The environment
Dar es Salam refugee camp, in Bagassola district, Chad, is home to thousands of refugees. 95% of the population is Nigerian, displaced by years of violent insurgency, drought and insecurity in the Lake Chad basin. Some have lived in the camp since 2014.
Here, temperatures soar to 45 degree Celsius nearly every day. Dust is inescapable, colouring everything a shade of yellow. Houses are constructed from tents, tarpaulins and reeds, pitched onto sand. There is no employment, few shops, and no green areas.

Kilometers from the lake, residents have no access to the water around which their livelihoods revolved, as fishing people, as traders at the markets located around the island network, or as cattle farmers. This renders them almost entirely reliant on aid. The edge of the camp is an enormous parking lot, filled with trucks loaded with donations. Signs interrupt the landscape, attributing the camp’s schools, football pitches, and water stations to different funding sources.
Polio immunization is a core health intervention offered by the health centre here, with monthly house to house vaccination protecting every child from the virus.
“We vaccinate to keep them healthy”
In return for their work, vaccinators receive a small payment, one of the few ways of earning money in the camp. In Dar es Salam, there are thirty positions, currently filled by 24 men and six women, and applications are very competitive. Those chosen for the role are talented vaccinators, who really know their community.

Laurence speaks multiple languages, adeptly communicating with virtually everyone in the camp. He is a fatherly figure, engaging parents in conversations about the importance of vaccination whilst his colleague gives vaccine drops to siblings. Their mother is a seamstress, constructing garments on a table under one of the few leafy trees. Laurence engages her in conversation, explaining why the polio vaccine is so important.
Describing his work, he says, “I tell parents that the vaccine protects children from disease, especially in this sun, and that we vaccinate every month to keep them healthy.”
A precious document in a plastic bag
Chadian nationals living in nearby internally displaced persons camps don’t have the same entitlements as international refugees. Several hours’ drive from Dar es Salam, children lack access to even a basic health centre.

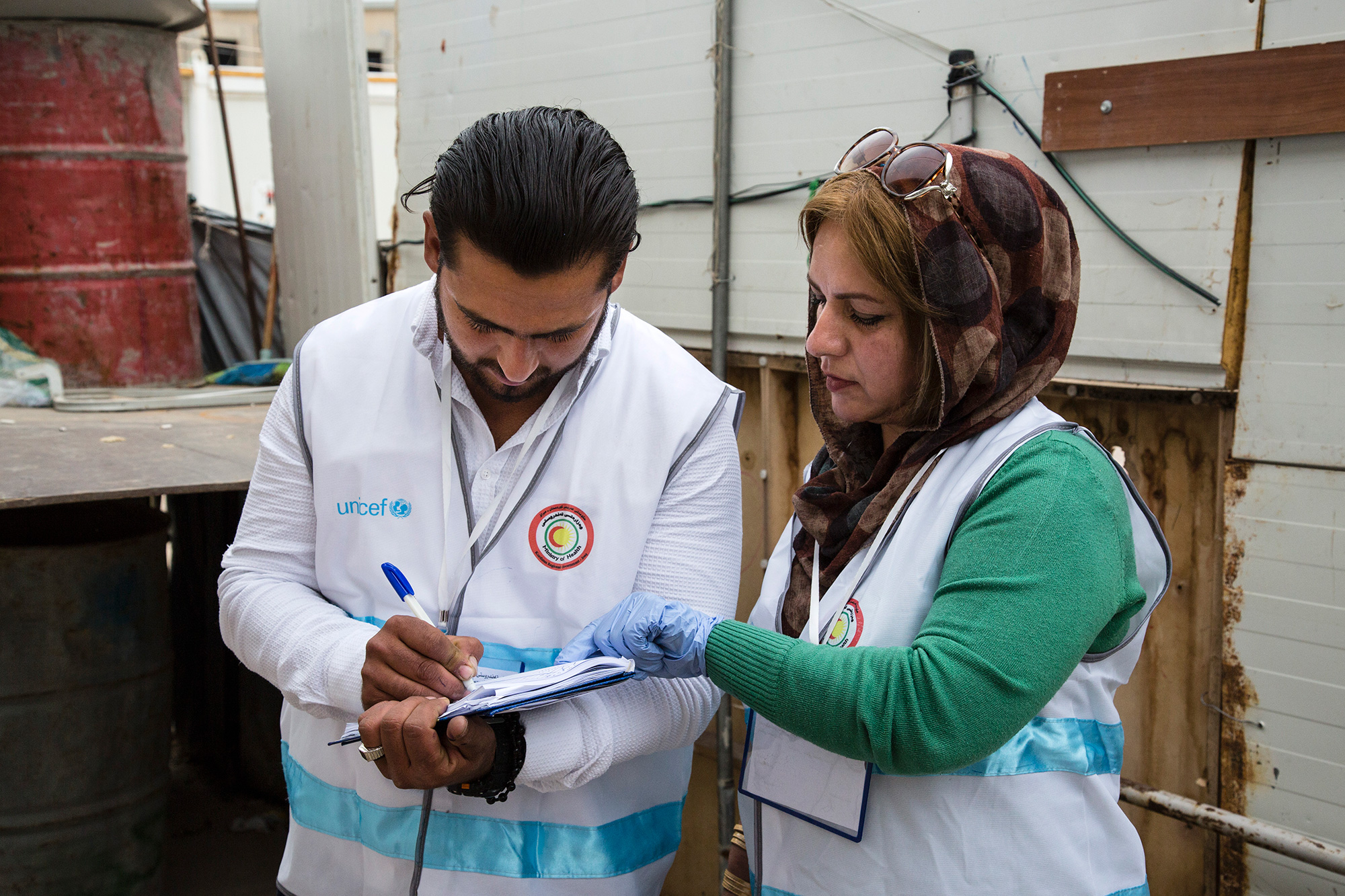
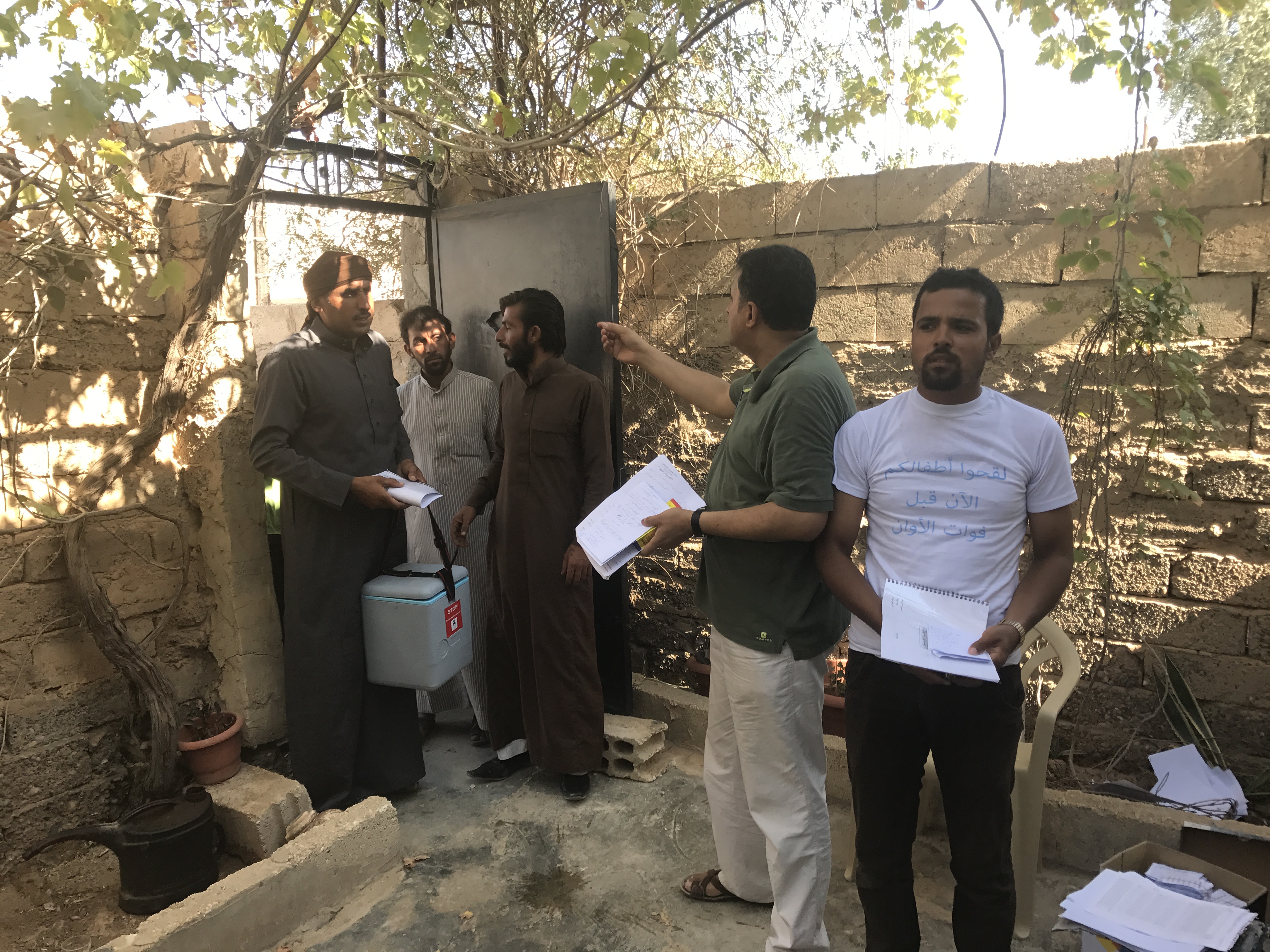
At a camp in Mélea, vaccinators perform routine immunization against measles and other diseases under a shelter made from branches. Cross-legged on the ground, they fill in paperwork, carefully administer injections, sooth babies, and dispose safely of needles. Other vaccinators give the oral polio vaccine to every child under the age of ten. These children are mostly from the islands, displaced by insurgency. Their vaccination history is patchy at best, and it is critical that they are protected.
One father arrives accompanied by his small, bouncy son. As the baby looks curiously at the scene in front of him, his dad draws out a tied plastic bag. Within is his son’s vaccination card, carefully protected from the temperatures and difficult physical environment of the camp.
A UNICEF health worker reads it, and realizes that the child is due another dose of polio vaccine. Squealing with confusion, the baby is laid back in his sibling’s arms, and two drops administered. The shock over, he is quickly back to smiling, rocked up and down as his dad folds up the card, and ties it up in the bag once more.

“Our biggest challenge”
Back in Dar es Salam, DJórané Celestin, the responsible officer for the health centre explains the wider challenges of vaccination in this environment.
“We don’t just vaccinate within Dar es Salam in our campaigns. We are also responsible for 27 villages in the nearby surroundings. Reaching these places proves our biggest challenge.”
Away from the main route to Dar es Salam, there are no roads or signs, and many tracks are unpassable. To reach the 539 children known to live in the villages, vaccinators walk, or rent motorbikes, travelling for many hours.
This month, another round of vaccination in the Lake Chad island region concluded. Hundreds more refugee and internally displaced children are protected, in some of the most challenging and under-resourced places to grow up.