the world just how vital reliable, climate-resilient energy for surveillance is. The insurgency resulted in over ten months of power outages, including at the University of Maiduguri Teaching Hospital, which houses one of only two national polio laboratories in Nigeria. This meant that samples from the 10 most vulnerable states for polio transmission in northern Nigeria couldn’t be tested.
To help the lab get back on track as quickly as possible and prevent future power issues, the World Health Organization6 provided 48 solar panels. As a result, throughout most of 2021, more than 10,000 stool samples of children with acute flaccid paralysis (AFP) and more than 500 environmental samples were analyzed by the laboratory, an essential step to finding and stopping the virus.
In the face of the climate crisis and its many knock-on effects, including extreme weather events and even more persistent conflicts, health programmes like the GPEI must continue to integrate renewable energy at every turn. From refrigerators to powering entire laboratories, solar power technology has become a key energy source to help reduce the GPEI’s GHG emissions and ensure a polio-free future.
[1] Energizing health: accelerating electricity access in health-care facilities. Geneva: World Health Organization, the World Bank, Sustainable Energy for All and the International Renewable Energy Agency; 2023. Licence: CC BY-NC-SA 3.0 IGO [2] https://www.unicef.org/innovation/stories/using-sun-keep-vaccines-cool [3] https://apps.who.int/iris/bitstream/handle/10665/254715/WHO-IVB-17.01-eng.pdf;sequence=1 [4] https://www.gavi.org/vaccineswork/drcs-solar-revolution [5] https://archive.polioeradication.org/news-post/protecting-against-polio-in-lake-chad/ [6] https://www.afro.who.int/news/who-delivers-solar-panels-accredited-polio-laboratory-borno-state
One of the first tasks they took on was to find ways to detect the possible spread of an outbreak of variant poliovirus that was confirmed in December 2022 after a paralysed child living near the border with Chad tested positive for the virus. Immediately after the start of the conflict, they worked to maintain the essential function of surveillance for acute flaccid paralysis (AFP) – the most common symptom of polio – in children.
Prioritizing essential polio functions
Much like a relay race, in AFP surveillance, speed and coordination are key. Once health teams find a child with AFP, the race begins. But emergencies often present additional hurdles. In one of the localities in Sudan’s White Nile state, Ahmed Masaood, a health worker, was tasked with collecting two stool samples from a child presenting with AFP. However, when the roads outside turned unsafe during Ahmed’s visit, he ended up having to seek refuge with the family he was visiting for two nights. As soon as he could, he rushed to the state cold room with his stool carrier to drop off the samples for storage until they could be tested.
The next lap of the race involves getting children’s stool samples to a WHO-accredited laboratory for testing. Due to the conflict, Sudan’s polio laboratory is not functioning, which meant the polio programme urgently needed to look for another laboratory to test stool samples to determine if children presenting with AFP had indeed been infected with poliovirus.
In a remarkable partnership, Sudan’s polio programme teamed up with Egypt’s health authorities to use the VACSERA laboratory in Giza for this crucial task. Senior decision makers at the Egyptian Ministry of Health not only approved the collaboration but instructed for it to begin as soon as possible.
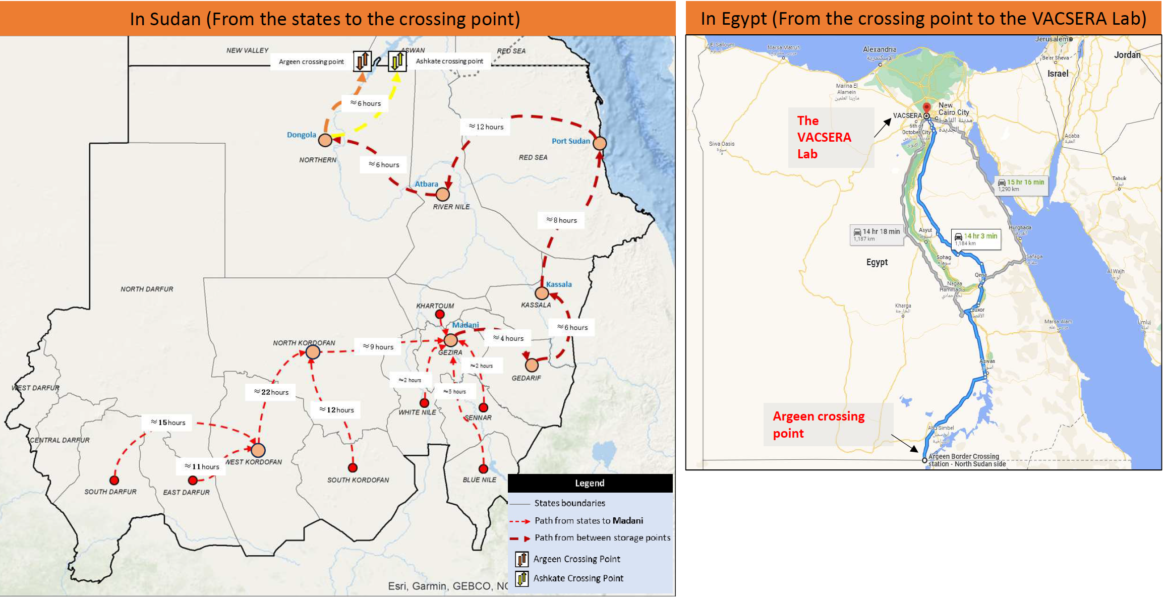
In June, the polio programme in Sudan completed a pilot mission to transport stool samples to the VACSERA laboratory for testing. With the conflict impacting movement and security on the roads, creativity was required to get the samples from collection points identified, such as Gezira to Port Sudan to Dongola, all the way to the border. Throughout, health workers relied on two criteria to ensure safe passage for themselves and their cargo: first, their neutrality, and second, their status in communities. The health workers who made this happen are known to and trusted by the communities they serve, and that trust, in many cases built over decades, facilitated their travel by road.
The first shipment of stool carriers passed through five stops in different states following a pathway assessed for security considerations. In Red Sea state, Dr Thabit Mohammed Elsadig, a WHO Public Health Officer, spent three days pulling together all the resources drivers would need, from permits and security clearances to cash, fuel and food. As the situation was formally graded as a level three emergency, this triggered WHO’s Emergency Response Procedures, effectively enabling staff to respond and repurpose resources at speed. In some cases, Dr Thabit and others used their own resources to make things happen.
At each stop, health workers picked up more stool samplesfrom their colleagues. They checkedtemperature controls in the sample carrier and replaced old ice packs with fresh ones to maintaintemperature and handling protocols of the reverse cold chain.
With the occupation of the National Public Health Lab in Khartoum by one of the parties, Hatim Babiker Othman, National Coordinator for the Polio Lab in Sudan, moved to Port Sudan during the first month of the conflict and started to restructure the polio lab’s functions. He organized samples in small boxes, assigned lab numbers, and established effective communication with the focal point in Egypt, to coordinate the handover of samples. Hatim traveled with the samples from Port Sudan to Atbara, Dongola, and finally, the Argeen border crossing point.
Meanwhile, WHO colleagues contacted the Egyptian Ministry of Health to confirm that, at last, the samples were on their way to the border. At the Argeen Gate, border officials examined the boxes and their contents. Dr Thabit recalled thinking that if anything went wrong at this point, all their efforts – days of planning and transport by road – would have gone to waste.
“The sample carriers were like trunks of gold for us. We hoped they would treat them well, and they did,” he said, with reference to their value in signaling any epidemiological developments related to the ongoing variant poliovirus outbreak.
Exemplary inter-country support
Once they received a prompt from WHO, a team from Egypt’s Aswan Governorate of Health set out on a six-hour journey to the shared border. There, they collected the samples and headed back to the health facility in Aswan for more fresh ice packs before driving to the VACSERA laboratory in Giza, a 14-hour drive away. The entire journey from Madani, Sudan, to Giza, Egypt, can take up to 56 hours and demands absolute precision in planning and execution.
Acknowledging Egypt’s generous support, Dr Ni’ma Saeed Abid, WHO’s Representative in Sudan said, “Our partners in Egypt have demonstrated how stronginter-country collaboration can help in ending diseases. We remain grateful to them for their timely support, and to every link in this chain of coordination. This support is a demonstration of ‘delivering as one WHO’.”
On 16 June 2023, VACSERA received a shipment of 56 stool samples for testing for poliovirus.Lab personnel prioritized Sudan’s samples for immediate testing, and the testing process began on the day of arrival.Final results were shared in 11 days — a full 10 days less than the standard three weeks. The results were also good news: no sample tested positive for variant poliovirus.
“Our heroic health workers stayed to deliver our mandate and support the most vulnerable communities in the face of the ongoing conflict,” Dr Nima said. “They are continuously finding extraordinary solutions to continue to protect children from polio and other vaccine-preventable diseases. This is a lesson to be followed by the integrated disease surveillance team. It reinforces what we believe in:everything is possible, with strong determination and will.”
The vast machinery of the global polio eradication programme is much like the inner workings of a clock – a network of interconnected people, organizations and programmes that together are more powerful than the sum of their parts. Collaboration is foundational to eradication, and every eradicator plays a part in edging the programme closer to its goals.
But in some cases, individual eradicators develop capacities or practices that enable programmatic leaps. Dr Humayun Asghar is one of those outsize drivers of progress. His initiatives around early laboratory testing of stool samples of children with acute flaccid paralysis (AFP), his efforts to create a cross-regional network of labs, and his efforts to set up a large pioneering network of environmental surveillance sites in Egypt are innovations that today power the programme’s surveillance capacity. We know where the virus is, even in the absence of paralytic polio cases, largely thanks to his work.
In 1988, when Dr Humayun joined the National Institute of Health (NIH) in Pakistan’s capital city of Islamabad, polio was paralysing more than 1000 children worldwide every day and the Global Polio Eradication Initiative (GPEI) was just being set up. Dr Humayun spotted an opportunity to stop the spread of poliovirus by tracking it – which meant identifying which children with AFP were infected with poliovirus and which children were experiencing paralysis for other reasons. In 1991, Dr Humayun began to contact pediatricians and, later, vaccinators, to collect stool samples from children who presented with AFP to test them for poliovirus infection. In a nod to the doctors’ and vaccinators’ contribution, Dr Humayun shared the results immediately with the reporting individual, regardless of their location.
The information filled a gap for physicians who wanted to know why their patients were unwell, and it provided a new level of detail on the virus’ whereabouts. Word got around and soon, more and more doctors started sending in their AFP patients’ stool samples. As the practice grew, processes needed to be formalized: Dr Humayun and his colleagues had to ensure stool samples were reaching them in the right conditions for testing, which led to the establishment of a set of criteria and standard operating procedures around the transportation of stool samples – something known today as the reverse cold chain.
The dawn of AFP surveillance in Pakistan
This new system unveiled the dawn of an era of detailed, systematic surveillance for AFP, the most common, tell-tale symptom of poliovirus infection. That it grew out of mutual trust and collaboration with focal points in the community reaffirmed Dr Humayun’s belief, “If you offer service to the community, the community serves you.”
In their quest to fill in gaps in disease surveillance and formalize a practice of testing samples from AFP patients, Dr Humayun and his colleagues succeeded in establishing the first poliovirus laboratory in Pakistan.
Dr Hamid Jafari, WHO Polio Director for the Eastern Mediterranean Region, says this contribution to eradication cannot be overstated.
“Dr Humayun has sowed the seeds of AFP surveillance in Pakistan all through his own initiative and drive and nurtured and supported the lab network in the Eastern Mediterranean Region; as one of the architects of the regional and global laboratory network, he has contributed to building a great legacy.”
Advancing the Region’s work
Over the intervening decades, Dr Humayun has helped the Region’s laboratory network grow in size and skill, bringing in new practices such as testing for poliovirus in sewage water (environmental surveillance) and then harnessing this new practice to test for the presence of other diseases – most recently, COVID-19. He also took the practice out of the Eastern Mediterranean Region and into the African Region, supporting the polio laboratory in Nigeria to introduce environmental surveillance.
Testing for and tracking the virus in stool samples and sewage water enabled the programme to identify different types of poliovirus, and by building on this, a practice was developed to conduct nucleotide sequencing, which provides a fuller picture of viruses’ lineage and allows scientists to identify which family any given poliovirus belongs to. Dr Humayun attributes these accomplishments to laboratory staff, who strengthened their own capacity to diagnose polio without waiting for results from other global specialized laboratories.
Supporting others to grow
Since he joined WHO’s Eastern Mediterranean Region in February 2002, Dr Humayun has served in several capacities – as Scientist Virologist, Regional Advisor for Public Health Laboratories, and finally as the Coordinator for the Region’s Poliovirus surveillance, Laboratory support and Data management. He credits two mentors in particular for inspiring his career – the late Dr Helmy Wahdan, former Polio Director for WHO’s Eastern Mediterranean Region, and Dr Olen Kew, a poliovirus scientist – and, over the course of his career, has tried to pay that inspiration forwards.
“Dr Humayun has mentored and supported young scientists and laboratory specialists across the Region to advance their skills and careers,” said Dr Nima Saeed Abid, WHO Representative for Sudan. “He has been a true leader in his field.”
Perhaps unsurprisingly, Dr Humayun believes one of the keys to eradicating polio lies not in the lab, but in people: in empowering and engaging the workforce by incentivizing them with education, training and promotion.
On the occasion of his retirement in May 2023, Dr Humayun expressed gratitude that he was able to witness and contribute to two important milestones: the eradication of wild poliovirus types 2 and 3.
And when the eradication of WPV1 does happen, he says, “I will be cheering from the sidelines, alongside so many other vital contributors to the programme’s legacy.”
After completing her bachelor’s degree in medical laboratory science, she cut her teeth in a HIV drug resistance lab in Botswana, where she tested blood samples to determine whether a patient with HIV had a mutated form of the virus which did not respond to antiretroviral therapy.
“Once you are in the lab you realize it’s not just a job, it’s more like a calling,” she says. “Someone sends samples to you, and you are the first one to see results and ask, ‘how is this going to impact the patient, the community as a whole, and then the country as a whole?’”
In 2019, just before the onset of the COVID-19 pandemic, Mphoyakgosi was transferred to the National Health Laboratory and when the pandemic hit, she was one of the first national experts to be trained by World Health Organization on how to test for COVID-19.
This period was a career highlight for Mphoyakgosi. “COVID-19 taught us a lot. When we get outbreaks now, we have learnt from COVID what can be done better,” she says.
Currently, as part of polio prevention, she tests wastewater samples for the poliovirus. And believes firmly in homegrown excellence in her field.
“My dream for my country Botswana is to have a well-established, operationalized national public health laboratory,” she says. “I think we have capacity in terms of human resources, in terms of infrastructure. What we need now is the drive to move towards excellence. You know, embracing the science as it is and technology as it comes.”
Elkoz Station (Wastewater station), Khartoum, Sudan. Jan 10, 2021: environmental surveillance collectors pouring wastewater for testing.
The Global Commission for the Certification of Poliomyelitis Eradication (GCC) met recently in Amman, Jordan, to review progress towards interrupting wild poliovirus type 1 (WPV1) transmission in polio-endemic Pakistan and Afghanistan, implementation of the Global Surveillance Action Plan, and to hear from the six regional certification commissions on current regional priorities and issues.
‘Deep-dive’ sessions on both endemic countries, focusing on epidemiology, virology, immunization coverage and surveillance, were valuable opportunities for the global body to be updated on current challenges being faced by Pakistan and Afghanistan country teams in achieving zero polio. The GCC commended the national programmes for their conduct of high-quality activities in the face of political instability, insecurity and other operational barriers, and concluded that 2023 presents a vital opportunity to finally stop transmission of WPV1.
On detection of poliovirus, the GCC noted the progress towards implementation of the GPEI Global Surveillance Action Plan (GPSAP) but raised concerns over shortcomings in surveillance performance, particularly the timeliness of detection and quality of environmental surveillance in some localities. The Commission reiterated the importance of environmental surveillance as a supplement to AFP surveillance, and while recognizing that its utility varies depending on ground realities, recommended that further analysis be conducted into ES system performance and for updates to be provided to the group on a biannual basis.
More broadly, the GCC stressed a need for greater confidence in surveillance systems worldwide, and particularly in the endemic countries, to detect transmission within areas and populations of greatest risk, such as those with substantial gaps in population immunity, high risk mobile groups and areas that have had silent transmission of poliovirus. The GCC called for greater granularity in GPEI reporting of progress in implementing the GPSAP and flagged a need for deeper understanding of all potential gaps, including region specific issues.
“It will be the quality of poliovirus surveillance that will allow the GCC to certify the eradication of WPV1 with the highest possible level of confidence,” said Professor David Salisbury, GCC Chair.
The GCC also recommended that immune-deficient vaccine-derived poliovirus (iVDPV) surveillance continue to be developed as an important aspect of the validation of the absence of VDPV.
Lastly, the GCC commended GPEI’s continued and intensive coordination and support of the endemic country programmes, to facilitate a smooth regional certification process when WPV1 is no longer detected and recommended that polio-free regions begin to prepare for global certification of WPV1, in line with the Eastern Mediterranean’s regional certification.
The full GCC report and recommendations will be made available in the coming weeks.
The review team, comprising of experts including virologists and epidemiologists, visited Afghanistan in June, conducting a comprehensive nationwide assessment of the country’s polio surveillance system. Among their recommendations was the need to address gaps in environmental surveillance and expand the number of environmental surveillance sites in areas deemed high risk for polio, including the country’s east, southeast, south and west regions, to ensure any presence of the virus is quickly detected.
Afghanistan’s AFP surveillance system – monitoring for signs of Acute Flaccid Paralysis in children under 15 years of age – is complemented by environmental surveillance – the collection of sewage samples at designated sites to check for the presence of the virus in the community. Together, they enable the programme to detect where the virus may be circulating and, importantly, mount a timely response.
Following the review’s recommendations, three new environmental surveillance sites have now come online, bringing the total number of sites in Afghanistan to 32. One of those sites, at Pezand Pana Dafter in Nangarhar province has produced three positive environmental samples since coming online in September. The programme quickly mounted a response targeting 1.4 million children under 5 years of age in all four eastern provinces – Nangarhar, Kunar, Laghman and Nuristan.
“Surveillance is the eyes and ears of the polio programme, and environmental surveillance plays an important part in eradicating polio because it enables the programme to detect the presence of the virus,” says Dr. Khushhal Khan Zaman, who oversees polio surveillance for WHO Afghanistan. “Environmental surveillance tells us very plainly where transmission is likely happening.”
WHO guidelines stipulate that an environmental site be located in areas with substantial populations, and with flowing sewage water. In Afghanistan, sites are established in major cities and larger population centres with existing wastewater and drainage systems. Communities with mobile populations are also a focus. Samples are regularly taken and sent to a WHO-accredited polio laboratory for testing.
Afghanistan has made significant progress in interrupting transmission of the virus. From 56 children paralysed by WPV1 in 2020, so far this year there have been two cases, in Paktika and Kunar provinces. Seventeen positive environmental samples have been detected in 2022, all in the country’s east region.
Further environmental surveillance sites are planned as WHO Afghanistan continues to implement recommendations from the surveillance review.
Around the time when the Fédération Internationale de Football Association (FIFA) World Cup tournament was introduced, in 1930, children didn’t have access to polio vaccines. Additionally, systems to search for polio symptoms in children were most likely weak across the world. This scenario has changed now.
To prepare for an estimated 1.2 million football fans congregating in Qatar to watch the World Cup tournament, the Government of Qatar took several measures to mitigate risks associated with the spread of diseases, including polio. As part of these interventions, the country requested the World Health Organization (WHO) for technical support to assess and improve surveillance for polio.
Taking stock of existing disease surveillance systems
To kick off these efforts, after months of joint planning and coordination, a team from WHO’s Eastern Mediterranean Region (EMR) visited Qatar at the end of September 2022 to conduct an elaborate review of the surveillance system for acute flaccid paralysis (AFP). They examined activities at four main health care facilities − where both Qataris and visitors in the country frequently visit − to assess their contribution to AFP surveillance.
The team also conducted a virtual capacity development session for more than 200 public and private health professionals to understand the global and regional polio situation, and the importance of AFP surveillance and case reporting.
Reviewing systems to detect and respond to polio cases
On noting the recent spread of polioviruses across the world, and ease with which viruses can be transmitted, WHO sensitized officials at the Ministry of Public Health on the standard operating procedures for polio outbreaks. This includes a template to develop a national preparedness plan for a polio outbreak.
As next steps, the team conducted a Polio Outbreak Simulation Exercise (POSE), to test the level of preparedness and the blueprint of activities that should be conducted in case of an outbreak. The POSE ensures users are aware of activities to conduct within the crucial first 72 hours of confirmation of a polio outbreak. This exercise also aimed to ensure all existing tools in use are valid, and refreshed health officials’ knowledge on the different kinds of polioviruses that exist and vaccines that can be used to boost immunity.
Need to strengthen AFP case notification
One of the most highly developed countries in the EMR, Qatar has a state-of-the-art online health client database, which is used by 90 percent of health service providers. The country also uses unique codes for all residents regardless of their nationality, which helps them manage infectious disease outbreaks. Health facilities offer high quality of health care, which encourages communities’ uptake in health services. Taking this into account, the surveillance review revealed that the electronic health system in Qatar is able to track AFP cases once notified.
The country, however, faces challenges in the notification of AFP cases, largely due to the lack of a comprehensive list of diseases related to AFP in the electronic databases currently in use in health facilities and hospitals. Additionally, physicians lack awareness about AFP and case notification, which is attributed to Qatar being polio-free since 1990.
Recommendations for stronger surveillance of polio
Recommendations made by WHO to the Ministry of Public Health are aimed at developing the capacity of staff to notify AFP cases early; conduct regular active search for children with AFP, including through active surveillance visits; and execute 60-day follow up examination for AFP cases. The WHO team also advised Qatar to maintain updated and functional AFP surveillance guidelines, and a national preparedness and response plan for polio outbreaks and response.
WHO also encouraged the Ministry of Public Health to set up a system for environmental surveillance to search for polioviruses in sewage and wastewater at prime sites across the country. This would help to cast a wider net to search for any poliovirus both in visitors and communities living in the country.
Qatar plays a key role in polio eradication
The Government of Qatar is a key partner in polio eradication efforts. Qatar’s Minister of Public Health, HE Dr Hanan Mohamed Al Kuwari has been serving as the co-chair of the Regional Subcommittee for Polio Eradication and Outbreaks in the Eastern Mediterranean Region since February 2022. In this capacity,
HE Dr Al Kuwari has been instrumental in shining the spotlight on the current status of polio in the Region and efforts needed to end polio by the end of 2023.
Arrive Kabul at 9.30am, my first visit in two years and the city has lost none of its bustle.
A review team last visited here in 2016 but access was limited. Much has changed – both within Afghanistan and for polio – since then. The programme now has access across the country and the epidemiological picture has changed dramatically. In 2020, 56 children were paralysed by the virus. So far this year only one child has been paralysed giving Afghanistan its strongest chance yet of interrupting polio transmission.
Surveillance underpins the eradication of any virus. For polio, it consists of monitoring for signs of Acute Flaccid Paralysis or AFP in children under 15 years, and collecting samples of sewage, what we call environmental surveillance, to check for the presence of the virus in the community.
We’re here to apply a magnifying glass to Afghanistan’s surveillance system, to see if there’s anywhere the virus might still be hiding and recommend adjustments to make sure the system is capable of catching it.
If polio surveillance is about gathering data and documenting it meticulously, it’s even more so for a surveillance review. Our job includes checking documents and records, interviewing health workers and families of children with AFP, reviewing guidelines and standard operating procedures – checking and rechecking data.
After meetings yesterday, including briefing the National Emergency Operation Center (EOC), the operational heart of the polio programme here, I head to Herat in the country’s west where my first stop is the WHO office. I meet the polio team before moving on to the Regional EOC where we discuss the objectives of my mission. I review records before checking the cold room where vaccines are kept. There’s a corner for stool specimens that come in from the western region. Part of the process of checking children with signs of AFP is collecting stool samples that are then sent to the regional laboratory in Pakistan for testing. Reviewing the collection, storage and shipping of these samples is part of my remit as a reviewer.
Thursday 9 June
At a hospital in Herat city, I meet with the AFP focal point – a pediatrician. All major health facilities have an AFP focal point who acts as the link between the facility and the broader surveillance system. I ask him about his background, the facility’s stool handling, preparation and shipment, and the work of the hospital.
In the afternoon, I examine two children affected by AFP earlier in the year. I talk to their parents and ask them the same questions they were asked by the initial investigating surveillance officer. I do this to check the accuracy of the information collected during the original case investigation and to see if there are any discrepancies.
Friday 10 June
Friday – the only holiday of the week. I spend it at the WHO office going through documents including AFP case files and data. It’s also a good opportunity to enter all the information I collected over the previous two days into the online tool developed specifically for this review.
Saturday 11 June
We set out early to a district near the border with Iran, two hours’ drive away. First stop is a very busy Comprehensive Health Center (CHC). It’s reported six out of the eight AFP cases from this district this year. I meet with the director, doctors, nurses, and other staff. Beneath their facemasks, their smiles are beaming. They speak with pride of their clinic and, like all the health facilities I visit, it’s spotlessly clean.
In the afternoon, I meet with the community health supervisor who oversees 16 community health workers (CHWs) working in village health posts nearby. Village health posts play an important role in community-based polio surveillance. I review the curriculum and training agenda to check what information is captured.
Sunday 12 June
I spend the day in the districts surrounding Herat city. My meetings include a visit to a traditional healer who fixes broken bones among other ailments, and a CHW who is an imam at a local mosque. Both are reporting volunteers in the 46,000-strong community-based surveillance network that keeps an eye out for polio among their communities.
I visit an environmental surveillance site in Herat city. Samples are taken from sewage on a regular basis and shipped to the lab in Pakistan to determine the presence of poliovirus. I assess the site to see if it meets quality standards, check its location to make sure it’s in the right place to catch a good enough sample, the flow of the water and its appearance. I watch as trained staff from the local municipality collect a sample to determine whether the SOPs are adhered to.
Tuesday 14 June
To neighbouring Farah province, a round trip of about eight hours. At a CHC, a boy is brought in who was referred by a local faith healer. I observe the staff examine the child, and then visit the faith healer who tells me he inherited the knowledge of healing from his father and has been doing it now for over 20 years. It was heartening to hear him talk of his collaboration with the polio team for both AFP surveillance and immunization campaigns.
Wednesday 15 June
Last day in Herat city and I debrief the team in the REOC. Our flight back to Kabul departs late and we stop in Bamyan in the central highlands to collect two other passengers, including my fellow reviewer assigned to the Central Region.
The rest of the review team makes its way back to Kabul in the remaining days. We’ve all been doing the same thing – verifying, checking, interviewing, collating data. Our next task is to compile our report and provide any recommendations to the programme to make sure Afghanistan’s polio surveillance system catches every last virus, no matter where it may be hiding.
The Global Polio Eradication Initiative (GPEI) has been informed of a case of paralytic polio in an unvaccinated individual in Rockland County, New York, United States.
The US Centers for Disease Control and Prevention (CDC) are coordinating with New York State health authorities on their investigation. Initial sequencing confirmed by CDC indicates that the case is type 2 VDPV.
Following the detection, the Global Polio Laboratory Network (GPLN) has confirmed that the VDPV2 isolated from the case is genetically linked to two Sabin-like type 2 (SL2) isolates, collected from environmental samples in early June in both New York and greater Jerusalem, Israel, as well as to the recently-detected VDPV2 from environmental samples in London, UK. Further investigations – both genetic and epidemiological – are ongoing to determine possible spread of the virus and potential risk associated with these various isolates detected from different locations around the world.
It is vital that all countries, in particular those with a high volume of travel and contact with polio-affected countries and areas, strengthen surveillance in order to rapidly detect any new virus importation and to facilitate a rapid response. Countries, territories, and areas should also maintain uniformly high routine immunization coverage at the district level and at the lowest administrative level to protect children from polio and to minimize the consequences of any new virus being introduced.
Any form of poliovirus anywhere is a threat to children everywhere. It is critical that the GPEI Polio Eradication Strategy 2022-2026 is fully resourced and fully implemented everywhere, to ensure a world free of all forms of poliovirus can be achieved.
17 February 2022 As a result of ongoing disease surveillance, the Global Polio Laboratory Network (GPLN) has confirmed the presence of type 1 wild poliovirus (WPV1) in a child suffering from paralysis in Tsabango, Lilongwe, Malawi. Analysis shows that the virus is genetically linked to WPV1 that was detected in Pakistan’s Sindh province in October 2019.
The three-year-old girl in Malawi experienced onset of paralysis on 19 November 2021, and stool specimens were collected for testing on 26 and 27 November. Sequencing of the virus conducted in February by the National Institute for Communicable Diseases in South Africa and the U.S. Centers for Disease Control and Prevention confirmed this case as WPV1.
Detection of WPV1 outside the world’s two remaining endemic countries, Pakistan and Afghanistan, is a serious concern and underscores the importance of prioritizing polio immunization activities. Until polio is fully eradicated, all countries remain at risk of importation and must maintain high vaccination coverage to protect all children from polio.
The GPEI is supporting health authorities in Malawi to conduct a thorough assessment of the situation and begin urgent immunization activities in the subregion to mitigate any risk of spread. Surveillance measures are also being expanded in Malawi and neighboring countries to detect any other potential undetected transmission.
As an imported case from Pakistan, this detection does not affect the WHO African Region’s wild poliovirus-free certification status officially marked in August 2020. Malawi last recorded a case of wild poliovirus in 1992. The polio eradication programme has seen importations from endemic countries to regions that have been certified wild poliovirus-free in the past, and has moved quickly to successfully stop transmission of the virus in these areas.
Polio anywhere is a threat to children everywhere. Now is the time for all parties to recommit to ending all forms of polio for good.
The WHO African Region is expected to be certified free of wild poliovirus on 25 August 2020. Chair of the WHO’s International Health Regulations Emergency Committee and of the AFRO Regional Immunization Technical Advisory Group Helen Rees explains the current cVDPV situation in Africa and its implications ahead of regional wild polio-free certification.
Q. Fifteen countries (as of 14 August 2020) in the World Health Organization’s African region have reported cases of circulating vaccine-derived polio type 2 (cVDPV2) in 2020. The total number of outbreak countries is 16. How does that impact the region’s upcoming wild polio-free certification?
First, it’s important to clarify that cVDPV is a different virus from the wild poliovirus, and will undergo a separate process to validate its absence once wild polio has been eradicated globally.
Second, I want to underscore that the ongoing cVDPV2 outbreaks in Africa do not affect the programme’s confidence that wild polio is gone from the region. Certification is backed by extensive data and a thorough evaluation process that demonstrates wild polio transmission has been interrupted on the continent.
In Africa, an independent body of experts called the African Regional Certification Commission for polio eradication (ARCC) oversees this process by carefully reviewing country documentation and analyzing the quality of surveillance systems and immunization coverage. With this intensive monitoring of polio programmes across the continent, the ARCC is able to confirm with 100% certainty that wild polio is gone from the region.
But for the ARCC, national polio programmes and GPEI partners, the work does not end here. Stopping cVDPVs remains an urgent priority. African countries will need to strengthen their efforts to reach all children with polio vaccines to protect them from cVDPVs and any importation of wild polio from the remaining endemic countries, Pakistan and Afghanistan.
How do cVDPV outbreaks happen?Andwhy has the number of cVDPV cases in Africa increased more rapidly in the past couple years while wild cases have not?
cVDPVs can occur if not enough children receive the polio vaccine. In under-immunized populations, the live weakened virus in the oral polio vaccine (OPV) can pass between individuals and, over time, change to a form that can cause paralysis—resulting in cVDPV cases. This means that the cVDPV outbreaks we’re seeing today are revealing pockets across the continent where immunization rates are too low.
The reason for the increase in cases can be explained by low immunity to type 2 poliovirus, which causes the vast majority of cVDPV cases. This is in part due to a global vaccine switch that occurred in 2016, when countries stopped using the trivalent OPV (which protects against all three forms of polio) and replaced it with the bivalent OPV (which protects against just type 1 and 3).
The GPEI, following the advice of the Strategic Advisory Group of Experts, decided to make this vaccine switch based on extensive evidence that showed it would decrease the number of cVDPV outbreaks. However, immunity to type 2 poliovirus was lower than predicated at the time of the switch and so there were actually more cVDPV2 outbreaks. In response to the cVDPV2 outbreaks monovalent oral polio vaccine type 2 (mOPV2) has been used to interrupt transmission. But with increasing numbers of children who do not have type 2 immunity, mOPV2 vaccines have had to be used longer and in larger quantities than was initially anticipated. This larger and more extensive use of mOPV2 vaccines has seeded new outbreaks especially in areas of low immunization coverage and on the borders of outbreak response zones.
All this said, mOPV2 is an effective tool to stop cVDPV outbreaks if children are properly immunized.
If cVDPV outbreaks can only affect under-immunized communities, doesn’t the increasing number of outbreaks indicate that polio immunity levels are too low across the region? Why were countries able to stop wild polio then?
For years, the wild poliovirus has only existed in a small area on the continent. Nigeria reported its last case of paralysis due to wild polio four years ago, but most other countries haven’t seen a wild polio case in quite some time.
Across the continent, population immunity levels to type 1 polio (the only type of wild polio that remains in the world) and surveillance networks have continued to protect against any wild polio importation from remaining wild polio endemic countries.
However, the increasing number of cVDPV outbreaks across Africa is a reminder that countries cannot afford to let their guard down, and must continue reaching every child with the polio vaccine.
What is the programme doing to address cVDPVs in Africa?
The same tactics that stop wild polio can be used to stop cVDPVs – high vaccination coverage and strong surveillance. The polio programme in Africa has proven experience and strategies to address cVDPV outbreaks. But we know that we cannot rely only on existing tactics, which is why the programme is innovating and adapting its strategies to address the challenge of cVDPVs specifically.
In early 2020, the GPEI released a comprehensive new strategy to stop cVDPV outbreaks currently affecting countries in Africa, Asia and the Middle East.
This includes revising outbreak response standard operating procedures to improve response time, doubling the size of the African Rapid Response Team, forming a global Rapid Response Team and prioritizing the GPEI’s ground presence in high-risk areas.
To raise immunization coverage, the GPEI partners – including Gavi, the Vaccine Alliance – are working to build and strengthen immunization systems in at-risk countries and expand routine immunization with the inactivated polio vaccine (IPV).
The strategy also includes the development of an additional tool to help stop cVDPV2 outbreaks – novel oral polio vaccine type 2 (nOPV2). nOPV2 is a modified version of the existing mOPV2 used to respond to cVDPV2 outbreaks that is less likely to change to a form that can cause paralysis.
The GPEI is confident that with strengthened commitment from country governments and full implementation of the tactics laid out in its strategy, cVDPVs can be wiped out across Africa.
Has COVID-19 affected the programme’s ability to stop cVDPV outbreaks in the region?
The recent pause in house-to-house polio campaigns to help control the spread of COVID-19 is expected to increase cVDPV transmission across affected countries.
The GPEI is taking a number of steps to get back on track. Even while campaigns were paused, surveillance activities continued so that as immunization activities ramp up the programme can target campaigns in areas that are most at risk.
The GPEI recently recommended that all countries with active polio transmission resume vaccination activities as soon as it is safe to do so, in line with WHO and national COVID-19 guidance. Burkina Faso and Angola were among the first countries to start implementing cVDPV outbreak response campaigns after the pause.
These campaigns are closely following safety guidelines and social distancing measures to protect communities and health workers against COVID-19. Measures including the use of masks and gloves, frequent handwashing and no-touch vaccination.
COVID-19 undoubtedly represents a setback for polio eradication, but not the first one the programme has faced. The GPEI and African countries’ national polio programmes are committed to ensuring that countries are ready to tackle the remaining challenge of cVDPVs and to recover lost ground once polio activities can safely ramp up.
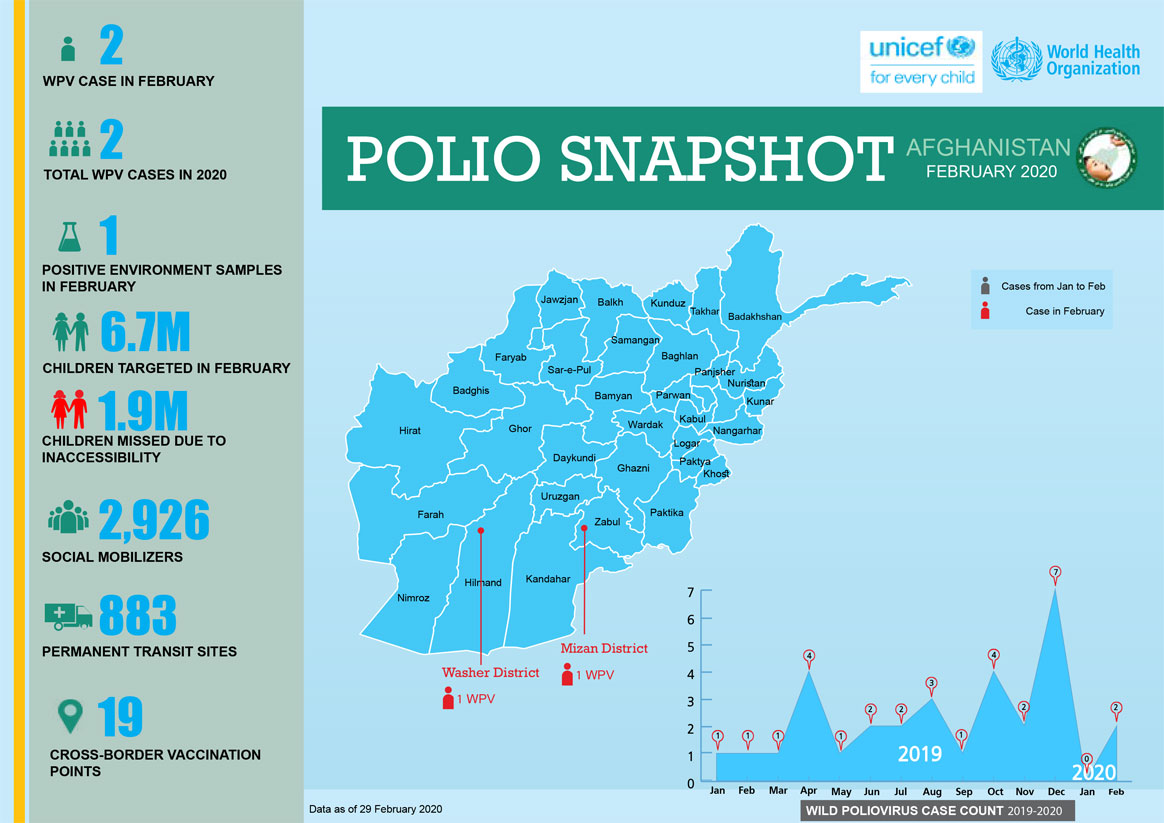
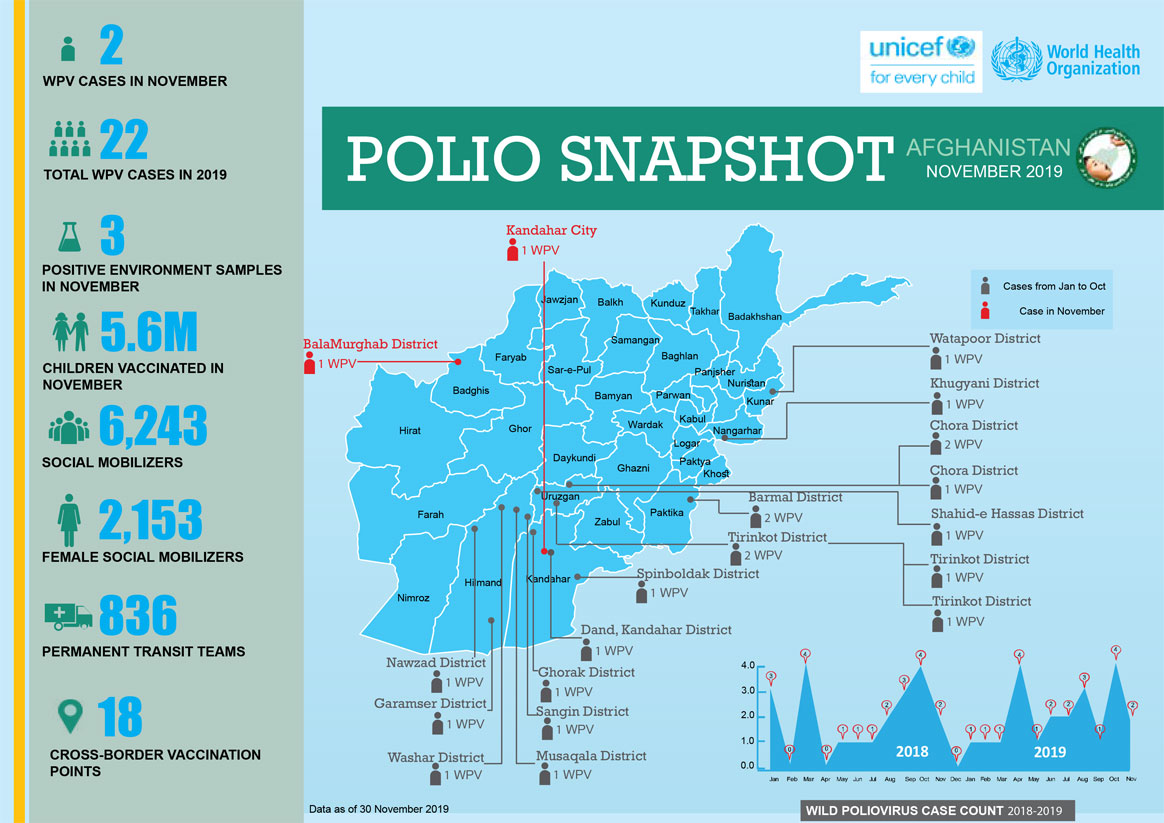
In February:
2 cases of wild poliovirus were reported
6.7 million children were vaccinated.
Permanent transit teams vaccinated 1,800,000 children and cross-border teams vaccinated 124, 309 children
Sudan borders a number of countries facing outbreaks of circulating vaccine-derived poliovirus, including Chad and the Central African Republic (CAR) to the west, and Ethiopia and Somalia to the east. Population movements between these countries increase the risk of importation of polio to Sudan. The World Health Organization and national health authorities in Sudan are scaling up efforts to reduce the risk of poliovirus transmission to the country.
To prevent a possible outbreak, health authorities have been working amidst immense operational challenges to carry out vaccination campaigns and strengthen disease surveillance. Public health teams in Sudan and CAR are collaborating to share details of vaccinated refugee children with their country of origin, and exchange information on upcoming supplementary immunization activities and reported cases of Acute Flaccid Paralysis.
Sudan was declared free of wild poliovirus in 2015, but remains at considerable risk for poliovirus importation or a VDPV outbreak. Much of the risk is shaped by Sudan’s unique population dynamics, and by the devastating effect of population movement, conflict and instability affecting routine immunization. Additionally, nomads, who account for around 10% of Sudan’s population, regularly move across borders to graze animals in Chad and CAR.
Over 8 million children under the age of five are estimated to live in Sudan – an age group considered to be most vulnerable to contracting and being paralyzed by poliovirus. Sudan also has large numbers of internally displaced people and refugees, many in the areas of the country with the lowest levels of routine immunization, such as the Darfur region.
In September and October 2019, states on the border between Sudan and CAR implemented accelerated routine immunization to provide children with coverage against a variety of vaccine-preventable diseases. Teams conducted reviews of vaccination facilities and posts in border areas, and orientation sessions were held in healthcare settings to reinforce reporting cases of Acute Flaccid Paralysis. Children received oral polio vaccine, pentavalent vaccine, and inactivated polio vaccine. Initial data from the campaigns suggests a spike in coverage, with teams reaching many children previously unprotected.
The nomads of the Lake Chad Basin account for 3%–5% of the population and are one of the most underserved communities when it comes to health.
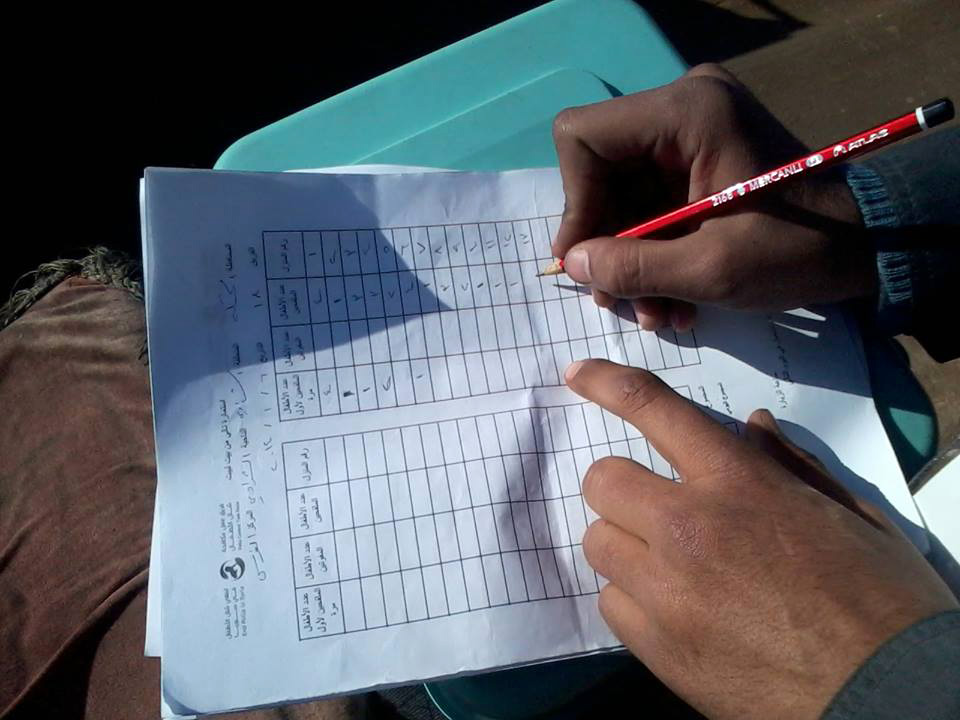
When Chad had to respond to the detection of wild poliovirus in Nigeria in 2016, it was crucial to vaccinate nomadic children. The World Health Organization, the United States Centers for Disease Control and Prevention and partners created a database of population numbers, movements, and immunization records. ‘Lake Chad response teams’, each with four specialists – an epidemiologist, a social mobilizer, a vaccinator and a data recorder – fanned out, data in hand, to reach every nomadic child with polio vaccines.
Often teams began by speaking to nomads in a market or on a road and then asking to follow them to their temporary camp. The Lake Chad Basin covers almost 8% of the African continent and trying to find groups amongst the vast expanse of semi-arid savannah was almost impossible without this kind of time-consuming work.
Upon arriving in a camp, the social mobilizer in each response team explained to family elders and parents the purpose of the vaccination and the benefits for their children. The response teams asked for permission to begin vaccination.
“They see themselves as neglected in society,” explains Ajiri Okpure Atagbaza, a GIS consultant in the WHO Regional Office for Africa Geographic Information System Centre, who spent three years as part of the Chad response team working with nomads. “When you came with aid, they welcomed you. As long as you spoke their language, they were open to it.”
Children received all immunizations for their age alongside polio vaccine, as part of an integrated approach to health delivery. The parents were given an immunization card recording which vaccines had been administered.
Each team carried a smartphone application used to capture the locations of the nomadic camps, the results of acute flaccid paralysis case surveillance, and information gained through conversations with the community, such as how long they had been in their current location, previous and future camp locations, the population size and vaccination rates. This information was uploaded to bolster the database to help plan future health services.
From April to August 2019, the Lake Chad response teams reached 1067 nomad groups in 17 districts in Chad alone and vaccinated more than 27,000 children. Across all five countries making up the Basin, more than 40,000 children in 3451 nomadic camps in 62 high-risk districts received their routine immunizations, including protection against polio. The information recorded during these activities will be used in routine immunization planning to ensure that children continue to receive all their vaccinations according to the schedule.
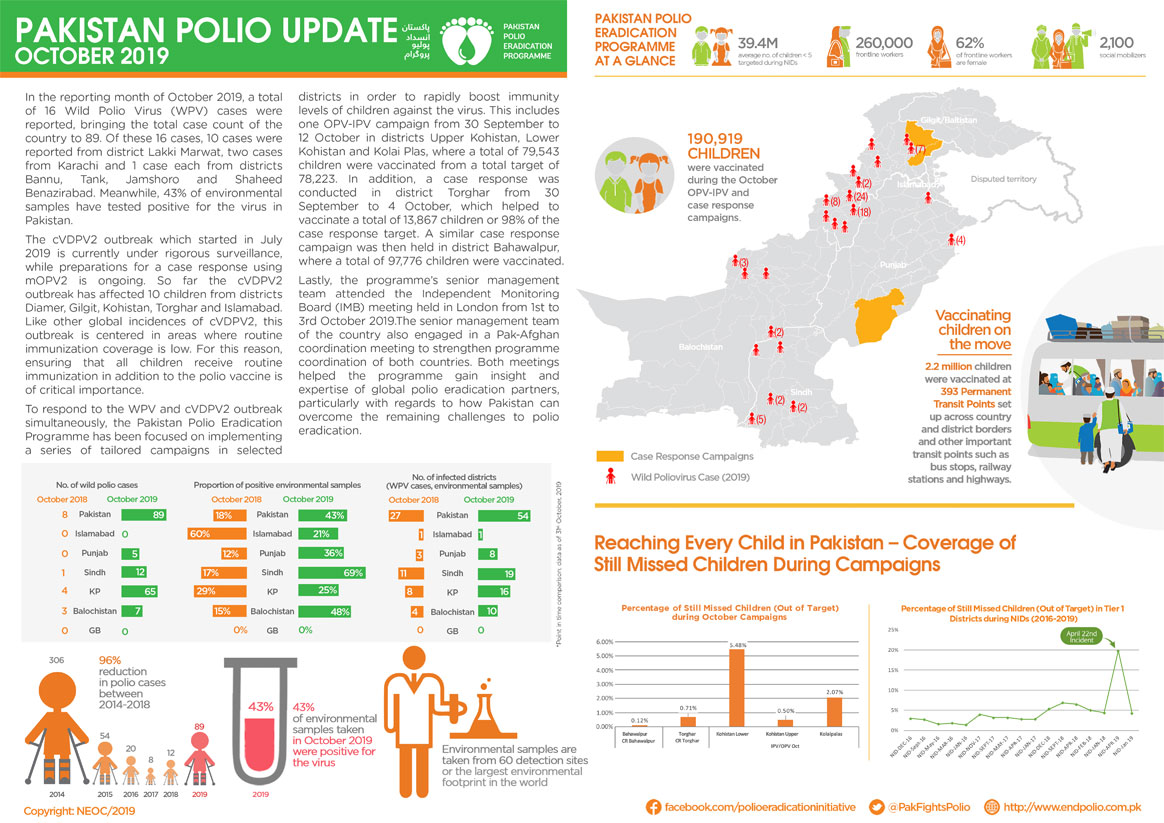
In October
190,909 million children were vaccinated during the October Case Response Campaigns.
2.2 million children were vaccinated at 377 Permanent Transit Points.
In Jere Local Government Area, in Borno State, Nigeria, a team of male surveillance officers have been dispatched to look for the poliovirus.
They make a first stop at the home of Hajiya Liman Bello, a mother of three and a housewife.
“Who are all of you and what do you want?” Hajiya asks.
“We are health workers please. We need to collect stool samples from your children as there has been a case of Acute Flaccid Paralysis (AFP) in this area”, they reply.
Hajiya isn’t comfortable with the idea of a male health worker handling stool sample collection for her children. She requests that surveillance officers return with a female colleague if they wish to go ahead.
Recognising the links between gender and disease surveillance
In line with the Global Polio Eradication Initiative’s gender strategy, Nigeria’s polio programme has been quantifying the gender aspect of its work. While women make up 95% of frontline workers delivering polio vaccines, a 2017 study conducted by the World Health Organization found there were significantly more men than women engaged in polio surveillance activities in Nigeria.
In 2016 there were 29 men employed in Nigeria as state epidemiologists compared with just eight women doing the same job; 23 male state disease surveillance and notification officers (DSNOs) compared with 14 women, and at a Local Government level, 609 male DSNOs versus 218 female.
The results of the study prompted reflection by programme staff. Gender, like other factors such as age, education and socioeconomic status, is an important determinant of health-seeking behaviour and outcomes. In the case of disease surveillance officers, gender diversity amongst personnel helps the programme build trust and acceptance amongst parents.
“I believe gender strongly influences disease surveillance and access to immunization services,” says Dr Kabir Yusuof, a health worker who has worked with the Nigerian Government polio programme for over ten years.
“Nigeria is generally a culturally attuned country. There are some communities where men only feel comfortable with female health workers, especially when it comes to house-to-house outreach and matters of maternal health. For this reason, I believe the role of women in both polio surveillance and response cannot be overlooked.”
Surprisingly, the report showed there were more men than women working as surveillance focal points in health facilities in northern zones of Nigeria, compared to the south. Using gender-disaggregated data helped the programme see where things need to change.
“WHO advocates for breaking…illusions that women cannot ‘fit in’ when it comes to disease surveillance practice,” says Dr Fiona Braka, Team Lead for the Expanded Programme on Immunization at WHO Nigeria.
Polio eradication was the first disease programme at the World Health Organization to develop a dedicated gender strategy. The Nigeria AFP surveillance gender study had never been done before and has helped lay the groundwork for further examination of the programme through a gender lens. The authors of the study found that the number of AFP cases detected in boys and girls was similar, as were polio vaccination rates.
Dr Braka observes, “Integrating or mainstreaming gender into all facets of socio-economic life is key to tackling gender inequalities.”
Health workers and community volunteers in remote and security-compromised areas across ten African countries now rely on an SMS-based application to ferret out any possible poliovirus hiding in their midst.
The application is called AVADAR, short for “auto-visual AFP detection and reporting”, with AFP referring to acute flaccid paralysis, which is the main visible clinical symptom of poliomyelitis. AVADAR is an SMS-based mobile application used for reporting, monitoring and surveillance of poliovirus. It was developed in 2016 by the World Health Organization (WHO), in collaboration with the Bill & Melinda Gates Foundation and the Swiss software company Novel-T, to ensure that every case of wild poliovirus is detected.
On a weekly basis, the health workers and volunteers in selected hard-to-reach districts use the AVADAR application to report whether they have noticed any child with paralysis of a limb. The districts are selected based on being deemed high risk yet having the sufficient telecommunications infrastructure that allows the health workers and community volunteers to communicate with the investigations team.
“In the last mile of polio eradication, we are not sparing any resources to reach a polio-free world. That is why we developed the AVADAR app,” says Dr Pascal Mkanda, WHO Regional Coordinator of the Polio Eradication Programme for Africa.
In the WHO African Region, no outbreaks of wild poliovirus have been detected since 2016, when the last case was found in Nigeria’s Borno State. This brings the region closer towards being certified free of wild poliovirus in 2020.
Health workers and community volunteers use AVADAR to recognize and report cases of acute flaccid paralysis, which is the sudden onset of paralysis or weakness in any part of the body that can be caused by polio, among children younger than 15 years. Acute flaccid paralysis could be caused by other diseases than poliomyelitis.
“Polio eradication requires that the surveillance system is sensitive enough to detect all acute flaccid paralysis cases -regardless of the disease behind it- and that such cases are promptly reported and investigated by disease surveillance personnel. This system starts at the community level,” Dr Mkanda adds.
Health workers and community volunteers first received training in workshops on how to use AVADAR and then they were each handed a smartphone with the application installed. On a weekly basis, the app sends them video reminders illustrating acute flaccid paralysis cases. The app then asks: “Have you seen a child with weakness of the legs or arms that you have not previously reported?” They then select between yes or no. If yes, the health workers and community volunteers input extra information about the case, such as the child’s name, date of onset of symptoms and geographic information.
Once the health worker presses the “send” button, a text message is sent to a system that triggers the sending of an SMS to the government and a WHO team that will investigate the case.
“In the AVADAR training workshops, we realized that some health workers and the majority of volunteers do not know the implications of acute flaccid paralysis and are unable to accurately identify such cases within their communities. The weekly AVADAR reminder videos helped improve that significantly,” says Dr Godwin Akpan, WHO Regional Polio Data Manager for Africa.
Dr Godwin is part of the team behind the innovation of the AVADAR application and trains health workers and community members on its use.
AVADAR was first piloted in Nigeria in 2016 and has been rolled out since 2017 in 99 districts of ten African countries: Burkina Faso, Cameroon, Chad, Democratic Republic of the Congo, Liberia, Mali, Niger, Nigeria, Sierra Leone and South Sudan.
As of October 2019, AVADAR has detected 1019 confirmed acute flaccid paralysis cases after health workers and community volunteers sent out 25,747 alerts through the application. None of those cases were polio cases. This marks a significant enhancement to the existing surveillance system that faces difficulties in remote and high-risk areas.
“Innovation and new technologies are our hope to finally make the feat of eradicating polio a reality. Thanks to the Global Polio Eradication Initiative, today, we are closer than ever to eradicating polio,” concludes Dr Mkanda.
Environmental surveillance teams in Mogadishu access the underground closed drainage system to collect sewage waste water samples, which they package and send to the laboratory for testing. If poliovirus is identified in a sample, epidemiologists know that the disease is likely to be circulating amongst the community whose sewage drains into that part of the system. This process is called environmental surveillance and is one of the most important tools for the polio programme to help detect poliovirus.
Vaccinating every child and conducting disease surveillance to know where the poliovirus is circulating are key strategies to end the outbreak. Low immunization coverage has led to an outbreak of vaccine-derived poliovirus in Somalia. This can occur in places where not enough children have received their full vaccine doses.
The teams must follow best practice to collect samples, to ensure that any poliovirus present can be detected.
Click through this photo gallery to learn more about the sample collection process.
Mohamed Sharif Mohamed, Regional Polio Eradication Officer for Banadir, is responsible for organizing the collection of waste water samples at two sites in Mogadishu.
He explains, “Environmental surveillance was established in September 2017, when the outbreak of vaccine-derived poliovirus occurred.”
So far in 2019, 36 samples have been collected from four sites in the city as part of this important initiative.
First, Mohamed Sharif’s team put on face masks, aprons, and gloves. They are collecting untreated sewage waste water, so it’s crucial that they wear protective clothing to protect themselves from bacteria and viruses that they may encounter during their work.
Their next task is to detect the atmospheric temperature of the site, and record this on the lab request form.
The officers try to collect a high-quality sample from a pipe with running waste water. The sample must be free of contaminants, such as detergent liquids or rubbish, which could kill the virus before it is detected.
Mohamed Sharif explains that collecting a high-quality sample can be a challenge in Mogadishu, “The sewage system is old and poorly maintained. Often, rubbish is visible. Despite this, we try our best.”
Once the sample is collected, it is drained into a secure screw-cap container, which is sealed, cleaned with liquid bleach, and labelled with a unique ID code.
The ID code references this specific environmental collection site.
“Mogadishu is the first region in the country to establish environmental surveillance for polio,” Mohamed Sharif says. “The community, Ministry of Health, and the Mogadishu Municipality are aware of the hard work we are doing.”
The sample is put into a cool box for transportation to the WHO office. From there, it will be immediately flown to Kenya Medical Research Institute (KEMRI) in Nairobi, where there is a specialized poliovirus laboratory. This lab tests samples from countries across the Horn of Africa.
The sample should be kept at 4°c throughout the four-hour journey to the laboratory. This is known as the ‘reverse cold chain’ and prevents the virus deteriorating during transportation.
Packing a sample from Waberi District Site ready for transportation to the lab
Back at the office, the sample container is sealed in a plastic zip lock bag, and paperwork is completed. Then the sample is transported, surrounded by fresh icepacks, to Nairobi.
At the laboratory, a highly trained technician will analyse the sample for viruses.
Staff in Somalia follow up the results with the laboratory two weeks after the sample arrives at the lab.
Carrying a sample collected from Egyptian Hospital site
Mohamed Sharif explains what motivates him to continue this challenging work: “It is our hope that in future, when polio eradication is achieved, our names will be written in the offices of the Eastern Mediterranean region of the World Health Organization.”
“We will be part of the legacy of polio-free Somalia.”
From the epidemics in the 1950s to the 1000 cases per day in the 1980s, polio’s devastation has seeped across generations. That is, until Global Polio Eradication Initiative and anchoring partners, Rotary International, WHO, UNICEF, CDC, and most recently, the Bill & Melinda Gates Foundation, united efforts and resources to develop a comprehensive polio eradication infrastructure.
Ranging from cutting edge research to dedicated laboratories to community engagement to sewage sampling, the polio infrastructure is as widespread as it is comprehensive. With presence in over 200 countries, the polio programme is second to none, making it one of the largest public-private health partnerships in history.
While the polio eradication infrastructure helps get us closer to a polio-free world, did you know that it is also used to fight and protect against other diseases, too? Here are five examples of the polio infrastructure at work:
The cold chain
The Oral Polio Vaccine (OPV) requires constant refrigeration and vaccine must be kept cool between 2-8 degrees, or it risks losing its effectiveness. This is no easy task in countries and areas where electricity is either unavailable or unreliable.
So, the programme developed what is known as a cold chain system — made up of freezers, refrigerators, and cold boxes — to allow polio workers to store the vaccine and transport it over long distances in extremely hot weather. In Pakistan, a measles immunization program now relies on the same system. With the help of the cold chain, Sindh province recently reached its goal of immunizing more than 7.3 million children against measles.
A critical component in immunizing more children against polio, especially in remote regions, is microplanning. A microplan allows health workers to identify priority communities, address potential barriers, and develop a plan for a successful immunization campaigns.
The workers collect as many details as possible to help them reach and vaccinate all the children. This strategy has helped keep India polio-free for five years. Now the Mewat district of India is using microplanning to increase its rates of vaccination against measles and rubella.
Surveillance
The polio surveillance system helps detect new cases of polio and determines where and how these cases originated. Environmental surveillance, which involves testing sewage or other environmental samples for the presence of poliovirus, helps workers confirm polio cases in the absence of symptoms like acute flaccid paralysis (AFP).
In Borno state in Nigeria, the AFP surveillance system is now being used to find people with symptoms of yellow fever and was one of many tactics used during a 2018 yellow fever outbreak that resulted in the vaccination of 8 million people.
Contact tracing
Since polio is a transmittable disease, health workers use contact tracing to learn who has come in contact with people who might be infected. Contact tracing was also critical to containing an Ebola outbreak in Nigeria in 2014. When a traveller from Liberia was diagnosed with Ebola, Nigerian officials were able to quickly trace and isolate the traveller’s contacts, helping prevent the disease from spreading further.
An important part of the polio infrastructure that Rotary and its partners have built is the emergency operations centres network. These centres provide a centralized location where health workers and government officials can work collaboratively and generate a faster, more effective emergency response. The emergency operations centre in Lagos, Nigeria, which was originally set up to address polio, was adapted to handle Ebola, and it ultimately helped the country respond quickly to an Ebola outbreak. Only 19 Ebola cases were reported, and the country was declared Ebola-free within three months.
Amidst a poliovirus outbreak in Papua New Guinea, legions of women health workers and leaders are playing a critical role in ensuring children are fully protected from lifelong paralysis. In the current emergency outbreak response, women have emerged as a strong, reliable, and a decisive group that continue to administer key services in the outbreak response implementation. From medical doctors to surveillance officers to community mobilizers to health workers, women are active and present on all fronts.
World Immunization Week—celebrated in the last week of April— aims to encourage the use of vaccines as one of the safest methods to protect against diseases, including poliovirus. This year’s theme – Protected Together: Vaccines Work! – highlights “heroes” who are ensuring that people of all ages, all across the world are protected through vaccines. Women on the frontlines of the outbreak response in Papua New Guinea are a fitting example who continue to inspire the public health community across the world.
Here is a roundup of some of the extraordinary vaccine “heroes”:
Dr Fiona Kupe is a Paediatric Medical Officer at the Gerehu General Hospital in the National Capital District, Papua New Guinea. She is, in effect, a one (wo)man army as she dons multiple hats in the polio eradication efforts in her home country by searching for children with acute-flaccid paralysis (AFP) at Port Moresby General Hospital and Gerehu General Hospital. She also leads the mapping of communities – or microplanning – for all Supplementary Immunization Activities (SIAs) across three districts.
Along with that, she finds time to train vaccinators and community volunteers, all the while carrying out her clinical duties as a child specialist.
“As a paediatric doctor and a mother…every day, I keep (my) passion alive to overcome challenges and basically to do everything I can to check on children’s vaccination status whenever they come to see me for check-up. As a mother, I know that vaccines save lives. I want my child to survive with good health and I would definitely want the same for all the mothers and children I see.”
Melanie Serei
Seen most days with her trusty pet dog by her side, Melanie works in one of the most challenging areas for immunization activities as a health worker in a remote village of Terapo in Kerema, Gulf province. Geographical inaccessibility aside, Melanie constantly juggles issues of insecurity, violence and community vaccine hesitancy. But, she tries every single day to overcome barriers in her mission to reach every last child with the life-saving polio vaccination.
Building community trust and demand for vaccination were considered key tenets in the risk communication for the polio outbreak response. Melanie successfully carried out door-to-door checks on all the children in the village. Thanks to her diligence, she was quickly able to notice polio symptoms in a child that allowed adequate and rapid actions.
Dr Winnie Sadua
Working as a paediatrician in Angau Memorial General Hospital in Morobe province, Dr Winnie treats one very special patient: six-year-old Gafo—the first reported case of polio in PNG in over 18 years, triggering a national outbreak emergency.
Since his diagnosis, Gafo has gone on to become somewhat of a celebrity, a symbol of hope, and a staunch advocate for polio eradication. Through timely treatment and physiotherapy by Dr Winnie, Gafo can now walk with his signature gait. He is now healthy and excited to start school next year.
With all the patients that come to her, Dr Winnie makes sure to remind all the parents to take heed from Gafo’s case and get their children vaccinated.
After concerted efforts spanning decades, polio eradication efforts are in the homestretch and experts are advising how to fast-track the last mile.
The SAGE convened in Geneva from 2-4 April 2019 to discuss all things related to vaccines and immunizations, including poliovirus and the global eradication efforts around it. SAGE reviewed the latest global polio epidemiology, the new Global Polio Eradication Endgame Strategy 2019-2023, and what the post-eradication world could look like.
Double down and escalate the fight to end wild poliovirus
While SAGE noted the achievements and the progress of the Global Polio Eradication Initiative—reducing the incidence of polio by 99%, absence of wild polio virus type 3 cases, and evidence of Nigeria being wild poliovirus free for over two years—the group displayed cautious optimism about meeting the timeline set out for global eradication of wild poliovirus.
The remaining challenges to fill vaccination coverage gaps—including restricted access, socio-political challenges, and large mobile populations—complicate the efforts to rid the world of poliovirus. However, the GPEI has developed a clear-cut five- year plan to secure a decisive win, the GPEI Polio Endgame Strategy 2019-2023, developed in broad consultation with stakeholders, including SAGE members.
Inactivated Polio Vaccine (IPV)—progress in roll-out continues
From the public health standpoint, Inactivated Polio Vaccine (IPV) can be used indefinitely even after polio eradication. As of April 2019, all 33 countries which had not yet introduced IPV into their routine immunization activities have now done so.
The projected IPV supply is thought to be sufficient enough for the introduction of a two-dose IPV schedule in all countries by 2022, and to catch-up all children missed due to earlier supply shortages, by 2020/2021.
Guidelines Endorsed
As per SAGE recommendations made in October 2016, GPEI developed guidelines for poliovirus surveillance among persons with primary immunodeficiency. After reviewing the guidelines, the SAGE endorsed the guidelines for implementation in high priority countries.
The meeting report will be published in the WHO Weekly Epidemiological Record by May 2019.
The Strategic Advisory Group of Experts (SAGE) on Immunization was established by the Director-General of the World Health Organization in 1999 to provide guidance on the work of WHO. SAGE is the principal advisory group to WHO for vaccines and immunization. It is charged with advising WHO on overall global policies and strategies, ranging from vaccines and technology, research and development, to delivery of immunization and its linkages with other health interventions. SAGE is concerned not just with childhood vaccines and immunization, but all vaccine-preventable diseases.
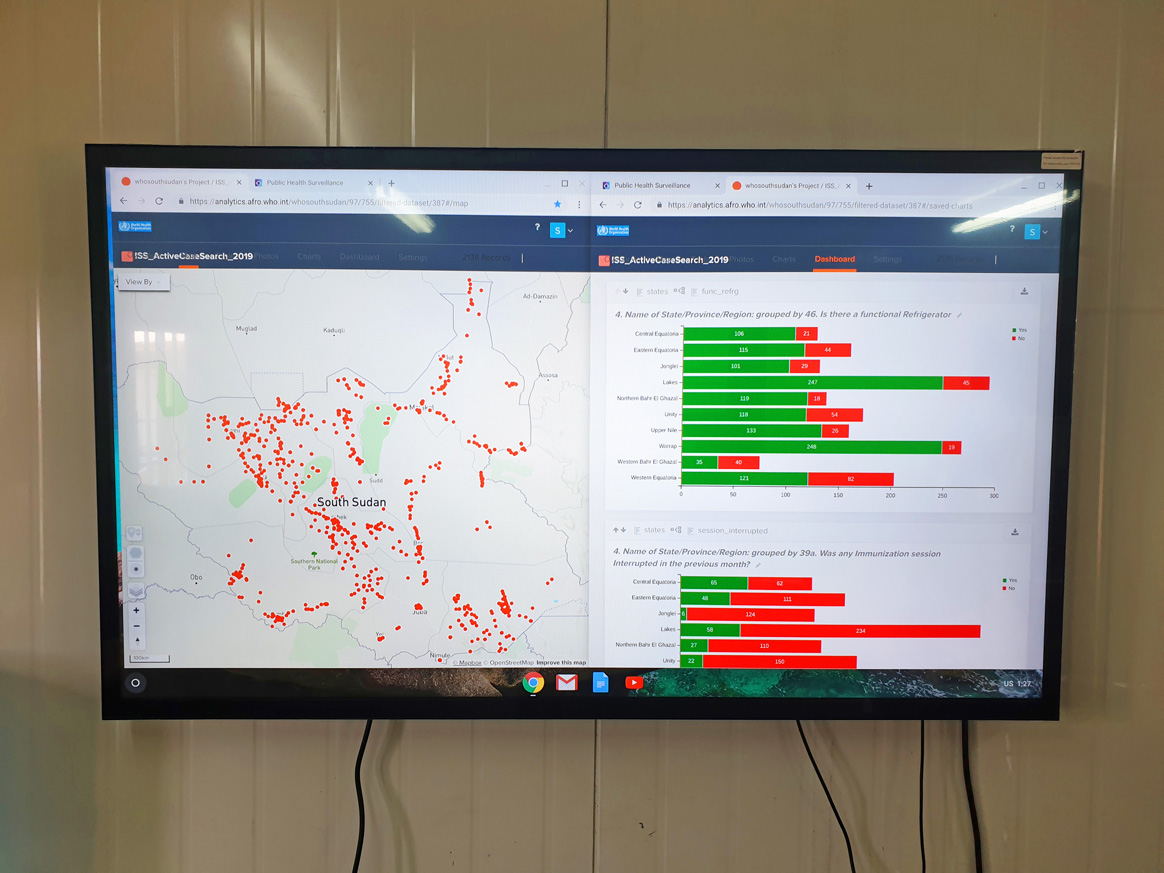
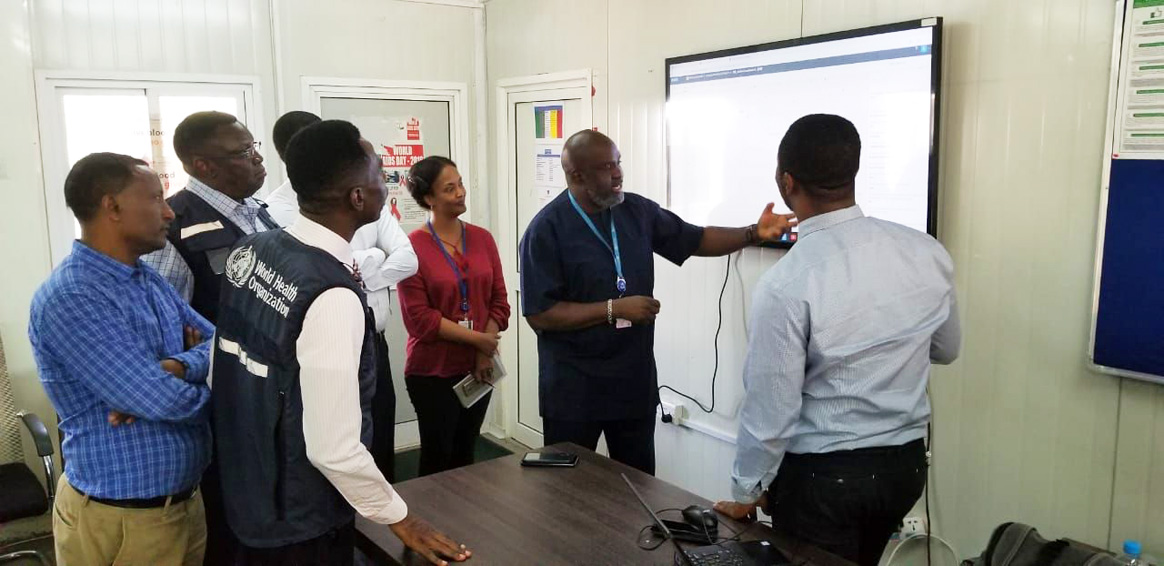
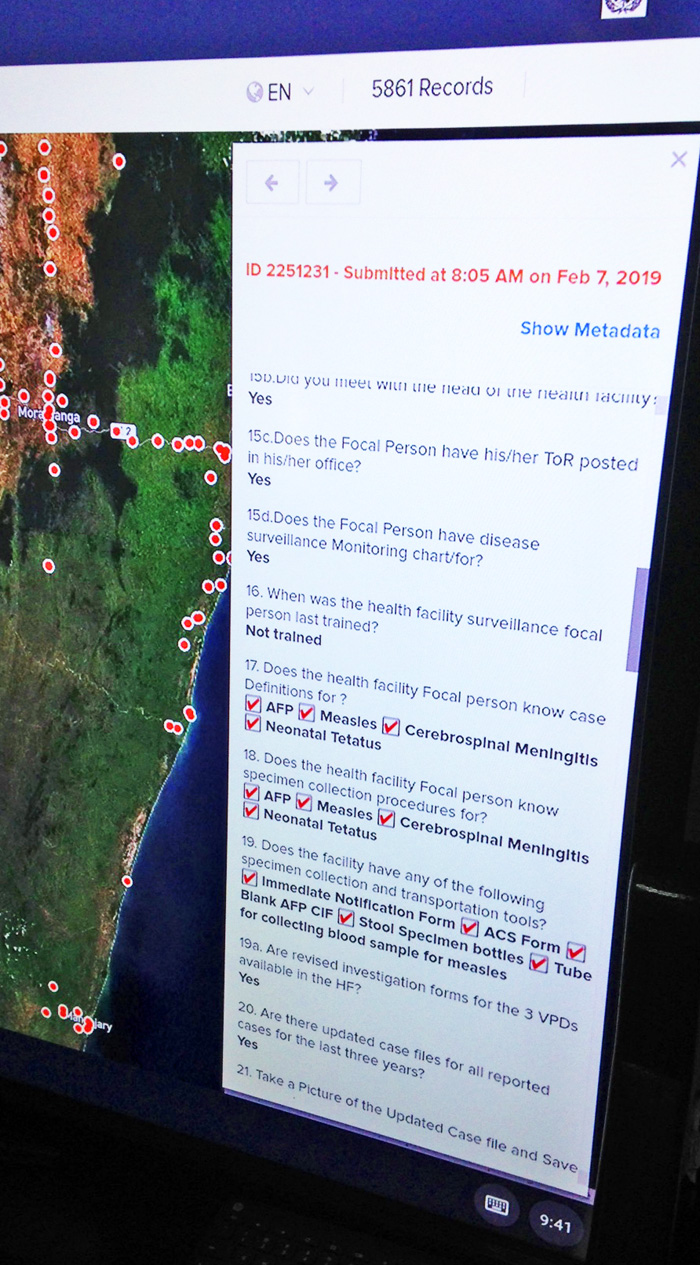
In a control room at the World Health Organization (WHO) Regional Office for Africa in Brazzaville, the smart screen projects the South Sudan map with a scattering of red dots—and even more popping up every now and then. These red dots are geo-coded locations for every healthcare facility being visited by surveillance officers to document active case search in real-time as it happens.
By simply using an application on their smart phones, the surveillance officers send their reports, even without internet connection, to the centrally generated map. Here in the control room, public health experts can quickly analyze data, visualize surveillance gaps, and conduct active case searches for priority diseases and routine immunization assessments at health facility levels. This is a game changer.
“Since the advent of the mobile-based surveillance, it has made it possible to prioritize areas and the required interventions for immunization and surveillance,”, says Dr Atem Anyuon, Director General of the Primary Health Care Ministry of Health South Sudan. He also said that other stakeholders that support the EPI programme would have access and utilization of the mobile technology.
Bridging surveillance gaps through touch screens
Data collected by health workers and community informants from the field is aggregated on database servers, and then displayed on touch interactive screens. With just a touch, maps can be viewed, and charts and dashboards of data streaming in from the field can also be monitored.
Explaining the innovation, WHO Representative, Dr Olushayo Olu says, “Interacting with real-time data through the smart visualization screens helped us recognize gaps in surveillance and intuitively navigate the interactive maps of South Sudan”. Dr. Olu is optimistic that the platform will help inform actions to improve and support surveillance and other primary health services in the country.
Progress towards certification standard documentation
In South Sudan, the technology has made clear where there are gaps in surveillance of Acute Flaccid Paralysis (AFP) – a symptom of polio – in hinterlands without internet. It also makes it easier and more transparent for staff to report what they are doing. . One of the achievements for South Sudan has been the active identification of over 6,000 cases of priority diseases across all the counties, with 85% of the AFP cases validated through geo-coordinates.
Cutting cost of active surveillance
“For me, my enthusiasm about innovating on this has been the fact that we can collect data with geographic information in places that do not have any form of network coverage and it sends the information whenever the health worker gets an internet source”, Mr Godwin Akpan, Data Management Officer of the Regional Office for Africa says.
Akpan stresses that “There are the exciting possibilities of country teams having the freedom to slice and dice the data with various analytics on the smart screen; appropriate technology hitherto used for weather analyses by mega news conglomerates is being harnessed and is now available for use by countries in the African region – a first of its kind built around open source technologies at no recurrent cost except for the hardware.”
With the interactive smart screens, the Ministry of Health and WHO can now interactively analyze data from AVADAR (Auto visual AFP detection and Reporting), Esurv (electronic Surveillance), Immunization Campaign Monitoring, Mortality monitoring as well as the ‘Lots Quality Assurance’ survey.
The initiative is facilitated by the WHO Regional Office for Africa, with support from the Bill & Melinda Gates Foundation.
On 15 March 2019 in Islamabad, representatives from the Embassy of Japan and the Japan International Cooperation Agency (JICA) were given a general update on the progress of the Polio Regional Lab and the surveillance network. Thanks to Japan’s funding, 70% of the latest molecular biology equipment has been procured, installed and made operational. JICA representatives also toured the facility and the works in process.
The Government of Japan through JICA is a long-standing and committed donor to the polio eradication efforts by funding initiatives and broader immunization activities in Pakistan since 1996.
As a part of its more recent commitment, JICA is supporting Pakistan in strengthening disease surveillance through a state-of-the-art equipment of the Regional Reference Laboratory at the National Institute of Health in Islamabad.
The Pakistan Regional Polio Lab will go a long way in facilitating poliovirus detection in stool samples and the environment. At present, the lab tests more than 30,000 stool samples from people with paralysis and 950 environmental samples each year, including samples from both Afghanistan and Pakistan. The new soon-to-be operational lab equipment will speed up the ability to process and respond quickly wherever the poliovirus may be hiding. This is critical work in ensuring Pakistan targets its last remaining core reservoirs of poliovirus.
In this last mile of polio eradication, support from JICA is crucial and much appreciated. Pakistan is one of the last remaining polio endemic countries in world, along with Afghanistan and Nigeria. The political and financial commitment from the Government of Japan over the years has already helped Pakistan in reducing the number of polio cases by 96% since 2014. With only 12 cases reported in 2018, Pakistan has a fighting chance of finally consigning polio to the history books.
The Japan International Cooperation Agency (JICA) assists and supports developing countries as the executing agency of Japanese ODA. In accordance with its vision of “Inclusive and Dynamic Development,” JICA supports the resolution of issues of developing countries by using the most suitable tools of various assistance methods, such as technical cooperation, ODA loans and grant aid in an integrated manner.
In close collaboration with the Bill & Melinda Gates Foundation, WHO’s Regional Office for Africa is continuing to roll-out an innovative disease surveillance platform, enabling the real-time detection of suspected polio cases anywhere on the continent.
Thousands of health workers, volunteers and members of local communities across the continent have been equipped with geo-coded mobile phone technology, and trained to conduct regular and active surveillance visits to health centres across Africa. Professionals and volunteers are tasked to regularly visit local health clinics and actively check for the presence of any child with polio-like symptoms (known as acute flaccid paralysis – AFP), or to look for children in their communities presenting such symptoms. This information is subsequently fed back in real-time to national and regional authorities, enabling for rapid action and immediate dispatch of an investigative team as needed.
“This really is the future of disease surveillance,” comments Reuben Opara Ngofa of WHO’s African Regional Office in Brazzaville, who was instrumental in developing this innovative system and who recently returned from Burkina Faso where he helped roll out the system in remote areas. “Particularly in remote or hard-to-reach areas, we need to know immediately if we have polio circulating in the area, and this system allows for real-time information, which in turn allows for an immediate real-time response. If one of our informants identifies a child with polio-like symptoms anywhere, we will know about it immediately. We are really giving the poliovirus nowhere to run.”
In addition to polio, this system helps detect and respond to other vaccine-preventable diseases, such as measles, yellow fever and neonatal tetanus. Across west Africa, measles vaccination coverage is being assessed through this system, and a cholera outbreak in 2018 in Ethiopia was actively tracked. It is a clear example of the polio infrastructure adding value over and beyond merely eradicating polio.
Thanks to such innovations, and efforts of dedicated professionals and volunteers across Africa, the continent stands on the brink of a historic public health success: the certification of wild poliovirus eradication. In 1996, when Nelson Mandela launched the Kick Polio Out of Africa campaign, wild poliovirus paralysed more than 75,000 children every year, across every African country.
No wild poliovirus has now been detected since 2016, and this real-time GIS surveillance system will provide crucial additional surveillance data, to truly validate the absence of wild poliovirus. Data generated through this system will be critically evaluated by the independent African Regional Certification Committee on polio eradication, when evaluating whether the Region as a whole can be certified as free of wild poliovirus in early 2020.