In an extraordinary joint statement by the Chairs of the main independent, advisory and oversight committees of the GPEI, the Chairs urge everyone involved in polio eradication to ensure polio will finally be assigned to the history books by 2023. The authors are the chairs of the Strategic Advisory Group of Experts on immunization (SAGE), the Independent Monitoring Board, the Emergency Committee of the International Health Regulations (IHR) Regarding International Spread of Poliovirus and the Global Commission for the Certification of the Eradication of Poliomyelitis (GCC).
The Endgame Plan through 2018 has brought the world to the brink of being polio-free. A new Strategic Plan 2019-2023 aims to build on the lessons learned since 2013.
The joint statement urges everyone involved in the effort to find ways to excel in their roles. If this happens, the statement continues, success will follow. But otherwise, come 2023, the world will find itself exactly where it is today: tantalizingly close. But in an eradication effort, tantalizingly close is not good enough.
The statement therefore issues an impassioned plea to everyone to dedicate themselves to one clear objective: to reach that very last child with polio vaccine. By excelling in our roles. It means stepping up the level of performance even further. It means using the proven tools of eradication and building blocks that have been established in parts of the world that have been free of polio for years.
The Chairs remind us that as a global community, we have stood where we stand today once before, with smallpox. And we achieved the eradication of smallpox. And the world is a much better place without smallpox.
So, let us make the world again a better place. Together. Let us eradicate polio.
Since polio was confirmed in Somalia in late 2017, health authorities have led a complex response to twin outbreaks of circulating vaccine-derived poliovirus type 2 and type 3 (cVDPV2 and cVDPV3), paying special attention to high-risk populations: nomads, internally displaced people (IDPs), and people living in peri-urban slums and rural areas.
So far, five of Somalia’s 12 infected children are from nomadic communities, and another four are from internally displaced families living in urban areas. To boost immunization among eligible children in these populations, vaccination activities have placed a special focus on reaching these communities.
Somalia has a rich culture of people leading pastoral lifestyles, raising livestock and moving with them as the seasons and the weather change. Nomadism has a long history in Somalia and nomads have a special place in Somali society: almost a third of Somalia’s people are nomads. However, they do not observe formal international borders – just like the poliovirus. For health workers, this context poses a significant challenge: How can you be sure you have vaccinated every last child when so many children are on the move?
For health workers, this means searching for polio symptoms in more than 900 health facilities across the country, as well as nutritional centres, camps for IDPs, and key sites along Somalia’s borders. At transit points, along borders and at water collection points, polio teams work to vaccinate children moving in and out of areas experiencing conflict or with limited access to health services. In high-risk areas, the Somali Government, WHO and UNICEF hire local vaccinators – people known and trusted by their communities – and when additional security is necessary, polio partners provide it.
Gaining high-level political goodwill
Even in an emergency, cross-border collaboration is not always easy to come by. In the Horn of Africa outbreak, regional collaboration moved into high gear in September, when health ministers from across the region and representatives from the Intergovernmental Authority on Development (IGAD) countries came together in the Kenyan town of Garissa to reiterate their commitment to ending polio.
One of the event’s key messages was around the risks posed by the easy and frequent mobility of communities across borders. Kenya’s national polio immunization ambassador, former UN Person of the Year and polio survivor, Harold Kipchumba, spoke directly to the pastoral communities in the region.
Kipchumba highlighted their focus on vaccinating animals, and urged parents in these communities to use the same vigour to vaccinate their children against polio, so they are able to serve as future herders for their families.
A regional response to support high-risk populations
The Technical Advisory Group, an independent body of experts that monitors outbreaks and offers guidance, recommended that countries in the region strengthen their coordination. In response, the Horn of Africa Coordination Unit coordinates joint responses among HoA countries – work that includes monitoring current outbreaks, and collaboratively planning, mapping, conducting immunization campaigns and communicating with various audiences. This ensures that countries work together in partnership rather than in silos, viewing the outbreak as one epidemiological block.
At regional and district levels, teams have spent the last few months building records of every settlement in their area, by lifestyle (nomad, IDP, peri-urban slums, rural). The highest priority: locating special populations – internally displaced persons, refugees, nomadic families, people living in informal settlements in urban areas and communities living in access-compromised areas – in order to reach them with vital polio vaccine.
A vital step in reaching more children, particularly those on the move, has been to move away from paper records and use electronic tools to collect data on children reached and missed during campaigns. This gives data specialists and decision-makers timely, accurate information, allowing them to analyze data in real time and flag areas with where high numbers of children are missed, so teams can revisit these households the following day.
Getting vaccines to the doorstep is not the only challenge for polio eradication teams in Somalia. Parents and caregivers also need information to ensure their children are vaccinated – something Kipchumba spoke to. On rare occasions, vaccinators meet families unconvinced of the need for vaccinations, particularly when the family has a newborn child or a sick child. In the lead up to every campaign, teams of social mobilizers, sometimes joined by influential Islamic leaders or scholars, visit communities to alert them of dates of polio immunization campaigns and the benefits of vaccination. Here, too, special attention is paid to nomadic communities, as polio teams liaise with elders from these communities in order to learn more about these communities and their needs, and to inform community members in appropriate ways about immunization dates and benefits of vaccination.
In the last week of October, Djibouti’s Ministry of Health, working with WHO, UNICEF and other partners, successfully carried out the country’s first polio National Immunization Days (NIDs) since 2015.
While Djibouti has not had a case of polio since 1999, the recent outbreaks of polio in neighbouring countries in the Horn of Africa, and the low levels of routine immunization coverage in some areas in the country, are indications that Djibouti is still at risk if poliovirus spreads through population movements. Other countries in the Horn of Africa are already cooperating to stop the ongoing outbreak and to reduce the risk of spread, and especially considering that Djibouti is on a major migration route in the Horn of Africa, it makes a lot of sense for Djibouti to join in this coordinated response.
For Dr Ahmed Zouiten, the acting WHO Representative (WR) in Djibouti, this context demanded action.
“I prefer to deal with a campaign for prevention than to have to deal with an outbreak of polio,” he said.
With that in mind, an NID planned for 2019 was brought forward and carried out over 23-26 October. The target was 120 000 children under five years of age, a number suggested by Djibouti’s last census, in 2009. Two strategies were proposed: one approach, where children would be vaccinated at fixed points (health facilities) and a complementary door-to-door approach using two-person teams (a vaccinator and a registration person).
In the days and weeks before the NID, all partners, including the government, WHO and UNICEF, used a variety of communication channels – from outdoor signage to radio spots – to ensure that communities were informed not just of the risks of polio, but also of the importance of protecting children from vaccine preventable diseases.
The campaign’s official launch ceremony was held at the Youssouf Abdillahi Iftini Polyclinic in Balbala neighborhood, Djibouti City, in the presence of Djibouti’s Minister of Health, WHO and UNICEF representatives, and other partners. Over the course of the following days, vaccinators surpassed targets, vaccinating all children under five they encountered living on Djibouti territory, regardless of their origin, including nomadic populations, refugees and migrant children.
Although final numbers are still being tabulated through independent monitoring mechanisms, initial results suggest high coverage of the target population. This means vaccinators reached the estimated target number of children, and more, such as newer cohorts of children not accounted for in earlier estimates. Catching these children helps to further inform immunization estimates for any further campaigns.
For Dr Zouiten, a result like this is something to celebrate.
“Today, our children are on their way to being better protected, and we are launching a second campaign in the near future to follow up on that,” he said.
“Before, we had some worries; we thought that the circulation of poliovirus in the region posed a risk. Now with this first vaccination campaign, we know we are on the right path to ensure the children of Djibouti are protected. These results weren’t easy to achieve, but were made possible through collaboration between the Ministry of Health, the partnership between WHO, UNICEF and others.”
Given the high risk of importation of poliovirus, the Government of Djibouti, WHO and UNICEF are not taking any chances: plans are in the works for a second and third NID to roll out in 2019. With an outbreak in the region, it is critical for nearby countries to strengthen their own immunity levels and ensure routine immunization and disease surveillance systems are strong enough to detect any virus circulation. Despite the cost and effort of staging national immunization activities, in this case, all partners agree: an ounce of prevention really is worth a pound of outbreak response.
In June 2017, some of the first circulating vaccine-derived poliovirus type 2 (VDPV2) cases were reported in Deir Ez-Zor governorate, in eastern Syria, confirming an outbreak of polio. Since then, 74 cases were reported, with the most recent case reported on 21 September 2017.
Despite being a high-risk country with large scale population movements, inadequate health infrastructure, and accessibility issues, the outbreak response was successfully carried out. Health workers reached out to children to raise immunity levels, vaccinate children, and stop the outbreak, regardless of the location or socio-political climate.
An official outbreak response assessment was carried out by experts on global health, virology, and epidemiology, which concluded that the outbreak could now be closed.
“(Disease) Surveillance is stronger today than it was 18 months ago, when the initial cases were detected…so, as we celebrate what is a remarkable achievement in stopping this outbreak, amid very challenging circumstances, we must not lose sight of the risks posed by continued circulation of virus in other parts of our Region,” said Chris Maher, Manager for Polio Eradication in the WHO Eastern Mediterranean Region.
A nation-wide immunization campaign helped in eradicating polio in India. WHO/2011
Eradicating polio in India was a feat of dedication, commitment and simply doubling down on immunization activities. Given India’s vast population, tropical climate in many parts of the country, and other environmental challenges, it would be easy to imagine that if polio couldn’t be stopped, India would be the place to fail.
Simply put: it was a challenge. After all, India constituted over 60% of all global polio cases as recently as 2009.
However, in 2014, India was officially declared polio-free, along with the rest of the South-East Asia Region. Thanks to the singular commitment of the Indian Government at all levels, partners of the Global Polio Eradication Initiative, notably WHO, Rotary International and UNICEF, polio was tackled head-on. India has not had a case single case of wild polio virus since 2011.
India had long been considered one of the most difficult geographical locations to eliminate the disease. Success in India really changed the game, and now serves as an example that eradication of polio is indeed possible when the world marshals political will and commits adequate resources to the cause that affects everybody worldwide.
Today, the world is close to making public health history when it comes to polio – as it was when in 1980 small pox was officially eradicated. The goal of reaching a polio-free world is well within reach.
Tune in to listen to the podcast as the UN Dispatch tells the story of how, against all odds, India wiped out polio, and some of the lessons learned along the way.
Chief Imman of Dutsen wai Sheck Zakaria Mohammed Sani sending message on RI and ANC during Eld-Kabir Prayer. UNICEF Nigeria
Malam Musa Abubakar was an ardent opponent of polio vaccination and other health services, not allowing his children to be immunized or his wives to receive antenatal care or other health services.
“I used to chase off immunization officers whenever they came to my door because I believed there was a hidden agenda behind it, and I was also uncomfortable allowing my wives to go to the hospital,” admitted Abubakar who hails from Zaria in Nigeria’s north-central Kaduna State.
Abubakar’s views changed, however, once Muslim clerics began to explain to the community the importance of allowing women and children to access health services and immunizations, along with the dire consequences of rejecting immunization services.
Delivering life-saving messages
Malam Ibrahim _Kaduan south RFP vaccinating a Child of NC house holdm at T-wada, Kaduna South LGA. UNICEF Nigeria
Religious, socio-cultural, and safety concerns are among the main barriers to polio vaccination and other health services in most of northern Nigeria.
United Nations Children’s Fund (UNICEF) has engaged 228 religious leaders in 11 northern Nigerian states, particularly in Muslim communities, to mobilize caregivers against social norms that prevent families from vaccinating their children. Muslim and Christian clerics deliver life-saving messages during sermons and other religious gatherings to dispel negative attitudes toward vaccinations and other health services.
Collaboration with religious leaders has not only supported polio eradication efforts but has also brought about further benefits in the fight against infant and maternal mortality through awareness campaigns.
“We have a duty to ensure people can live healthy lives”
Speaking at an annual meeting of 228 religious leaders held in Abuja in September 2018, Dr. Anis Siddique, UNICEF Chief of Communication for Development, described female and male religious leaders as game changers and encouraged them to create demand for immunization.
Sheik Abubakar Gumi, a renowned Muslim thought-leader and cleric, said that cooperation with religious leaders is creating positive change.
“Up until a few years ago, people in Muslim-majority communities stayed away from health centres, rejected polio vaccines and other routine immunizations even if they were brought to their doorstep due to misconceptions, suspicions, and socio-cultural norms,” explains Sheik Gumi. “But this changed with the engagement of religious leaders, who have succeeded in mobilizing people against behaviours that have put the lives of women and children at risk.”
Seeing respected religious scholars endorse immunization, others have also followed suit. Haruna, who leads Friday prayers at a mosque in Kaduna, speaks to over 1000 men every week about the importance of women and children accessing health services.
These collective efforts have brought about shifts in attitudes and knowledge as an average of 20 000 men who attend weekly Friday prayers across the mosques in northern Nigeria receive resounding messages on polio immunization and antenatal care-related health services.
“I used to be non-compliant but was convinced by Sheik Gumi about the dangers of rejecting immunization and other health services that are specifically provided to prevent women and children from dying of preventable diseases. As religious leaders we have a duty to ensure that all people can live healthy lives,” says Haruna.
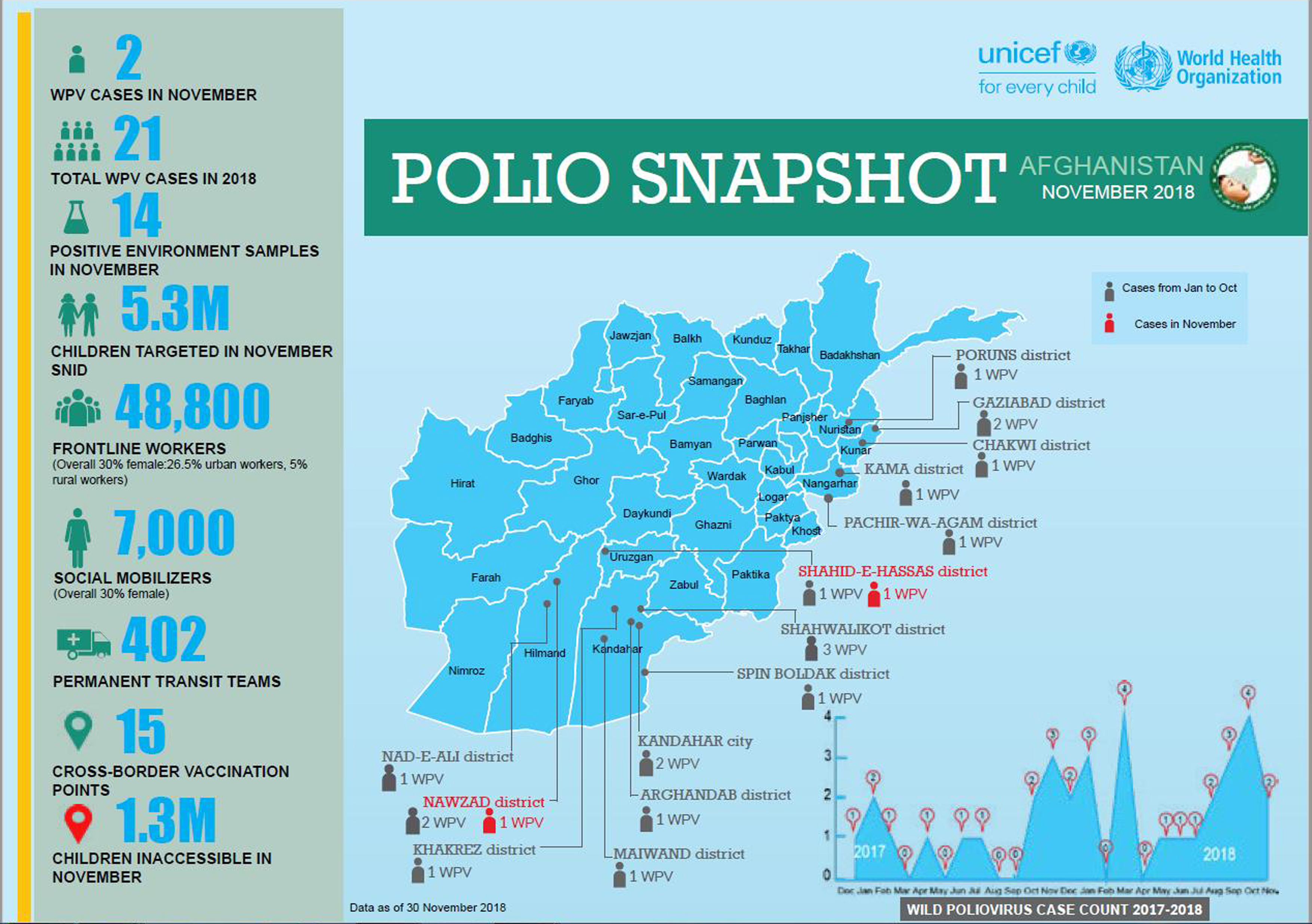
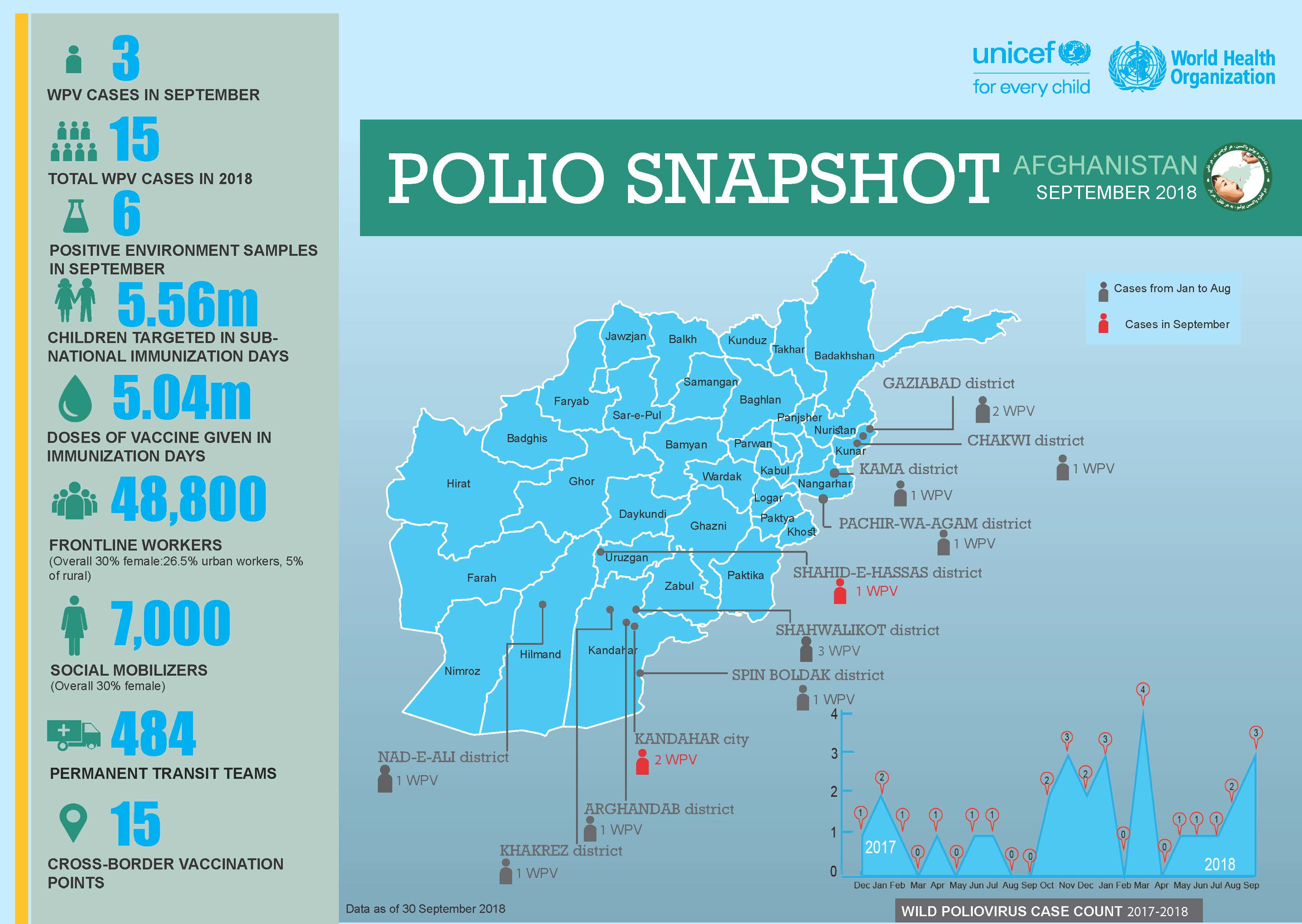
In September
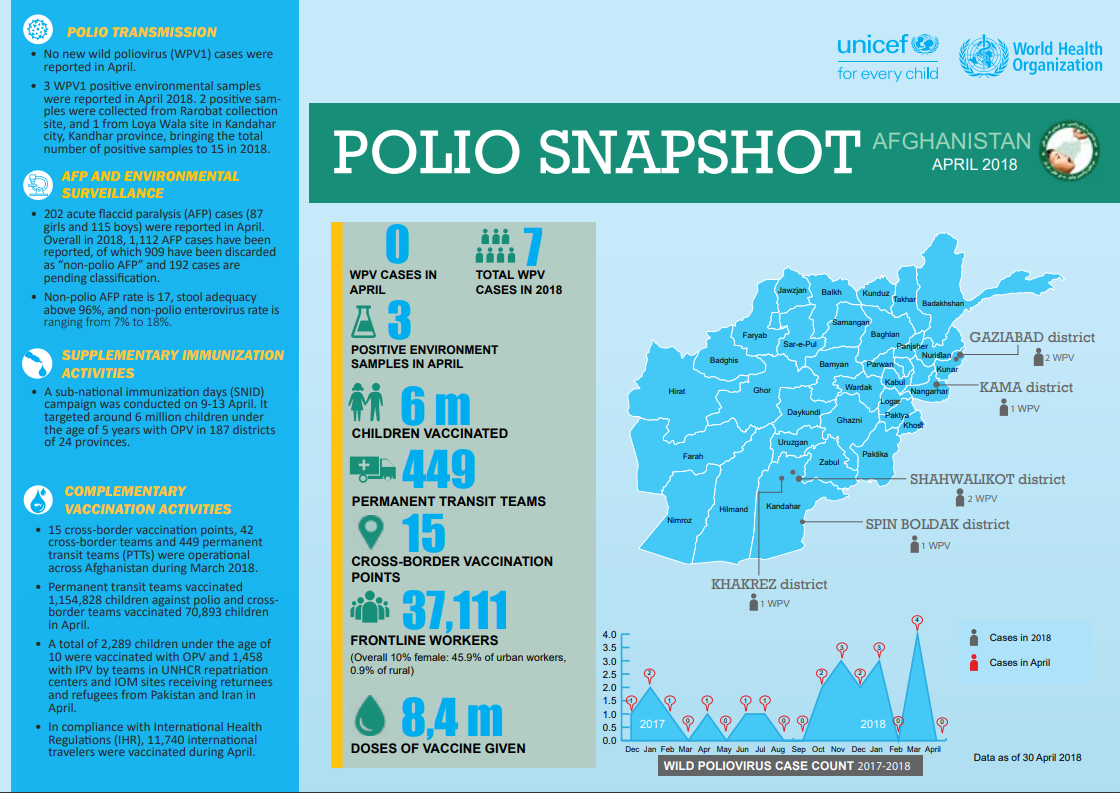
3 new wild poliovirus (WPV1) cases were reported in September 2018.
In the September Sub-National Immunization Days, 5.6 million children under the age of five were targeted.
484 permanent transit points (PTPs) were operational across Afghanistan during September 2018.
Pakistan polio eradication programme has achieved significant progress in recent years, thanks to renewed government commitment and revitalized community ownership. However, in cities like Karachi, poliovirus continues to be detected.
Working to overcome the virus once and for all, the polio programme an emergency action plan in January 2018. Since then, the geographical scope of the virus has been noticeably reduced. Much of this progress is thanks to religious leaders like Imam Qari Mehboob, who has spent years building trust and demand for polio vaccination in some of the most difficult areas of the city.
Gulshan-e-Buner is in the eastern corner of Karachi. The town includes some of the most impoverished and high-risk populations of the city. Playing in the streets, playgrounds and compounds that wind up and down the hilly landscape are around 2200 boys and girls under five years old. The places where they learn to crawl, walk, and run are perfect hiding spots for the paralysing poliovirus, but the last detection in the environment was in June 2016. No child in Gulshan-e-Buner has been paralysed by polio since 2014. In a community where vaccine refusal has sometimes caused problems, this represents a dramatic transformation.
Gulshan-e-Buner is one of the high-risk areas of Karachi where the polio programme first began community-based vaccination. Religious leaders helped to identify and recruit female vaccinators to reach every child with vaccines, and the area seemed well on the way to becoming polio-free. Then in 2012, an attack on health workers caused vaccination activities here to stop. In the years since, the commitment of religious leaders to ensure security, restore access, and build community trust has been crucial to defeat the virus.
Iman Qari Mehboob is 50 years old, a migrant from Khyber Pakhtunkhwa like most of his neighbours. He calls the community to prayer five times a day, and teaches many of the youngest children in the town. A father of four children, he is devoted to keeping them and all the other children in his community safe from the poliovirus. His support of the polio programme has helped increase vaccine trust, boost uptake of routine immunization services, and spark conversations about the vaccine.
During every polio vaccination campaign, Qari Mehboob goes from house to house with vaccination teams to check for any unvaccinated children. He speaks to parents who refuse the vaccine for their child, reassuring them that it is safe and effective. He conducts his work under the guidance of the National Islamic Advisory Group for Polio Eradication (NIAG), which educates religious leaders about polio eradication and the unique and important role they can play in protecting all Pakistan’s children from polio.
Under the guidance of NIAG, religious leaders are trained on the basics of social mobilization, communication, health, and hygiene. They also learn about the religious justifications for polio vaccination, including examining the arguments and fatwas of influential religious scholars.
Reflecting on his training, Qari Mehboob says, “The toughest job [for the NIAG trainers] is to convince religious clerics because their denial and doubt is deep rooted, but the collective Fatwa [scholarly verdict] of prominent scholars helps a lot”.
Since his training, Qari Mehboob has organised community engagement sessions to raise awareness about the dangers of the poliovirus. He often makes vaccination a central theme during his sermons at Friday and Eid prayers.
“I face less resistance because most of the people here know me personally and they rely on me because of my status as a religious cleric.” he says.
Qari Mehboob also uses the power and platform of his mosque to amplify his voice. He means this literally – sometimes he can be found using a loudspeaker. That’s so that mothers working inside compounds and homes can hear his messages, as well as the fathers who attend prayers. He doesn’t just speak about polio eradication, but also educates his community about personal hygiene, routine immunization and importance of education in Islam.
To thank him for his work, the provincial polio eradication programme team gave Qari Mehboob a clock during a Mosque promotional activity a few years ago. Below the time lies a message emphasising the importance of vaccination. Now displayed prominently on the wall of the mosque, the gift reminds parents why the polio vaccine is one of the best gifts that they can give to their children.
Back out in the streets of his town, Qari Mehboob laughs with local children as he checks their finger marking to make sure that they are vaccinated.
Discussing his motivation, he says, “These children are my own children. So I must protect them from any harmful disease - especially from a crippling disease like polio.”
At the end of the day’s campaign, Qari Mehboob offers tea and cookies to members of the provincial polio eradication programme team.
Since he joined the programme, vaccine refusals in Gulshan-e-Buner have dropped by 50%, and far more children receive their full polio vaccine doses on time.
Reflecting on the impact of his work, Qari Mehboob returns to his desire to keep all children safe. “I feel an extreme level of contentment after I contribute my part in the programme,” he says.
In the Democratic Republic of the Congo, emergency response has been ongoing since 2017 to overcome outbreaks of circulating vaccine-derived poliovirus, caused by low rates of routine immunization. In the battle to close the outbreak, health workers, partners of the Global Polio Eradication Initiative, Governors of affected provinces, and the Ministry of Health are working together to vaccinate every child. In a context with weak health systems and other high-profile health and humanitarian emergencies, these united efforts are crucial to boost population health and keep all young children safe from paralysis.
In Tanganyika province, where poliovirus was first detected in September 2017, outbreak response is focused on reaching all vulnerable populations with the safe, effective oral polio vaccine. Health infrastructure is weak in the province, and it has taken concerted efforts to reach many children. Here, mothers with their babies queue for polio immunization activities in Manono district, organized with the support of WHO, UNICEF and partners.
Despite several campaigns, immunity gaps still remain. Continuing cases from several virus strains in the country show that the battle to protect every child from paralysis is far from over. Here, a nurse carefully places vaccines vials back in a cooler during immunization activities in Manono. It is critical that the polio vaccine is kept cool, a considerable challenge in warm locations far from the nearest vaccine storage facility.
A small boy is vaccinated against polio after waiting in line with his mother. The Democratic Republic of the Congo has some of the lowest vaccination rates worldwide, and it is hoped that the lessons learned in overcoming this and other health emergencies will help strengthen the country’s health system for the future, and prevent other outbreaks.
A community mobilizer tells a woman in a village in Manono about the polio vaccination campaign that has just begun. Community mobilizers, usually local people trained by UNICEF and partners, are a critical part of efforts to ensure that every child is protected from the virus. Going house to house, they speak to parents about the dangerous poliovirus, and answer questions about the vaccine. Often, they also provide other health service support, including child and maternal health advice.
A girl has her little finger marked after being vaccinated against polio. All children under the age of five are being targeted in vaccination campaigns in the affected districts.
Amongst the communities here, there are children whom the virus has already reached. Remy Muyombi was previously an opponent of vaccination. Since his three-year-old son Justin was affected by polio paralysis, he has become a strong advocate of the campaigns ongoing in his district. So far in 2018, there have been eleven confirmed cases of polio paralysis due to the outbreak. In 2017, 22 children were paralyzed.
A community health worker crosses a shallow stream with his bike to reach the most distant children in Manono health zone. Many communities here live hours from the nearest road, far from any route that a car could easily traverse.
After a household is visited with vaccines, health workers mark the home with chalk to show that the children there have been immunized. They also collect paper records of vaccination, to feed back into a central monitoring and evaluation system coordinated by WHO.
Community mobilizers speak to a mother in Kalunga site for internally displaced people in Tanganyika Province. Regular movement of people in the Democratic Republic of the Congo complicates outbreak response, as there is a real threat of virus spread. The programme works specifically with moving and displaced populations to boost immunization rates, and collaborates with other UN agencies to gather up-to-date information on population movements and the wider humanitarian situation in the country.
A girl is vaccinated against polio in Manono. With each campaign, the polio eradication programme is looking to protect more children, and get closer to ending the outbreak. More polio immunization activities are planned for the coming months, building on commitment from the government of the Democratic Republic of the Congo and provincial governors. Working with other programmes, and in complex contexts, the polio eradication teams continue their work to keep every child safe from polio paralysis.
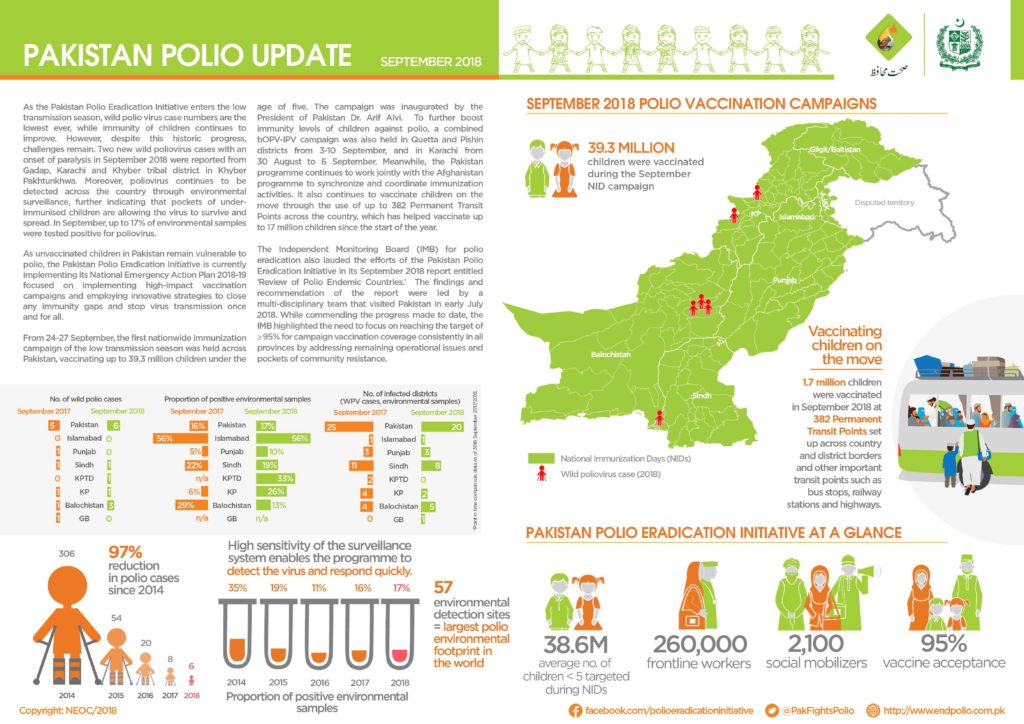
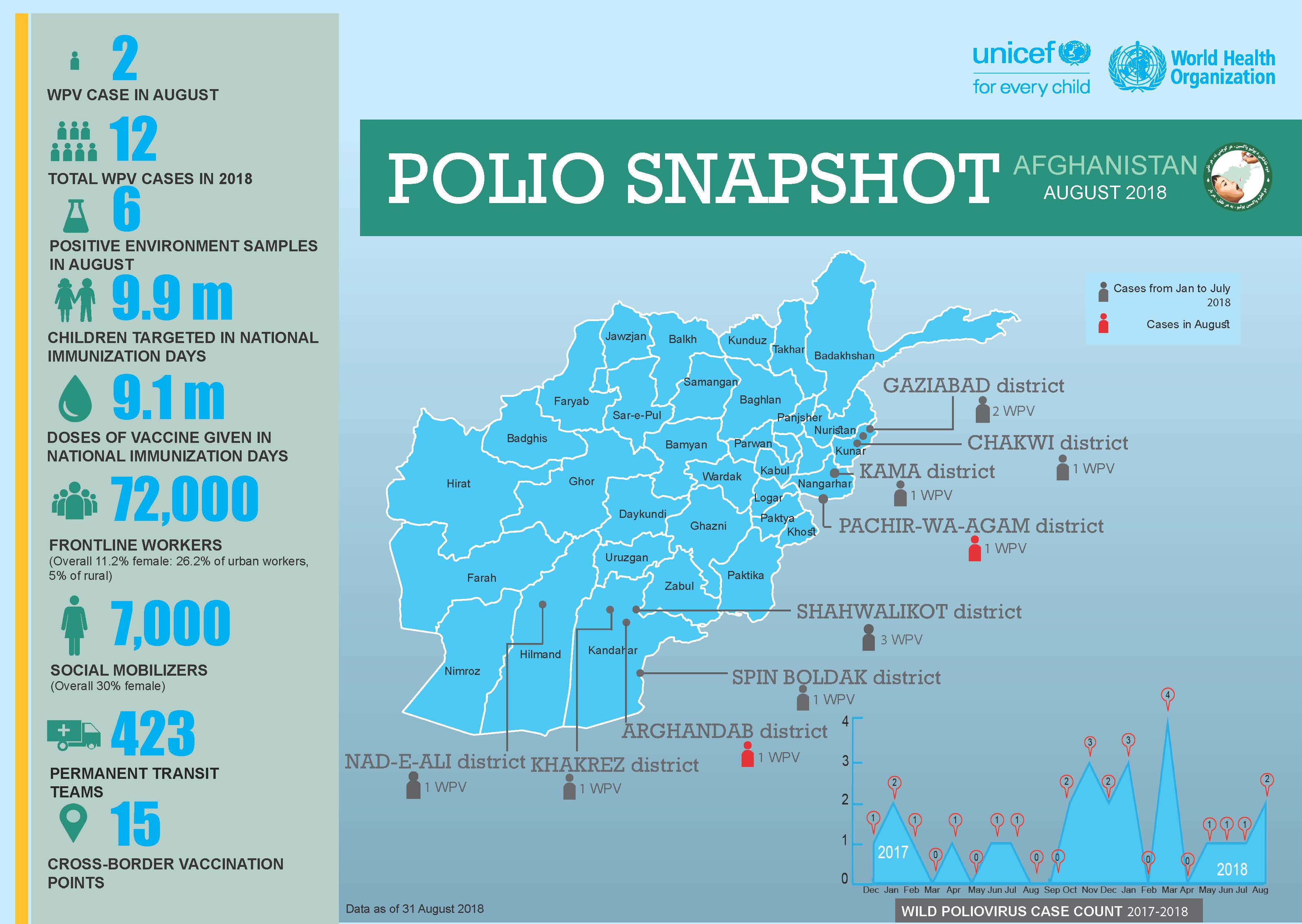
In August
-Intensified eradication efforts are continuing in Afghanistan, in close cross-border coordination with Pakistan.
-Efforts are focusing on reaching children in hard-to-reach areas, and among mobile population groups.
-Subnational surveillance sensitivity continues to be strengthened.
“Please wait, I’ll soon be with you,” says Nasiru, the father of six children, as he disappears into his house in Gagi Makurdi settlement in Nigeria’s northwestern State of Sokoto.
Within minutes, Nasiru reappears, proudly displaying immunization cards with the record of the vaccines given to his youngest three children. It is unusual for fathers in this conservative part of Nigeria to readily know the whereabouts of these documents. Tending to children and ensuring that they stay healthy is usually a mother’s job.
“Take a look at the cards. My children Fidausi and Fatima have completed all their required immunization, whilst my youngest, Nana Asmaiu, is well on course to complete his,” he says.
Nasiru is a champion for immunization, but he wasn’t always so enthusiastic.
20 000 community mobilizers
It was Hauwa Ibrahim, a 46-year-old UNICEF-trained Volunteer Community Mobilizer, who persuaded Nasiru that the vaccine was safe and effective. She is part of a 20 000-strong network of community mobilizers who work across twelve Nigerian states like Sokoto, where some communities have been resistant to polio vaccination.
As recently as 2012, Nigeria used to account for half the world’s polio cases. Today, with help from women like Hauwa, no wild poliovirus has been detected in the country since August 2016. There are still many immunity gaps in Nigeria – as underlined by an outbreak of vaccine-derived virus currently ongoing in the country – but in the villages where VCMs like her work, these gaps are beginning to close.
Using a simple register, Hauwa goes house to house in Gagi Makurdi to record all children below the age of five, as well as women who are pregnant. It is the same register that Hauwa used to track the pregnancies of Nasiru’s wife – Zara’u – and she now uses it to find out who manages the routine immunization schedules of the three youngest children in the household.
Strengthening routine immunization
This forms part of the polio programme’s work in Nigeria to strengthening routine immunization, building on the infrastructure developed to eradicate the virus.
Upon her first visit, Hauwa was determined to convince Nasiru that vaccination against polio and other diseases is important – and that he should take the children to the health facility.
“My culture does not allow a wife to go outside of the compound, so when Hauwa insisted that we take our children to the health facility for vaccines, I had no way but to go myself. Else, Hauwa would not give up,” Nasiru explains. Whilst he travels with his children, Zara’u takes care of their older siblings at home.
By recruiting locally influential women like Hauwa from communities where some parents are vaccine-hesitant, and training them to be advocates for child health, vaccination rates are improved throughout their neighbourhoods. In some areas, more than 99% of parents now accept the polio vaccine for their child.
“Hauwa resides in this settlement and I trust her; I trust that the advice she is giving is in the best interest of my children,” says Nasiru.
He also notes, however, that he is often the only man at the health facility.
Engaging all fathers
Hauwa hopes that by encouraging more fathers to take on the parental responsibility of completing their children’s routine immunization schedule, immunization coverage will increase across Sokoto. Greater vaccine acceptance and awareness means that children are more likely to receive a life-saving polio vaccine, and other vaccines, whether through routine immunization or through door-to-door vaccination.
Already, the trust that she has built amongst parents in Gagi Makurdi has helped surmount many of the barriers that deny children immunization and other health services. In Nasiru and Zara’u’s compound, nearly all children are now protected against polio and other vaccine-preventable diseases.
Only their baby, Nana Asmaiu, has yet to have all his vaccinations – and Hauwa will soon visit his household to support Nasiru and Zara’u, and ensure he gets them.
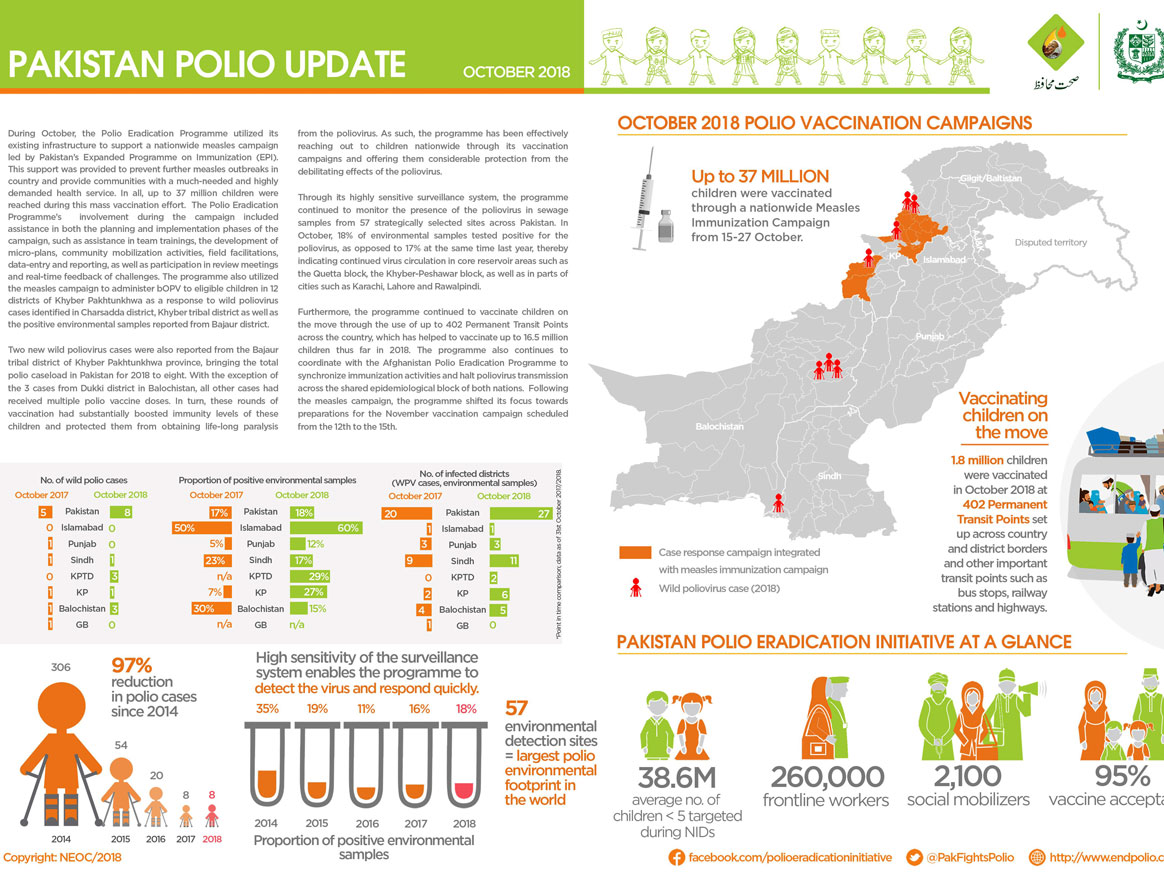
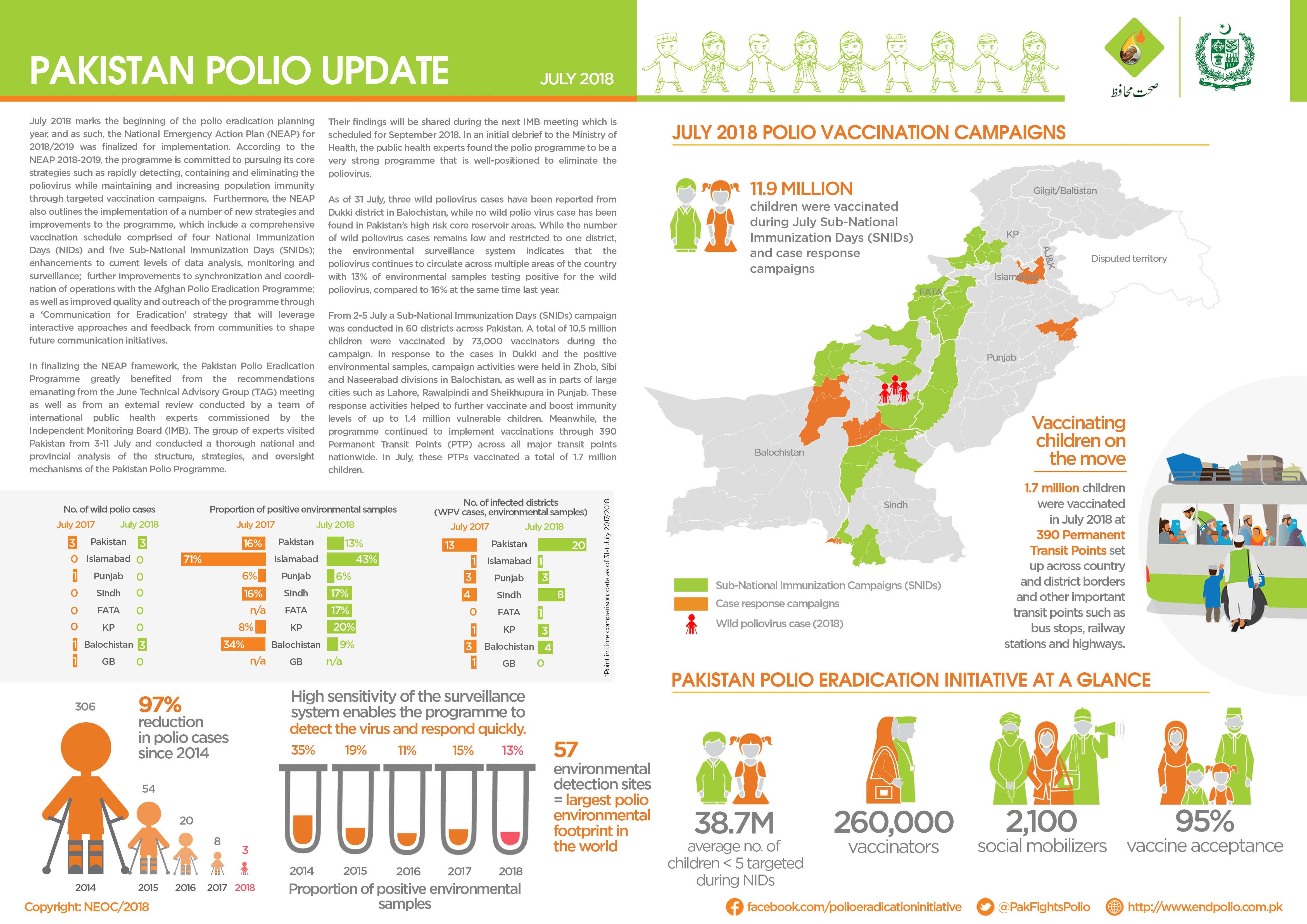
In July:
There were no new cases of wild poliovirus (WPV1) reported.
10.5 million children were vaccinated against poliovirus during case response campaigns by more than 73 000 dedicated frontline workers.
Teams at transit points and borders successfully vaccinated 1.7 million children.
This is southern Afghanistan. A place characterized by a rich, diverse, but often complex history. Enveloped by mountains, this part of the country has seen years of conflict which have left hospitals under-resourced and health services shattered. Children face many challenges – as well as conflict and poverty, southern Afghanistan has the highest number of polio cases in the world.
In this difficult environment, the virus can only be defeated if every child is vaccinated.
Afia (not her real name), who is nineteen years old, is one of over 70 000 committed polio workers in Afghanistan, supported by WHO and UNICEF. Last month, she and her colleagues vaccinated 9.9 million children and educated thousands of parents about vaccination across the country.
The polio eradication programme comprises one of the biggest female workforces in Afghanistan: a national team, all fighting polio. Some women work as vaccinators, whilst others, like Afia, are mostly engaged in education and social mobilisation efforts. The polio programme gives women culturally-appropriate opportunities to work outside the house and engage in their community, speaking to parents about the safe, effective polio vaccine, and answering their questions. Often, women vaccinators offer other kinds of health advice, including recommendations for good child and maternal health.
To be a good vaccinator and educator, women must be committed to better health for all, with strong communication skills. They must also be organized to ensure that every child is reached during the campaign.
Afia says that if she wasn’t eradicating polio, her parents would expect her to give up her education and get married. Her younger sisters look up to her, excited to work in the polio eradication programme when they are old enough.
Her job is very important to protect all children. Afghanistan is just one of three countries – the others are Nigeria and Pakistan - that have never interrupted poliovirus transmission.
Women can vaccinate children who might otherwise miss out. Culturally, male vaccinators are unable to enter households to administer vaccine, causing difficulties if young children are asleep or playing inside. Their freedom to enter homes and give the vaccine to every child is one reason female polio workers are so critical.
Afia started work at 7 am, and is now walking home ten hours later with a young boy she has just vaccinated. Her purple burka stands out against the sand as she goes home to tell her parents and siblings about her day.
Afia feels positive about the future of polio eradication in Afghanistan: “We have a duty to protect our children, and I won’t stop working until every child is protected.”
Women have a right to participate in all aspects of polio eradication. Removing barriers to women’s full participation at all levels is a key goal for the Global Polio Eradication Initiative (GPEI). To learn more, see the gender section of our website, and read the GPEI ‘Why Women’ Infographic.
Almost everyone in the Killa Saifullah district of Balochistan, Pakistan, knows and respects 35-year-old Taj Muhammad. A dedicated and passionate doctor by profession, Dr Taj spends his days working as a Union Council Medical Officer in his local public health facility, and his evenings running a free medical clinic for local residents.
In his capacity as Medical Officer, he coordinates polio eradication efforts at the Union Council level, which is the smallest administrative unit in Pakistan.
His role includes coordinating microplanning, training frontline health workers, and supervising polio vaccination campaign activities. Since the start of his medical career in 2007, he has supervised more than 100 polio vaccination campaigns.
Dr Taj says he became a doctor to fill the existing health care gap in his area. “During my childhood, my mother was seriously ill and she died because of the absence of medical facilities in our area. She often used to tell me that I must become a doctor to help poor people with their health. She died afterwards but her words are still in my heart,” he explains.
His hometown, Killa Saifullah, is located 135 kilometers away from Balochistan’s provincial capital Quetta. Economic and social deprivation is widespread, and the district lacks basic health facilities, particularly for women and children. “There is only one hospital, serving only 150 people per day in the district, whereas the current population is more than 200,000. In these conditions, working as a medical officer is quite challenging,” Dr Taj says.
His job is tiring, and the demands are huge, but Dr Taj perseveres. As well as supporting polio vaccination activities, and endorsing vaccination, each day he tends to the large crowd of people who gather outside his evening clinic, often desperately needing health care.
His work to serve his community is particularly important because Killa Saifullah lies close to Dukki, where the only case of polio in Pakistan so far in 2018 was reported. Nawabzada Dara Khan, who chairs the Killa Saifullah’s Municipal Committee, notes that the community feels “vulnerable” knowing that the virus is close by.
Since the first polio case of 2018 was detected, polio vaccination campaigns have been conducted in response in all neighboring districts, including Killa Saifullah. But whilst this has increased immunity to the virus, it has also caused vaccine hesitancy amongst some parents, who question the need for multiple vaccination campaigns.
“We are trying hard to vaccinate each and every child; however, repeated campaigns and misconceptions are posing a big challenge for us,” Dara Khan says.
Luckily, the efforts of dedicated doctors like Dr Taj are helping to remove misconceptions and doubt. With the immense trust and respect he enjoys from his community, he has been able to use his free evening clinic as a local platform to advocate for polio eradication and the safety of the vaccine, extending his critical role in the polio programme.
Dara Khan adds, “The contribution of Dr Taj in polio eradication is commendable. His goodwill is playing a very positive role within our community to remove these misconceptions.”
His impact is also wide ranging, reaching multiple different families.
The proof? In April, thanks to the intensive efforts of Dr Taj and others, no parents or caregivers in Killa Saifullah refused vaccination.
That’s 70,690 children who now have lifelong protection from polio.
How do vaccinators ensure that every child is reached?
Every child needs to be vaccinated to protect them from poliovirus. To achieve this, detailed plans are prepared for vaccination teams. The aim is to find each child under 5 years of age – in Afghanistan, that’s around 10 million – and to reach them with vaccines.
A heavy steel gate opens on a quiet suburban street in central Herat. The city lies in a fertile river valley in Afghanistan’s west, an area rich with history. Over the centuries, invaders from Genghis Khan’s army to the troops of the Timurid empire, the Mughals and the Safavids have opened the gates to rule the city once known as the Pearl of Khorasan.
Now, a far more peaceful group can be seen walking down the streets of Herat. Equipped with blue vaccine carrier boxes and drops of polio vaccine, the teams knock on one door after another to vaccinate any children they find inside. The aim is to eradicate polio in Afghanistan.
Four-year old girl Fariba peeks from behind the gate and steps out on the street, followed by her father Mashal.
Mashal encourages his daughter to open her mouth to receive two drops of polio vaccine, and a drop of vitamin A. Fariba looks at the vaccinators with suspicion, but follows her father’s guidance.
The vaccinators thank them and continue down the street.
Locating all children
In March, vaccinators in Herat gave oral polio drops to over 150 000 children.
In a country with one of the highest rates of population growth in the world and frequent population movement, it is no easy feat to tell how many children live in each province, district, village, block, house or tent.
How do vaccinators know where the children in each area are located then? Through a simple but elegant guide known as a ‘microplan’. This is what the vaccinator follows: Where to start the day, how many children live on that street, which is the next house to visit?
No coincidence: Who goes where
A few kilometres from Fariba and Malik’s home, Dr Khushal Khan Zaman is sifting through printed plans on his desk at the World Health Organization office.
Dr Khushal explains that once a year, health workers physically count the houses in their area. Then they check that the plans from the previous year still match the numbers.
Campaign supervisors know the approximate number of children in each house from the last campaign. But the data is complemented by their personal knowledge. As locals, they often know of any changes in the composition of their community – where new children have been born, or the location of nomadic groups who have settled in the area.
This helps keep the plans accurate. For instance, if a nomadic group has stayed in an area for a longer time, their tents may be added to the microplans. For shorter stays, a separate checklist is used instead to monitor nomadic population movement. This improves the programme’s ability to trace and reach every child with vaccines, even if they are on the move.
Once the plans have been updated, teams of vaccinators are assigned to visit specific homes on a particular day during the upcoming campaign.
The final plan indicates not only the numbers of houses and children, but also details on how many related items are needed for each team: vaccine vials, vaccine carriers, ice packs (to keep the vaccines at optimum temperature), chalk, tally sheets, pens, leaflets, finger markers, plastic bags and scissors.
This is a contrast to a few years ago, when the plans listed only the name of the area with the estimated number of children to be vaccinated. The newer plans include even the smallest houses, and information on the closest mosque and local elders.
“It needs to be clear to everyone, which team is responsible for which area. We mark where the teams start and which direction they take using arrows,” Dr Khushal explains.
And it is no coincidence who goes where. To ensure that parents allow their children to be vaccinated, vaccinators may be allocated parts of their community that they know well, to increase trust when they deliver the vaccine.
Children like Fariba might not understand yet why the vaccine is important, but their father does. When vaccinators knock, it is not chance that brings them, but care and commitment.