A poliomyelitis (polio) vaccination campaign for children aged 6 months to 6 years who missed routine polio doses in the past will begin in Ukraine on 1 February 2022. This catch-up campaign is part of a comprehensive response to stop an outbreak of poliovirus first detected in Ukraine in October 2021. This first stage will last 3 weeks and is expected to reach nearly 140 000 children throughout the country.
Years of low immunization coverage in Ukraine have created a large pool of unvaccinated or under-vaccinated children who are vulnerable to polio. While routine immunization coverage has gradually increased over the past 6 years, in 2020, only 84% of 1-year-olds received the required 3 scheduled doses of polio vaccines by 12 months of age.
The immediate goal of the campaign is to reach the WHO-recommended level of 95% vaccination coverage of eligible children.
Background
The polio outbreak in Ukraine was confirmed on 6 October 2021. Poliovirus (circulating vaccine-derived poliovirus type 2) was first isolated in a 17-month-old girl in the province of Rivne who developed acute flaccid paralysis. Analysis of all her contacts found that 7 household contacts (siblings) and 8 community contacts in Rivne as well as 4 cousins in the province of Zakarpattya (who had had contact with the girl’s siblings) also tested positive, but did not develop paralytic symptoms.
A second case with acute flaccid paralysis (a 2-year-old boy in the region of Zakarpattya) also tested positive for poliovirus, with onset of paralysis in December 2021.
The isolated strain of the virus found in both paralytic cases and their contacts is linked to a poliovirus in Pakistan, which was also the cause of several cases in Tajikistan in 2020–2021.
Comprehensive plan to stop the spread of poliovirus
Following an initial local vaccination campaign, conducted where the first case was detected, a comprehensive polio outbreak response plan was approved by the Ministry of Health in December 2021.
The first stage of the plan will provide inactivated polio vaccine (IPV) to children aged 6 months to 6 years who have not received the required number of doses. In the second stage, all children under the age of 6 will be vaccinated with oral polio vaccine (OPV), even if they have received all their scheduled vaccination doses. This is necessary to protect children from infection and to stop the circulation of the virus. Dates for the second stage are pending.
With the ongoing COVID-19 pandemic, continued wild polio transmission in the remaining endemic countries and spreading outbreaks of circulating vaccine-derived polioviruses type 2 (cVDPV2), this year began with many challenges facing polio eradication efforts. But amid this new reality, countries and partners of the Global Polio Eradication Initiative (GPEI) intensified their efforts to protect children from lifelong paralysis.
In June, the GPEI launched the new GPEI Strategy 2022-2026, which lays out the roadmap to achieving a lasting world free of all forms of polioviruses through stronger community engagement, a renewed focus on gender equity and the rollout of new tools and technologies. These new tools include the novel oral polio vaccine type 2 (nOPV2), which began deployment under Emergency Use Listing (EUL) as part of the GPEI’s broader polio vaccine repository to curb cVDPV2 transmission. In August, the WHO African Region celebrated one year since it was certified wild polio-free, and countries recommitted to strong cVDPV2 outbreak response across the continent with the support of the GPEI.
Further critical progress took place in Afghanistan – one of two final countries endemic for wild poliovirus, along with Pakistan. For the first time in more than three years, nationwide polio immunization campaigns resumed across Afghanistan reaching 8.5 million children, including 2.4 million children who were previously inaccessible.
At the same time, polio programme health workers at the forefront continued to support global COVID-19 response efforts by delivering vaccines, mobilizing communities, and countering misinformation among other activities. The use of GPEI infrastructure for health emergency response has provided critical lessons for integrating polio resources into broader health systems as more countries work towards transition and the post-certification period.
Following dire predictions issued at the end of 2020, the polio programme once again proved its ability to adapt to programmatic, epidemiological and political developments. Entering 2022, there is much cause for cautious optimism – wild poliovirus transmission has slowed drastically, and cases of cVDPV2 have also declined compared to last year.
Importantly, commitment to achieving a lasting polio-free world is evident at all levels: by core GPEI partners, including among the Polio Oversight Board, which travelled to Pakistan twice in 2021; by health workers, communities and parents; and by country leaders worldwide who helped champion this year’s milestones. With the new strategy, new tools and adapted approaches, the stage is set to achieve lasting success.
To stop all forms of polio for good, the GPEI aims to capitalize on the positive epidemiological situation leading into 2022. A key opportunity to kick-start the year will be the WHO Executive Board meeting in January, where Member States plan to discuss building on the successes of this past year by fully implementing and financing the programme’s new strategy. Rotary and other key global GPEI partners are planning a renewed and intensified outreach across the broader international development community to secure the necessary financial resources to achieve success. Polio immunization campaigns will also continue in full force in both endemic and outbreak countries.
Twelve months ago, the programme was in a much different place, as WHO and UNICEF launched an Emergency Call to Action to draw attention to the need for renewed commitment. A year later, thanks to a strengthened and unified response, the GPEI is meeting the moment and is more committed than ever to end all forms of poliovirus, once and for all.
On 31 May, Tajikistan started a supplement immunization campaign against poliomyelitis to vaccinate all children under the age of six with two doses of oral polio vaccine. ).
Poliomyelitis (polio) returned to Tajikistan in the past year, with the first case of an outbreak of circulating vaccine-derived poliovirus type 2 (cVDPV2) detected in a child who developed acute flaccid paralysis (AFP) on 22 November 2020 in the province of Khatlon.
In response to the outbreak, 3 rounds of supplementation immunization with novel oral polio vaccine type 2 (nOPV2) were conducted, all of which reached a reported 99% of the target group of children under the age of 6.
Both environmental surveillance and active AFP case searches in hospitals and health facilities are continuing throughout the country to ensure that any potential further circulation will be detected.
The latest AFP case with confirmed cVDPV2 had onset of paralysis on 26 June 2021. The latest positive environmental sample was collected on 27 August, before completion of the third round of immunization in early September.
“Tajikistan has responded with full commitment and with the dedicated support of Global Polio Eradication Initiative partners to stop this outbreak,” said Dr Victor Olsavszky, WHO Representative and Head of the WHO Country Office in Tajikistan.
“We are cautiously optimistic that the extensive surveillance and immunization campaigns of the past 11 months have closed the door on further spread of this virus. This is vital for the health of children in Tajikistan and beyond.”
Extent of the outbreak in Tajikistan
As of 1 October 2021, 31 children have been found to have polio (paralysis) caused by cVDPV2, and the virus has also been isolated from 26 children without paralysis. Twenty environmental samples have tested positive for presence of the virus. All detected polioviruses are linked to a virus strain currently circulating in Pakistan.
The geographic spread of cVDPV2 (based on detection among children and in the environment) has been limited to Dushanbe city and 14 districts in the centre and south of the country.
Background
The oral polio vaccine (OPV) that has brought the wild poliovirus to the brink of eradication has many benefits: the live attenuated (weakened) vaccine virus provides better immunity in the gut, which is where polio replicates.
However, in communities with low immunization coverage, as the virus is spread from one unvaccinated child to another over a long period of time (often 12–18 months), it can mutate into a form that can cause paralysis, just like the wild poliovirus. This mutated poliovirus can then spread in communities, leading to cVDPV2 outbreaks.
The number of cVDPV2 outbreaks globally has increased sharply since early 2019. In 2020, cVDPV2 cases emerged in Afghanistan and were reported in areas close to Tajikistan, Turkmenistan and Uzbekistan.
nOPV2 is a new tool that Global Polio Eradication Initiative partners are deploying to better address cVDPV2. nOPV2 is safe and provides comparable protection against poliovirus, while being more genetically stable and therefore less likely to revert into a form that can cause paralysis in under-immunized communities. This means that nOPV2 could help stop cVDPV2 outbreaks.
WHO recommends that all countries, in particular those in which there is frequent travel to and contact with polio-affected countries and areas, strengthen surveillance for AFP and maintain high routine immunization coverage. All travellers to polio-affected areas should be fully vaccinated against polio.
Watch this animation to learn how the Global Polio Eradication Initiative (GPEI) intends to reinvigorate polio prevention and outbreak response with the bold new GPEI Strategy for 2022-2026.
In Ukraine, one case of polio, caused by circulating vaccine-derived poliovirus type 2 (cVDPV2), has been confirmed. A cVDPV2 was isolated from a 17-month old girl with acute flaccid paralysis, from Rivne province (in the north-west of the country), and from six healthy contacts (siblings of the girl).
The current isolate is closely linked to the virus originating in Pakistan which has also been a cause of ongoing cVDPV2 outbreak in Tajikistan. Local authorities, along with WHO regional and country teams, are conducting further investigations to determine the source of the isolated virus, whether there has been transmission within Ukraine, and to ascertain any potential risk of further spread. The Government of Ukraine officially notified WHO of the isolated virus on 3 October 2021 and publicly announced the case detection on 6 October 2021.
Supplemental vaccination of all young children in the affected area is planned to ensure catch up for any children who may have missed routine polio vaccination and ensure that all are protected from the disease. This will take place from 11 to 22 October with inactivated polio vaccine (IPV) for children aged less than five years of age, regardless of previous vaccination history, in the immediate area of where the case was detected. Additional vaccination activities will aim to cover the entire population of under-five year olds in this region over the coming 90 days.
In 2015, Ukraine was affected by a circulating VDPV type 1, resulting in two cases at the time. This outbreak was successfully stopped in 2016. An ambiguous VDPV type 2 was reported in Odesa province of Ukraine in 2016. The latest detection in Rivne is unrelated to the 2015 outbreak and 2016 isolation.
cVDPVs can occur if the weakened strain of the poliovirus originally contained in OPV passes among under-immunized populations for a prolonged period of time. If not enough children are immunized against polio, the weakened virus can pass between individuals and over time genetically revert to a form that can cause paralysis.
National coverage in Ukraine with the first dose of inactivated poliovirus vaccine—which protects against all three types of polioviruses—was 87% in 2020, according to WHO/UNICEF estimates. However, subnational coverage varies and is reportedly below 50% in some regions of the country.
VDPV outbreaks are stopped using the same tactics that have enabled progress against wild polio – ensuring every child is reached with polio vaccines through high-quality immunization campaigns and routine immunization.
Following careful review of safety and genetic stability data from mass immunization campaigns conducted with the novel oral polio vaccine type 2 (nOPV2), the Strategic Advisory Group of Experts on immunization (SAGE) today endorsed the transition to the next use phase for the vaccine. WHO’s independent Global Advisory Committee on Vaccine Safety (GACVS) and SAGE confirmed that there were no major safety concerns associated with nOPV2 after reviewing data from campaigns that used more than 65 million doses in Nigeria, Liberia, Congo and Benin earlier this year. Rollout of nOPV2 began in March and to date approximately 100 million doses have been administered to children across seven countries.
“The move is a positive and welcome advancement as GPEI and countries strive to bring cVDPV2 outbreaks to an end, and sees the achievement of a milestone outlined in goal 2 of our strategic plan: the goal to stop cVDPV2,” commented Aidan O’Leary, WHO’s director of polio eradication. “Not only does the decision inspire further confidence in nOPV2 as a safe and effective tool, it will facilitate a smoother preparedness process for countries looking to use the vaccine in the future,” he added.
“We are very pleased with the SAGE’s endorsement of transitioning nOPV2 to the next rollout phase. Progress like this is a result of strong partnerships at every level and we must continue forging forward together, using innovative tools like nOPV2, to reach every last child and end all forms of polio for good,” said Akhil Iyer, the UNICEF Director of Polio Eradication.
Ananda Bandyopadhyay, deputy director from the Bill & Melinda Gates Foundation and co-lead of GPEI’s nOPV2 Working Group stated, “Today is an important milestone in the road to polio eradication. Innovation has always been key to progress, and this tool – the first vaccine ever to be approved under WHO’s EUL pathway – is a shining example of how the GPEI responds to challenges, but the work is far from over.” BMGF is a core partner in GPEI and has funded the development of nOPV2 from its inception.
Requirements for rollout
Prior to this transition, countries were required to meet an additional set of strict criteria to use nOPV2 during its initial use period. These were developed by GPEI and endorsed by SAGE to allow for even closer monitoring of nOPV2’s performance during its introductory phase and early large-scale uses. While countries no longer need to meet these initial use protocols, use of nOPV2 remains subject to specific post-deployment requirements under EUL, such as monitoring for safety and effectiveness.
“As we move forward into the next phase of the vaccine’s rollout, countries will still need to meet special use requirements, but they will be less onerous,” said Simona Zipursky, WHO co-lead of the GPEI’s nOPV2 Working Group. “GPEI will continue to work with all countries who wish to roll out nOPV2 to help them meet these remaining criteria,” she added.
Optimal response with available vaccine
In addition to those who have already rolled out the new tool, 16 other countries are also verified as ready to use nOPV2 by GPEI and a further 17 are in the midst of preparations. More nOPV2 campaigns are due to launch later this year, however, supply of the vaccine is limited.
Active cVDPV2 outbreaks are ongoing in more than 20 countries across Africa and Asia and there have been recent detections of the virus in Europe. COVID-19 has impacted production of the vaccine, including by limiting supplies, available personnel and manufacturer capacity. GPEI is working with nOPV2’s manufacturer, Bio Farma, to increase supply as soon as possible and is accelerating efforts to bring a second manufacturer online. A GPEI prioritization framework will guide distribution of nOPV2 for the immediate term, until supply is increased.
“We are seeing sharp rises in demand for nOPV2, which is testament to the vaccine’s field performance, and we are working to increase supply as quickly as feasible,” said O’Leary. “We must be very clear though, that outside of nOPV2, there is no shortage of effective type-2 containing oral polio vaccines, and countries should not delay in responding to an outbreak. In line with SAGE’s guidance they should respond rapidly with whichever of the vaccines (mOPV2/nOPV2) is available to them,” he said.
With nOPV2 not yet WHO-prequalified, monovalent oral polio vaccine type 2 (mOPV2) ̶ nOPV2’s counterpart and close relative ̶ remains available to countries for outbreak response. The vaccine has a track record of successfully stopping cVDPV2 transmission and from 2019 to 2020, nearly 80% of outbreaks were closed following just two rounds of immunization. Trivalent oral polio vaccine (tOPV), containing all three vaccine serotypes, may be a more appropriate tool in situations where there is co-circulation of wild polio virus type 1 (WPV1) and cVDPV2.
“All OPVs can stop outbreaks,” said O’Leary. “Regardless of which vaccine is used, the key for any successful [outbreak] response is achieving high levels of vaccination coverage and quickly. That is what we need to remain mindful of and achieve. nOPV2 is only one of the effective vaccines in our toolkit and GPEI will continue to support countries to respond as rapidly as possible to outbreaks, as per the SAGE guidance.”
Next steps for nOPV2 development
Polio remains a Public Health Emergency of International Concern (PHEIC) under International Health Regulations, enabling nOPV2’s continued use through EUL. Field data collection and analyses will be ongoing to support the vaccine’s prequalification and full licensing, expected in 2023. Among other studies, a phase III clinical trial is currently underway in the Gambia.
The Global Polio Eradication Initiative (GPEI) is greatly concerned by the United Kingdom’s proposed cuts to contributions toward polio eradication in 2021. The proposed 95% reduction will result in an enormous setback to the eradication effort at a critical moment.
The UK has a long legacy as a leader in global health and its leadership in polio eradication, including financial contributions to the GPEI, have driven wild poliovirus out of all but two countries in the world. The GPEI values the UK government’s steadfast partnership and shared commitment to eradicating polio, and UK citizens have generously championed the drive to end polio. This has helped bring the world to the cusp of being polio-free, whilst providing an investment in broader public health capacity.
In 2019, the UK government pledged to help vaccinate more than 400 million children a year against polio and to support 20 million health workers and volunteers in this vital work. In addition to their life-saving work to end polio, these health workers have been in the frontline of the fight against COVID-19 and have helped some of the world’s most vulnerable countries protect their citizens. The UK’s ongoing support is needed to ensure that the polio infrastructure can continue supporting COVID-19 response efforts, while also resuming lifesaving immunization services against other deadly childhood diseases. In 2020, the UK government’s contributions ensured that the GPEI could continue to support outbreak response in 25 countries and conduct surveillance in nearly 50, all whilst strengthening health systems. The continuation of such support will not be possible unless replacement funds are identified, and as such, this funding cut will have a potentially devastating impact on the polio eradication program.
The GPEI recognises the challenging economic circumstances faced by the UK government and a host of other countries. Governments worldwide are making critical investments in the health of their citizens, as well as evaluating global commitments. Cutting the UK government’s contributions by 95% will, however, put millions of children at increased risk of diseases such as polio and will weaken the ability of countries to detect and respond to outbreaks of polio and other infectious diseases, including COVID-19. Furthermore, it risks delaying polio eradication and the dismantling of one of the most effective disease surveillance and response networks at a time when the COVID-19 pandemic continues its devastation.
GPEI looks forward to working with the UK and the broader global community to address these urgent issues, which jeopardize the collective investment and progress toward a polio free world. Together we can end polio forever and ensure that polio infrastructure and its assets continue to strengthen preparedness and response and save lives.
Dr Hamid Jafari, Director of Polio Eradication for WHO’s Eastern Mediterranean Region, declared Somalia’s outbreak of circulating vaccine-derived poliovirus type 3 (cVDPV3) closed a full 28 months after this strain of polio was last detected in Somalia.
Seven children were paralysed by the type 3 strain in the 2018 outbreak, and sewage samples regularly monitored for poliovirus tested positive for cVDPV3 a dozen times, beginning March 2018. There is no doubt that the virus circulated widely around southern and central Somalia. Despite extensive disease surveillance measures, no cVDPV3 has been identified since 7 September 2018, when the last child developed paralysis.
Closing a polio outbreak is a formal process steered by a detailed checklist of surveillance indicators that must be met in order to show that the virus is not just hiding in a far-flung pocket but has truly disappeared. Sewage runoff is tested for virus, and health workers and community members actively search for paralysis in children, and then investigate any paralysis they do find to rule out polio. Accessing hard-to-reach communities is a challenge in Somalia, but a vital aspect of this work.
The 2018 cVDPV3 outbreak was part of a 2-strain polio outbreak in Somalia at that time, along with circulating vaccine-derived poliovirus type 2. Both strains emerge and paralyse children in under-immunized populations – places where not enough children have consistently had access to polio vaccines. The cVDPV2 outbreak continues to paralyse children, and environmental samples – sewage water – consistently show that virus moving through Somali communities. For the polio programme, the presence of cVDPV2 samples and the absence of cVDPV3 samples is bittersweet: it demonstrates the sensitivity of our testing, so we can be confident cVDPV3 is no longer a threat to Somali children – but it makes clear that the threat of paralytic polio still looms.
Across the Region, cVDPV2 cases are on the rise – as across much of WHO’s African Region. Wild poliovirus still stalks children across Afghanistan and Pakistan, and the movement of people across borders underscores the risk of importation across and beyond the Region.
The end of Somalia’s cVDPV3 outbreak shows what can be achieved with high-quality vaccination campaigns, on-the-ground leadership and sensitive surveillance measures.
The new Regional Subcommittee brings together ministers of health from Member States across the Eastern Mediterranean Region to tackle some of the persistent high-level challenges to polio eradication. Those include raising the visibility of polio eradication as a regional public health emergency and priority and mustering the political support and domestic financial support needed to finish the job.
During the inaugural meeting convened by the Regional Director, Dr Ahmed Al-Mandhari, two co-chairs were elected to drive the regional push: Egypt’s Minister of Health and Population, H.E Dr Hala Zayed, and the Minister of Health and Prevention of the United Arab Emirates, H.E. Abdul Rahman Mohammed Al Oweis.
H.E. Abdul Rahman Mohammed Al Oweis was represented at the meeting by Dr Hussain Al Rand, the Assistant Undersecretary for Health Centres and Clinics and Public Health, United Arab Emirates. Both Member States flagged the urgency of the state of polio transmission in the last polio-endemic region at present, but also the opportunity to leverage greater regional coordination to achieve eradication.
Polio eradicators around the world know that ours is, in many ways, a grassroots programme: we use microplans to work through neighbourhoods door to door, household to household. But big-picture solidarity is needed to maximize the success of our ground-level efforts.
Wild poliovirus transmission has spread beyond core reservoirs of polio endemic Afghanistan and Pakistan, infecting 140 children in 2020. Outbreaks of circulating vaccine-derived poliovirus type 1 (cVDPV1) paralysed 29 children in Yemen. Type 2 outbreaks spread across the Region in 2020, paralysing 308 children in Afghanistan, 135 in Pakistan, 58 in Sudan and 14 in Somalia. At a time like this, moving forward as a region and as blocs, rather than on a country-by-country basis, is critical.
One of the issues identified by Member States as critical to stopping transmission is the movement of people across borders, and ensuring that surveillance and vaccination efforts target the increasing number of people who regularly cross borders across the region – whether they are moving as a consequence of conflict, environmental crises or economic necessity.
Interventions were made by Afghanistan, Egypt, the Islamic Republic of Iran, Iraq, Oman, Pakistan, Saudi Arabia and the United Arab Emirates. All statements reaffirmed strong support for the establishment of the subcommittee under the Regional Committee Resolution on polio eradication adopted in 2020.
Members of the subcommittee were unanimous in their commitment to engage in coordinated action and support of regional polio eradication efforts in four strategic areas. These include raising the visibility of the polio emergency in the Region, pushing for collective public health action, strengthening efforts to transition polio assets and infrastructure and advocating for the mobilization of national and international funding to achieve and sustain polio eradication.
A theme that ran through all Member States’ interventions was the idea of maximizing the resources already in place – including the workers, the polio and EPI infrastructure a across the region, and the array of community leadership groups with which the polio programme has worked in past.
“Last year or the year before the year before there was a meeting in Muscat with religious leaders from different countries, and I think we need to capitalize on their support. We need to give them ownership,” said Dr Ahmed Al Saidi, Minister of Health, Oman.
The COVID-19 pandemic has had an outsized impact on polio programmes across the region. The four-month pause in vaccination, from March-July 2020, gave the virus a window to spread almost unchecked. While we are immensely proud to have shouldered much of the COVID response burden, with GPEI infrastructure still supporting that response, this has come at a cost: nearly 80 million vaccination opportunities were lost.
“But we are moving forward, making up lost ground and, through this new Regional Subcommittee, leveraging the credibility that the polio programme has built through its pivot to COVID-19 and back again to polio,” said Dr Hamid Jafari, Director of the regional polio programme and co-facilitator of the Regional Subcommittee.
That credibility is now the polio’s most valuable asset: the proof that polio programmes are not just a means to battle polio, but sophisticated, fast-moving public health assets skilled in pandemic response.
The subcommittee will report its progress to WHO’s governing bodies meetings, including the World Health Assembly and the Regional Committee for the Eastern Mediterranean.
The Secretariat, which is made up of the office of the Regional Director and members of the regional polio eradication programme from WHO’s Eastern Mediterranean Region, will support the subcommittee to develop a programme of work based on the key outputs of the group.
From her first polio vaccination campaign in 1997 to the present day, Dr. De Sousa has never lost her passion for increasing access to immunization. The National Expanded Program on Immunization (EPI) Manager for Angola, she remembers her first impressions of the country, “At the time, I could see that most children in the country were not vaccinated and I was excited to help them.”
From the outset, she knew that taking on polio eradication would be challenging. “Angola had just emerged from an armed conflict and there were areas that were very difficult to access, due to dilapidated roads, broken bridges and mining activity, and for that reason there was low routine vaccination coverage. Nevertheless, I felt that I had a duty to fulfill for our children, so I accepted the challenge.”
In 1998, Dr. De Sousa was appointed by the National Directorate of Public Health to help implement the Epidemiological Surveillance System for Acute Flaccid Paralysis (AFP) – one of the primary symptoms of polio. It was a position that required grit and resilience.
She explains, “This was a big responsibility because highly sensitive surveillance for AFP, including immediate case investigation and specimen collection, are critical for the detection of wild poliovirus. AFP surveillance is also critical for documenting the absence of poliovirus circulation for polio-free certification.”
“One of my most vivid memories of the programme is from 1999 when I was trying to reach conflict-affected areas after a polio epidemic had registered more than 1190 cases and 113 deaths. I was early in my career with only two years of service and the sheer number of cases and deaths led me to be proactive and persistent in my day-to-day activities toward the eradication of the disease.”
“Another standout moment occurred on the second time that I went to coordinate a vaccination campaign in the province of Moxico; one of the vehicles in our convoy triggered a mine, so we were forced to stop the vaccination campaign as our colleagues were stranded in conflict zones for a few days. This incident captures the difficult circumstances we were operating in as health workers.”
Eradicating wild virus in Angola
For years the polio team worked to improve operations to detect polio and deliver vaccines, but the virus fought back. After registering a last case of indigenous wild poliovirus in September 2001, Angola recorded four successive outbreaks imported from India and Congo. Dr. De Sousa remembers that this caused many people to doubt that the eradication of polio would ever be possible.
“But I refused to be discouraged. I’ve never backed down from a challenge and I don’t plan to soon.”
After years of work, Angola finally received wild polio-free status in November 2015. Dr. De Sousa describes it as her proudest moment.
“I felt that I made a great contribution to my country and our children as the person managing the Extended Program on Immunization in Angola.”
A new challenge
In 2019, Angola’s immunization team faced a new challenge when the polio programme detected an outbreak of circulating vaccine-derived polio type 2, a type of polio that emerges in places with low immunity. Dr. De Sousa again found herself at the forefront of the action, starting by supporting the Government to respond with vaccination campaigns.
One of her key tasks since has been recruiting new immunization health professionals, who can help reach the children missed by routine immunization and polio campaigns. She explains, “my goal is to train my colleagues so that we can work together to reach the vast number of Angolan children missing out on lifesaving vaccines.”
In July 2020, Angola held its first polio campaign after a pause on vaccination activities in the early months of the COVID-19 pandemic. More than 1.2 million children were reached by over 4000 vaccinators.
Gender and leadership
Dr. De Sousa explains that being a woman leader in Angola isn’t easy. “It requires a lot of time, dedication and a balance with domestic, family, and social life, which has not been easy to manage. However, with the help of God and my family – especially my husband – I am managing to carry out my work.”
“It has all been worth it for the results I’ve helped to achieve, and even though we have some way to go in relation to vaccination coverage, I’m grateful for the opportunity to ensure the health of our children and serve my country.”
In Angola, at the provincial and municipal level, there are very few women compared to men. However, in public health programmes at the national level, women outnumber men. Dr. De Sousa says that, “In general, I think there should be more women leading and administering vaccination programmes”.
In 2021, the polio programme is aiming to implement more outbreak response vaccination rounds to reach children with low immunity to the poliovirus. Driven by her passion and sense of duty, Dr. De Sousa will continue to be on the frontlines of this effort.
N’Djamena – One of the largest polio immunization campaigns in the African Region this year has just concluded in Chad, where over 3.3 million children in 91 districts were vaccinated. This pushes the total number of children vaccinated against polio to over forty million across 16 countries in the Region, since campaigns resumed following a necessary pause in immunizations due to the COVID-19 pandemic.
While Africa was declared free of the wild poliovirus in August 2020, another form of polio continues to affect children: circulating vaccine-derived poliovirus, or cVDPV. This type of polio is rare and can only occur in areas where not enough children are immunized. The only way to stop spread of cVDPV is through immunization.
The current type 2 cVDPV outbreak in Chad was detected in February 2020—yet immunizations were halted due to COVID-19 and the virus spread to 36 districts across the country, paralyzing more than 80 children and even leading to cases in neighbouring Sudan and the Central African Republic.
“Viruses do not respect national borders,” said Dr Ndoutabé Modjirom, head of the polio Rapid Response Team at the World Health Organization (WHO) African Region. “Given Chad’s central geographic location and its mobile populations, it was important to carry out a large-scale campaign that targeted key populations and high-risk areas throughout the country.”
The vaccination campaign was carried out in two phases, the first taking place between 13-15 November and the second from 27-29 November.
While mass polio vaccination campaigns were stopped across Africa due to COVID-19 restrictions, they resumed in July 2020. The response in the region overall, and in Chad in particular, demonstrates the commitment by Global Polio Eradication Initiative partners and countries across Africa to stop polio, even amidst the difficult operating context of COVID-19.
“The number of children reached since polio campaigns have resumed is extremely encouraging,” said Dr Matshidiso Moeti, WHO Regional Director for Africa. “This large-scale campaign in Chad during COVID-19 is a reflection of the Region’s commitment and ability to face multiple difficult health challenges and protect the health of all children.”
Although campaigns were on hold for several months, work did not stop. Chad’s team of national and international polio experts together with the AFRO Rapid Response Team tracked the virus, conducted a comprehensive risk assessment, and planned an outbreak response to take place as soon as it was safe to do so, taking into account timelines in outbreak response standards of practice. Consultations were also held with the national COVID-19 task force to ensure that best practices in infection prevention and control would be followed. The commitment and efforts of the Ministry of Health and other key national and regional health leaders and partners, including UNICEF, were instrumental in conducting the campaign.
“With increased immunizations and the continued commitment of health leaders and partners, we are confident that we will soon see the end of this outbreak and the end of all forms of polio in Africa,” said Dr Jean Bosco Ndihokubwayo, WHO representative for Chad.
About polio eradication
The Global Polio Eradication Initiative is spearheaded by WHO, Rotary International, the US Centers for Disease Control and Prevention (CDC), UNICEF, the Bill & Melinda Gates Foundation and Gavi, the Vaccine Alliance.
On 6 November, WHO and UNICEF jointly issued an urgent call to action to avert major measles and polio epidemics as COVID-19 continues to disrupt immunization services worldwide, leaving millions of vulnerable children at heightened risk of preventable childhood diseases. Learn more about the call to action.
Fahima Ahmed Hassan is a 25-year-old community mobilizer who goes the extra mile to ensure parents of children under the age of five are informed of Somalia’s polio vaccination campaigns and are ready for their children to be vaccinated.
Fahima and the other mobilisers are from the local community and they lay the groundwork for vaccinators ahead of campaigns. They work tirelessly to reach every house, speaking to families to help them understand, trust, and accept the vaccine.
On a mid-October morning, children and their families are waiting anxiously. They have been informed, by Fahima and through loudspeaker announcements, that a team of vaccinators will be visiting their community.
Amid the COVID-19 pandemic, some people are concerned and worried about taking their children for vaccinations. They fear they might contract the virus or expose their children to it. Together with her team, Fahima takes every precaution to keep herself and the community she serves protected.
She explains that it is critical to show the community that vaccination can go ahead while maintaining physical distancing, wearing protective masks and using hand sanitizer.
Some people do not need to be convinced about the benefits of immunization. Asha Osman Yarow is one of them. She is patiently waiting for her son to be vaccinated.
“I decided to vaccinate my children because their health is important to me,” Asha says, holding her young son. “Vaccines protect children against diseases, like polio, measles and others.”
“Praise be to Allah that these services come to us,” chimes in Sahro Mohamed Haile. “I encourage all mothers to take care of their children, vaccinate them and keep records of their vaccination status. Me, I’m here today with my grandson,” she adds with a smile.
Others in the community are more reluctant to accept vaccines. “At first, I refused to vaccinate my children. I heard people say that the vaccines were no good and that they were made by non-Muslims. I was scared,” explains 30-year-old Wardo. “After speaking to the community mobilizers, I realized that the vaccines are good for my children’s health – and I changed my mind.”
“I understand where they are coming from, and I do my best to give them information and convince them that vaccinations are beneficial,” says Fahima. “Illiteracy, lack of education and myths make people reject the vaccines.”
Together with the other community mobilizers, Fahima engages elders, religious leaders and community influencers as well as urging parents until the very last minute to come forward.
“I’ve vaccinated all of my children and I was one of the first people in my community to support vaccines,” says Isha Hassan Saney, a fellow community mobilizer. She believes showing a good example helps to convince others in the community to vaccinate their children.
“I am motivated to serve the community, especially the mothers and children, because they need to be taken care of,” Fahima says. “There is no better reward than seeing them healthy.”
COVID-19 shows why vaccines are so important
Despite COVID-19, and the enhanced risk of infecting her husband and her extended family members when she comes home, Fahima continues to show up for work and doesn’t let fear take over.
The COVID-19 pandemic has revealed what is at stake when communities do not have the protective shield of immunization against an infectious disease. When vaccines are available, they are the most effective tool to prevent dangerous disease outbreaks.
Staying informed about their benefits and understanding the risks of not getting vaccinated has never been so important. Fahima and the other community mobilizers play an instrumental role in this.
During the recent polio immunization campaign, 8 951 vaccinators went door to door and 3 390 community mobilizers, including Fahima and her team, sensitized communities. The two-part campaign, organized by the Federal Ministry of Health, UNICEF and WHO, reached more than a million children under the age of five in south and central regions of Somalia.
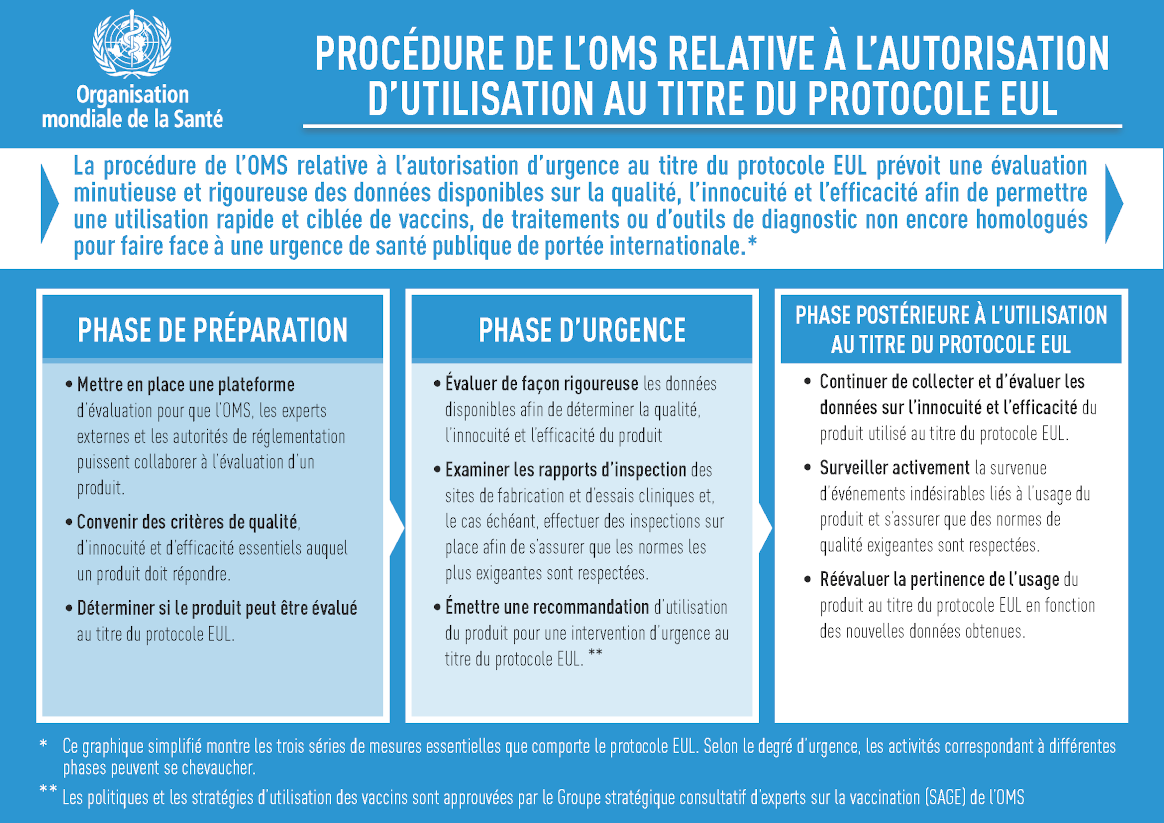
13 Novembre 2020 – Aujourd’hui, le programme de préqualification de l’Organisation mondiale de la Santé (OMS) a émis une recommandation d’autorisation d’utilisation d’urgence au titre du protocole EUL pour un nouveau vaccin antipoliomyélitique oral de type 2 (nVPO2). Le déploiement du vaccin sera ainsi autorisé pour une utilisation initiale limitée dans les pays touchés par des flambées de poliovirus circulant dérivé d’une souche vaccinale de type 2 (PVDVc2).
L’émission de cette recommandation au titre du protocole EUL pour le nVPO2 vient au terme de plusieurs mois d’analyse rigoureuse des données issues d’essais cliniques qui ont démontré l’innocuité du vaccin et une protection contre la poliomyélite comparable à celle fournie par le VPO monovalent de type 2 (VPOm2) actuellement utilisé.
Le nVPO2 est une version modifiée du VPOm2, mis au point depuis près de dix ans grâce à la collaboration d’un vaste réseau d’experts mondiaux.[1] Outre son innocuité et son efficacité, les essais cliniques montrent que ce vaccin est génétiquement plus stable que le VPOm2, ce qui réduit nettement la probabilité qu’il retrouve une forme pouvant entraîner une paralysie dans les milieux présentant un faible niveau d’immunité. Par conséquent, le nVPO2 réduit le risque de voir apparaître de nouvelles flambées de PVDVc2, même si le VPOm2 demeure un vaccin sûr et efficace qui protège contre la poliomyélite et qui a permis d’empêcher des flambées de PVDVc2 par le passé.
La procédure EUL de l’OMS, anciennement connue sous le nom de procédure d’évaluation et d’homologation en situation d’urgence de l’OMS (Emergency Use Listing, EUL), a été créée pour évaluer et répertorier les nouveaux vaccins, traitements et produits diagnostiques qui ne sont pas encore homologués afin qu’ils puissent être utilisés de façon précoce et ciblée en réponse à une urgence de santé publique de portée internationale (USPPI).
Ce mécanisme a déjà été utilisé avec succès pour accélérer la mise à disposition de produits diagnostiques pour les virus Ebola et Zika et, fin septembre, une autorisation d’utilisation d’urgence au titre du protocole EUL a été émise pour un test de diagnostic rapide de l’antigène de la COVID-19 qui donne des résultats en 30 minutes.
Pour qu’un produit reçoive une recommandation d’utilisation au titre du protocole EUL, l’OMS et des experts indépendants examinent les données cliniques existantes afin de déterminer son innocuité, sa qualité et son efficacité, et la décision d’émettre une recommandation est fondée sur une évaluation approfondie des avantages et des risques au vu de l’urgence de santé publique.
Pendant toute la durée d’utilisation d’un produit au titre du protocole EUL, on continue à recueillir des données et à les suivre de près afin de déterminer si ce produit peut recevoir une autorisation d’utilisation d’urgence au titre du protocole EUL.
Pourquoi le protocole EUL est-il utilisé pour lenVPO2 ?
Compte tenu des situations d’urgence actuelles concernant le PVDVc2 en Afrique et en Asie et du fait que la poliomyélite est considérée depuis 2014 comme une urgence de santé publique de portée internationale (USPPI), au mois de février, le Conseil exécutif de l’OMS a prié instamment les États Membres d’accélérer les procédures d’autorisation de l’importation et de l’utilisation du nVPO2 au titre du protocole EUL au vu des résultats prometteurs de ce vaccin dans la lutte contre le PVDVc2.
Les flambées de PVDVc2 se produisent lorsque la souche affaiblie du poliovirus contenue dans le vaccin antipoliomyélitique oral (VPO) peut se propager au sein de populations sous-vaccinées pendant une période prolongée et retrouver une forme pouvant entraîner une paralysie. L’année dernière, il y a eu 366 cas de PVDVc2 dans le monde. Au cours des dix premiers mois de 2020, on a recensé 588 cas (données au 28 octobre 2020).
Outre la décision du Conseil exécutif, le Groupe stratégique consultatif d’experts (SAGE) sur la vaccination a approuvé dans son principe un cadre définissant les critères d’une utilisation initiale pour permettre le déploiement rapide et ciblé du nVPO2. À la suite de sa réunion du 5 au 7 octobre, le SAGE a également approuvé, sur le principe, que le nVPO2 devienne le vaccin de choix pour lutter contre les flambées de PVDVc2, une fois que l’examen de la période initiale d’utilisation sera terminé et que toutes les conditions d’utilisation de ce nouveau vaccin seront remplies.
Des études cliniques sur le nVPO2, menées en Belgique et au Panama, ont montré que le vaccin était sûr et efficace pour protéger contre la poliomyélite, et qu’il présentait moins de risque de retrouver une forme pouvant entraîner une paralysie dans des populations sous-vaccinées.
Au cours des six derniers mois, le programme de préqualification de l’OMS a minutieusement analysé les données émanant de ces études afin de déterminer si le nVPO2 répondait aux exigences du protocole EUL. Grâce à la recommandation au titre de ce protocole, le nVPO2 constitue désormais un moyen supplémentaire de la Stratégie de lutte contre le PVDVc2 de l’IMEP.
Quelle est la période d’utilisation initiale du nVPO2 ?
Comme le précise le cadre approuvé par le SAGE, la période d’utilisation initiale durera environ trois mois après la première utilisation du nVPO2 au titre du protocole EUL, et ce vaccin sera déployé de manière mesurée dans la lutte contre les flambées de PVDVc2.
L’IMEP travaille étroitement avec les pays touchés par des flambées de PVDVc2 afin de déterminer où le nVPO2 peut être utilisé pendant la période initiale. Cette décision s’appuiera notamment sur la situation épidémiologique actuelle et sur la capacité du pays à mener la surveillance renforcée requise en termes d’innocuité et d’efficacité du nVPO2 pendant son déploiement.
Il est important de noter que toute décision d’utiliser le nVPO2 sera prise par le pays et soumise à l’accord des responsables concernés dans le pays et des autorités de réglementation nationales. Le VPOm2 restera disponible pour faire face aux flambées dans les pays qui ne répondent pas aux critères d’une utilisation initiale ou qui décident de ne pas utiliser le nVPO2 initialement.
L’utilisation initiale du nVPO2 devrait avoir lieu environ cinq à huit semaines après la publication de la recommandation d’utilisation au titre du protocole EUL, en tenant compte des processus réglementaires et des approbations définitifs, de l’achat des vaccins, de l’expédition et de l’état de préparation du pays. L’IMEP continue de travailler en étroite collaboration avec les pays à haut risque, en les aidant à se préparer à utiliser le nVPO2.
Perspectives d’avenir
On continuera à recueillir des données sur le nVPO2 pendant la période d’utilisation initiale, en plus des études en cours et de celles qui seront menées prochainement.
Parallèlement à l’utilisation initiale du nVPO2, l’IMEP poursuivra la mise en œuvre des autres volets de sa stratégie globale de lutte contre les flambées de PVDVc2. Cette stratégie consiste notamment à optimiser la riposte aux flambées en utilisant le VPOm2, à renforcer la vaccination systématique avec le vaccin antipoliomyélitique inactivé dans les zones à haut risque et à veiller à ce que les stocks de VPO soient suffisants pour que chaque enfant puisse en bénéficier.
[1] Le nVPO2 a été mis au point grâce à un partenariat mondial réunissant de multiples agences et experts internes et externes à l’Initiative mondiale pour l’éradication de la poliomyélite (IMEP). Il s’agit notamment de Bio Farma, de l’Université d’Anvers, de la FIDEC (Fighting Infectious Diseases in Emerging Countries), du NIBSC (National Institute for Biological Standards and Control), de l’UCSF (University of California San Francisco), des CDC (Centers for Disease Control and Prevention des États-Unis), de PATH et de la Fondation Bill et Melinda Gates.
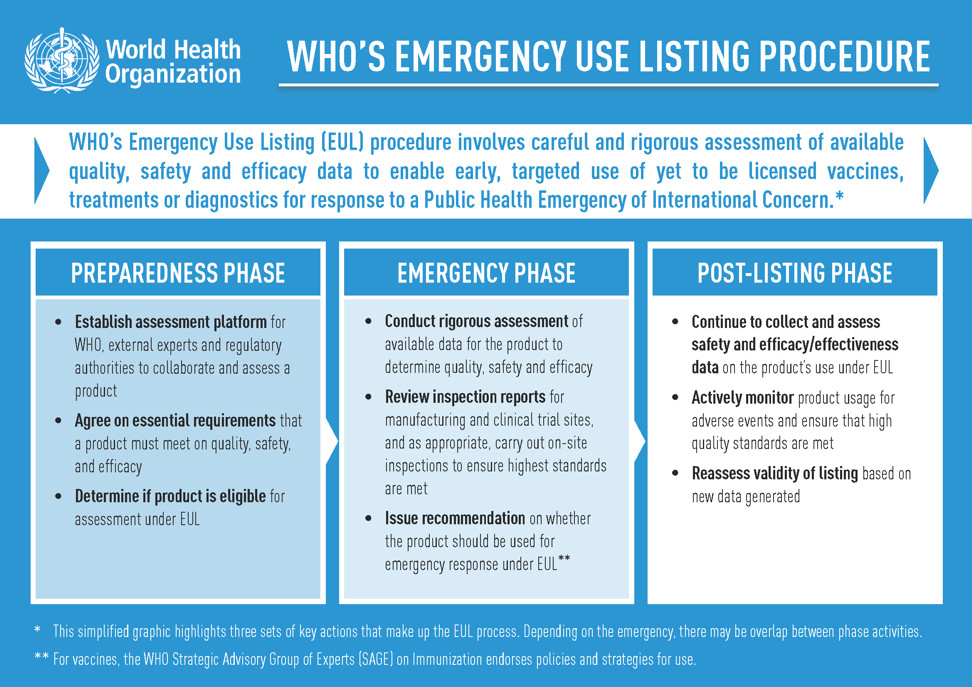
13 November 2020 – Today, the World Health Organization’s (WHO) Prequalification (PQ) program issued an Emergency Use Listing (EUL) recommendation for the type 2 novel oral polio vaccine (nOPV2). This will allow rollout of the vaccine for limited initial use in countries affected by circulating vaccine-derived poliovirus type 2 (cVDPV2) outbreaks.
The PQ program’s issuance of an EUL recommendation for nOPV2 follows months of rigorous analysis of existing data from clinical trials of the vaccine, that have shown it to be safe and provide comparable protection against polio as the currently used type 2 monovalent OPV (mOPV2).
nOPV2 is a modified version of mOPV2 and has been in development for close to a decade thanks to the collaboration of an extensive network of global experts.[1] In addition to nOPV2’s safety and efficacy, clinical trials show the vaccine to be more genetically stable than mOPV2, making it significantly less likely to revert into a form which can cause paralysis in low immunity settings. This means a reduced risk of seeding new cVDPV2 outbreakscompared to mOPV2, which remains a safe and effective vaccine that protects against polio and has successfully stopped cVDPV2 outbreaks in the past.
What is an Emergency Use Listing?
The WHO’s EUL procedure, previously known as the Emergency Use Assessment and Listing (EUAL) procedure, was created to assess and list new and yet-to-be licensed vaccines, therapeutics and diagnostics to enable their early, targeted use in response to a Public Health Emergency of International Concern (PHEIC).
This mechanism has previously been used to successfully accelerate the availability of diagnostic products for Ebola and Zika virus, and in late September, EUL was issued for an antigen rapid diagnostic test for COVID-19 that provides results within 30 minutes.
For a product to receive an EUL recommendation, existing clinical data is scrutinized by WHO and independent experts to determine its safety, quality and efficacy, and a decision to list is based on a thorough benefit-risk assessment considering the public health emergency.
Throughout a product’s use under EUL, data continues to be collected and closely monitored to help inform decisions about whether the emergency listing can be maintained.
Why is EUL being used for nOPV2?
In light of ongoing cVDPV2 emergencies across countries in Africa and Asia, coupled with polio’s status as a Public Health Emergency of International Concern (PHEIC) since 2014, the WHO Executive Board urged Member States in February to expedite the processes for authorizing the importation and use of nOPV2 under the EUL given data showing the vaccine’s promise against cVDPV2s.
cVDPV2 outbreaks occur when the weakened poliovirus strain contained in the oral polio vaccine (OPV) is able to spread among under-immunized populations for a prolonged period and reverts to a form that can cause paralysis. Last year, there were 366 cases of cVDPV2 globally, while in the first 10 months of 2020 alone there have been 588 cases (data as of 28 October 2020).
In addition to the Executive Board decision, the Strategic Advisory Group of Experts (SAGE) on Immunizationendorsed in principle an initial use criteria framework to support early, targeted nOPV2 rollout. Following its 5-7 October meeting, SAGE also endorsed, in principle, that nOPV2 become the vaccine of choice in response to cVDPV2 outbreaks after review of the initial use period is completed and all requirements for nOPV2’s use are met.
Clinical studies on nOPV2, conducted in Belgium and Panama, have shown the vaccine to be safe and efficacious in protecting against polio, while carrying less risk of reverting into a form that can cause paralysis in under-immunized populations.
Data from these studies has been subject to WHO PQ program’s rigorous analysis for the past six months to determine if nOPV2 meets requirements for EUL. The EUL recommendation means nOPV2 is now an additional tool in the GPEI’s Strategy for Control of cVDPV2.
What is the initial use period for nOPV2?
The initial use period, as detailed in the SAGE-endorsed framework, will last for approximately three months following the first use of nOPV2 under EUL and will see nOPV2 deployed in a measured way to tackle ongoing outbreaks of cVDPV2.
The GPEI is working closely with countries affected by cVDPV2 outbreaks to determine where nOPV2 can be used during the initial period. Factors that will inform this decision include the current epidemiology and the country’s ability to conduct the required enhanced monitoring of nOPV2’s safety and effectiveness during rollout.
Importantly, any decision to use nOPV2 will be country-led and subject to agreement from relevant in-country officials and national regulatory authorities. mOPV2 will remain available for outbreak response in countries that do not meet initial use criteria or choose not to use nOPV2 initially.
It is anticipated that the initial use of nOPV2 will take place approximately five to eight weeks after the EUL recommendation issues, factoring in final regulatory processes and approvals, vaccine procurement, shipping and country readiness. GPEI continues to work closely with high-risk countries, supporting with preparations to use nOPV2.
Looking ahead
Data on nOPV2 will continue to be collected during the initial use period, in addition to further nOPV2 studies that are underway and will be conducted in the near future.
Alongside nOPV2’s initial use, the GPEI will continue to implement the other strands of its comprehensive strategy to control cVDPV2 outbreaks. This includes optimizing outbreak response using mOPV2, strengthening routine immunization with inactivated polio vaccine in high-risk areas, and ensuring adequate supplies of OPV are available to reach every child.
[1] A global partnership across multiple agencies and experts from within and outside of GPEI have supported nOPV2’s development. This includes Bio Farma, University of Antwerp, Fighting Infectious Diseases in Emerging Countries (FIDEC), National Institute for Biological Standards and Control (NIBSC), University of California San Francisco (UCSF), US Centers for Disease Control and Prevention (CDC), PATH, the Bill & Melinda Gates Foundation, and several others.
Captain Nestor and Nurse Jeff support each other during polio vaccination campaigns in Barangay Bianoan, in Aurora in the Philippines. A barangay is the smallest administrative district in the Philippines, often home to a tightknit community. By combining their skills to raise vaccine confidence, publicize the campaign and share vehicles to reach every child with immunizations, Nestor and Jeff are playing a vital role to close the polio outbreak.
Meet more of the #HeroesEndingPolio in the Philippines, from nurses and laboratory workers, to Rotarians and polio campaign monitors.
Ismail Taxta/Ildoog/WHO Somalia
From 30 August to 3 September, Somalia conducted an integrated measles and polio campaign in the Banadir region – the first immunization campaign held since the COVID-19 pandemic reached Somalia. Over the last seven months, health workers have been fully engaged in fighting the pandemic. This campaign, conducted whilst observing safety measures to prevent spread of COVID-19, was a chance to get back on track to protect children who have missed out on vital immunizations.
Ismail Taxta/Ildoog/WHO Somalia
The campaign was conducted by Somalia’s Federal Ministry of Health, with technical support from WHO and UNICEF, and financial support from the Global Polio Eradication Initiative and Gavi, the Vaccine Alliance. The campaign had initially been scheduled to take place in 2019 as part of a nationwide effort, but was postponed due to technical challenges.
Ahead of the campaign, vaccines were procured and stored in optimum cool conditions. Microplans and maps were updated to help vaccinators reach all children at health facilities and fixed outreach sites. Building population immunity to polio and measles is extremely important in Somalia: Since the start of the year, 744 children in Banadir have contracted measles, accounting for half of the cases nationwide. Two forms of polioviruses, in circulation in Somalia since the end of 2017, have caused paralysis in 19 children across the country.
As part of the planning, 602 teams of health workers were given protective face masks and gloves, and were trained rigorously to keep themselves and their families safe from COVID-19. Every morning, they were checked to see if they had COVID-19 symptoms. Precautionary measures taken during the campaign included washing hands regularly, wearing face masks and ensuring physical distancing.
On the first day of the campaign, health teams set up fixed outreach vaccination sites and health facilities in different locations in Banadir. The aim was to reach as many children as possible: those living in urban and rural locations, those with nomadic lifestyles, and those living in camps for internally displaced persons.
All children under five who visited facilities during the campaign received deworming tablets and vitamin A, in addition to measles and polio vaccines. The inclusion of other health interventions in polio campaigns is a safe and effective way to help parents give their children the best possible protection against childhood diseases. This is particularly crucial in the Somali context, where children have limited access to health facilities, and population immunity is chronically low.
Two hundred and twenty-four district field assistants supervised more than 3000 vaccinators to ensure vaccinations were administered correctly and COVID-19 safety measures were observed. The campaign was also monitored by staff from the Ministry of Health, UNICEF and WHO.
Women and men played an important role in the campaign as social mobilizers, sharing messages on the benefits of vaccinations and COVID-19 prevention measures. Additionally, community volunteers helped to manage crowds of caregivers who visited health facilities and vaccination sites, ensuring that physical distancing was observed.
At the end of the day, all waste products from the campaign, including syringes, sharps and empty vials, were disposed of safely. By delivering multiple health interventions at once, cost savings can be achieved, and environmental impact is reduced when compared to delivering interventions separately.
Vaccination teams provided caregivers with vaccination cards for children, so that monitors could keep track of children who did not receive measles and polio vaccines.
Around 408 000 children aged between six months and five years (92% of those targeted by the campaign) received vaccinations against measles and 459 000 children aged under five (93% of the target) were vaccinated against polio. Ninety-two percent of children also received vitamin A and deworming tablets. This campaign proved that delivering health interventions amid COVID-19 in Somalia is achievable – and paved the way for subsequent campaigns to fill immunity gaps.
The WHO African Region is expected to be certified free of wild poliovirus on 25 August 2020. Chair of the WHO’s International Health Regulations Emergency Committee and of the AFRO Regional Immunization Technical Advisory Group Helen Rees explains the current cVDPV situation in Africa and its implications ahead of regional wild polio-free certification.
Q. Fifteen countries (as of 14 August 2020) in the World Health Organization’s African region have reported cases of circulating vaccine-derived polio type 2 (cVDPV2) in 2020. The total number of outbreak countries is 16. How does that impact the region’s upcoming wild polio-free certification?
First, it’s important to clarify that cVDPV is a different virus from the wild poliovirus, and will undergo a separate process to validate its absence once wild polio has been eradicated globally.
Second, I want to underscore that the ongoing cVDPV2 outbreaks in Africa do not affect the programme’s confidence that wild polio is gone from the region. Certification is backed by extensive data and a thorough evaluation process that demonstrates wild polio transmission has been interrupted on the continent.
In Africa, an independent body of experts called the African Regional Certification Commission for polio eradication (ARCC) oversees this process by carefully reviewing country documentation and analyzing the quality of surveillance systems and immunization coverage. With this intensive monitoring of polio programmes across the continent, the ARCC is able to confirm with 100% certainty that wild polio is gone from the region.
But for the ARCC, national polio programmes and GPEI partners, the work does not end here. Stopping cVDPVs remains an urgent priority. African countries will need to strengthen their efforts to reach all children with polio vaccines to protect them from cVDPVs and any importation of wild polio from the remaining endemic countries, Pakistan and Afghanistan.
How do cVDPV outbreaks happen?Andwhy has the number of cVDPV cases in Africa increased more rapidly in the past couple years while wild cases have not?
cVDPVs can occur if not enough children receive the polio vaccine. In under-immunized populations, the live weakened virus in the oral polio vaccine (OPV) can pass between individuals and, over time, change to a form that can cause paralysis—resulting in cVDPV cases. This means that the cVDPV outbreaks we’re seeing today are revealing pockets across the continent where immunization rates are too low.
The reason for the increase in cases can be explained by low immunity to type 2 poliovirus, which causes the vast majority of cVDPV cases. This is in part due to a global vaccine switch that occurred in 2016, when countries stopped using the trivalent OPV (which protects against all three forms of polio) and replaced it with the bivalent OPV (which protects against just type 1 and 3).
The GPEI, following the advice of the Strategic Advisory Group of Experts, decided to make this vaccine switch based on extensive evidence that showed it would decrease the number of cVDPV outbreaks. However, immunity to type 2 poliovirus was lower than predicated at the time of the switch and so there were actually more cVDPV2 outbreaks. In response to the cVDPV2 outbreaks monovalent oral polio vaccine type 2 (mOPV2) has been used to interrupt transmission. But with increasing numbers of children who do not have type 2 immunity, mOPV2 vaccines have had to be used longer and in larger quantities than was initially anticipated. This larger and more extensive use of mOPV2 vaccines has seeded new outbreaks especially in areas of low immunization coverage and on the borders of outbreak response zones.
All this said, mOPV2 is an effective tool to stop cVDPV outbreaks if children are properly immunized.
If cVDPV outbreaks can only affect under-immunized communities, doesn’t the increasing number of outbreaks indicate that polio immunity levels are too low across the region? Why were countries able to stop wild polio then?
For years, the wild poliovirus has only existed in a small area on the continent. Nigeria reported its last case of paralysis due to wild polio four years ago, but most other countries haven’t seen a wild polio case in quite some time.
Across the continent, population immunity levels to type 1 polio (the only type of wild polio that remains in the world) and surveillance networks have continued to protect against any wild polio importation from remaining wild polio endemic countries.
However, the increasing number of cVDPV outbreaks across Africa is a reminder that countries cannot afford to let their guard down, and must continue reaching every child with the polio vaccine.
What is the programme doing to address cVDPVs in Africa?
The same tactics that stop wild polio can be used to stop cVDPVs – high vaccination coverage and strong surveillance. The polio programme in Africa has proven experience and strategies to address cVDPV outbreaks. But we know that we cannot rely only on existing tactics, which is why the programme is innovating and adapting its strategies to address the challenge of cVDPVs specifically.
In early 2020, the GPEI released a comprehensive new strategy to stop cVDPV outbreaks currently affecting countries in Africa, Asia and the Middle East.
This includes revising outbreak response standard operating procedures to improve response time, doubling the size of the African Rapid Response Team, forming a global Rapid Response Team and prioritizing the GPEI’s ground presence in high-risk areas.
To raise immunization coverage, the GPEI partners – including Gavi, the Vaccine Alliance – are working to build and strengthen immunization systems in at-risk countries and expand routine immunization with the inactivated polio vaccine (IPV).
The strategy also includes the development of an additional tool to help stop cVDPV2 outbreaks – novel oral polio vaccine type 2 (nOPV2). nOPV2 is a modified version of the existing mOPV2 used to respond to cVDPV2 outbreaks that is less likely to change to a form that can cause paralysis.
The GPEI is confident that with strengthened commitment from country governments and full implementation of the tactics laid out in its strategy, cVDPVs can be wiped out across Africa.
Has COVID-19 affected the programme’s ability to stop cVDPV outbreaks in the region?
The recent pause in house-to-house polio campaigns to help control the spread of COVID-19 is expected to increase cVDPV transmission across affected countries.
The GPEI is taking a number of steps to get back on track. Even while campaigns were paused, surveillance activities continued so that as immunization activities ramp up the programme can target campaigns in areas that are most at risk.
The GPEI recently recommended that all countries with active polio transmission resume vaccination activities as soon as it is safe to do so, in line with WHO and national COVID-19 guidance. Burkina Faso and Angola were among the first countries to start implementing cVDPV outbreak response campaigns after the pause.
These campaigns are closely following safety guidelines and social distancing measures to protect communities and health workers against COVID-19. Measures including the use of masks and gloves, frequent handwashing and no-touch vaccination.
COVID-19 undoubtedly represents a setback for polio eradication, but not the first one the programme has faced. The GPEI and African countries’ national polio programmes are committed to ensuring that countries are ready to tackle the remaining challenge of cVDPVs and to recover lost ground once polio activities can safely ramp up.
“The road to the mountain village was rough. It’s only 50 kilometres, but it took more than 3 hours,” says Dr Fatima Ismail, a disease surveillance officer working in Somaliland. “We were bouncing in the car.”
In early 2020, Dr Fatima’s team headed to a remote village near Djibouti to check on a small boy. The boy’s right arm and leg showed a kind of paralysis that sometimes indicates polio. “The village polio volunteer in this mountainous area, geographically inaccessible, found an acute flaccid paralysis (AFP) case,” Dr Fatima remembers.
When children show signs of this paralysis, it is critical to get stool samples to a laboratory to determine whether they have polio. Polio teams ride camels in the desert or donkeys in the mountains when they have to. They brave conflict to get samples to laboratories. In brutally hot climates, they plug mini-freezers into car dashboards to keep samples cool.
All over the world, polio surveillance systems that have been built up over decades track infection sources, evaluate symptoms and transport samples to the laboratory — despite distance, natural disasters, and sometimes war. Now, disease surveillance network — reaching into the most far-flung corners of the globe — is being tapped to address the COVID-19 pandemic.
“In Somalia, the polio programme pivoted its workforce of thousands of frontline staff to support the effort as the cases of COVID-19 spread. Rapid response teams — made up of disease surveillance officers, community health care workers and volunteers — were trained to educate people about the virus and to test suspected cases. By April 2020, the teams were deployed in the field,” said Dr Mamunur Malik, WHO Representative in Somalia.
“In Somalia’s remote villages, they know us as their polio teams, and once they see us, what comes to their minds is that we’re giving them information about polio,” says Mohamed*, a surveillance officer. “So we also give them information about COVID-19. Social mobilisers tell them about COVID-19 symptoms, how to prevent getting infected, physical distancing, cleaning their hands very well with running water and soap.”
The careful procedures that the teams learned for polio surveillance have been adapted for COVID-19, where the required sample is a naso-pharyngeal swab. “We’ve trained our surveillance people on the case definition and how to collect the samples correctly, from people that meet the definition of a suspected case of COVID-19,” says Dr Fatima. “It’s the same infrastructure. After, when we collect the samples from the patient, we send it to the laboratory in Hargeisa.” WHO has given the laboratory equipment and supplies to test samples for COVID-19.
“As with polio samples, the samples of COVID-19 have to be refrigerated, the ice packs should be VERY cold,” says Mohamed. Teams are used to monitoring the packs’ temperature, even in Somalia’s hot weather.
“The logistical challenges we face with AFP/polio surveillance are still the same. This is the rainy season and the roads tend to be terrible,” says Mohamed. “You can’t get to certain places you normally get to, because of the situation on the road. Most of our vehicles can’t make it through the mud.” In those situations, teams work with other United Nations agencies to arrange special humanitarian flights to ship samples.
Frontline staff put their own lives on the line. In April 2020, the polio team lost a colleague due to COVID-19-related infection. Ibrahim Elmi Mohamed, who joined WHO in 2001, was working as a district polio officer in Lower Shabelle. His tragic death, one of many frontline staff around the world due to COVID-19, reminds us of the risks they face every day they go to work.
“Despite overwhelming challenges, teams are committed to continuing their polio work in tandem with the COVID-19 response. It is critical that polio surveillance continues during the pandemic, as Somalia is also fighting outbreaks of vaccine-derived polio type 2 and 3. With polio vaccination campaigns temporarily paused, the teams must be able to track any resulting spread of poliovirus and get ready to respond as soon as it is safe to do so,” says Dr Malik.
“All of us are still doing polio surveillance at the same time as we do surveillance for COVID-19,” says Dr Fatima. “I used to hear from my colleagues that the polio surveillance system is the strongest disease surveillance system. Any polio surveillance team can work in the detection of COVID-19 cases because of the system’s structure, the capacity and experience of the teams.”
Mohamed agrees. “My surveillance coordinator said don’t leave the AFP surveillance behind, follow that normal routine, don’t forget it and leave it aside.’”
As Somalia grapples with the COVID-19 pandemic, its trained teams are working quickly to prevent the spread of both COVID-19 and polioviruses. “What gives me hope in the COVID-19 response is when I look behind and I see what we have done with the polio teams, the impact we’ve had on so many lives,” says Mohamed. “We face everything and we overcome it.”
Noora Awakar Mohammad was only sixteen years old when she started working as a volunteer for the Polio Programme in Somalia. Since then, she has lived through civil war and armed conflict in her country, which have left the health infrastructure in tatters. Recalling the days of war, Noora’s face tenses. “During the civil war years, on many occasions the polio campaign was stopped because of intense fighting. As soon as the fighting would stop, we would run to communities to vaccinate children,” she recalls.
During those days, it was mostly elderly women and mothers who trained as vaccinators. The adolescent Noora had to work hard to build community trust. “Often, I stayed with the community and vaccinated the children amidst war. The community trusted me even though I was a young health worker,” she remembers.
Noora still faces challenges in her fight against polio. Many areas in Somalia are unreachable because of the presence of non-state groups. These groups, who oppose vaccination, have been responsible for creating fear among parents by spreading misinformation. Noora has also encountered vaccine-hesitancy among parents because of inadequate health awareness. “I have seen fathers refusing to vaccinate their children on one hand, while mothers request us to vaccinate them on the other. Under such trying circumstances, we have to seek the help of religious leaders to convince the refusing fathers,” Noora explains.
Alongside polio vaccination, Noora works as a midwife. As part of her role, she educates pregnant women and young mothers about the benefits of vaccination. She also builds awareness of Acute Flaccid Paralysis (AFP) in the community, a key symptom of polio. “I share information about AFP with mothers and now I see more and more mothers bringing their children to health centers even with the slightest symptom of AFP,” Noora says.
Noora emphasizes that closing the current polio outbreak in her country remains tough given the climate of insecurity and inaccessibility, but she remains determined to carry on with her work.
Zainab Abdi Usman is a midwife in Madina district in Banadir state in central Somalia. For the last twenty years, she has volunteered for the polio eradication programme. A source of frustration for Zainab is the children missing out on vaccination in inaccessible areas. The barriers health workers face to access populations in desperate need of basic healthcare and community services are sometimes insurmountable.
“During the civil war, I used to carry the vaccine in a thermos kettle to keep it cold and I would hide it under my Abaya. If fighters got suspicious, they would not allow me to go into the communities to vaccinate the children. Today, many areas remain inaccessible,” Zainab says.
Whenever the access situation changes, the polio programme is amongst the first health initiatives to reach children. Zainab explains, “In a conflict situation, there is an immediate need to treat victims of the conflict. However, at the same time, it is important that we save our children from paralysis resulting from polio. Therefore, reaching out to children in insecure areas is very crucial in our fight against the disease.”
Feriha Abdur Rehman Yusuf is the young mother of a one-year old boy. She sees the fight against polio as personal and has been part of over 30 immunization campaigns in Somalia.
An incident from Feriha’s past stays with her years later. “One day, during a door-to-door campaign, I knocked at the door of a house. A man carrying a gun opened it. He yelled at me and started shooting in the air. I was shaken for days,” she remembers. Thankfully, the situation has changed in Feriha’s district since then.
Thanks to efforts to educate parents, the public is more aware of the long-term benefits of vaccination. However, Feriha still faces a few families who reject the polio vaccine during campaigns. She tries to convince parents using the examples of her own son, and her nephews and nieces. If families continue to be worried, she seeks help from religious leaders and community members.
Working during campaigns is not easy for Feriha now she has her son. Feriha says that her mother is the biggest supporter of her work and source of encouragement. “When I am in the field during the polio campaigns, my mother practically moves into my house and takes care of my child,” she says.
Feriha believes that despite the climate of insecurity and inaccessibility, things are improving in Somalia. “Health services are getting better than before. More and more children are getting vaccinated, so they have a better shot at life,” she says.
7 February 2020 – Meeting in Geneva, Switzerland, Member States of the Executive Board expressed overwhelming support to the global effort to eradicate polio, in the face of an alarming polio epidemiology which emerged in 2019.
Last year saw an upsurge of wild poliovirus cases in Pakistan and Afghanistan, and an unexpectedly large number of circulating vaccine-derived poliovirus outbreaks. To address the situation requires new energy, and Member States strongly asserted their support to urgently achieve a world free of all strains of poliovirus.
Addressing the delegations, WHO Director of the Global Polio Eradication Initiative Michel Zaffran noted the strong response of Member States to 2019 setbacks: “Witnessing the efforts of colleagues, and the commitment of national governments, I feel personally confident and optimistic that we have begun to turn things around to ensure success. I see new commitments at country level. In Pakistan, a re-launch of the effort began midway through 2019. The programme undertook an in-depth analysis of the major area-specific challenges and their root causes, which they have now started to address.”
Eradicating polio in the remaining global wild poliovirus transmission block in Afghanistan and Pakistan is critical, as failure could result in global resurgence of the disease. Modelling indicates that within ten years, 200,000 cases would be reported worldwide, every single year. The risk of global spread of communicable disease has this year been underlined by the novel coronavirus (2019-nCoV) situation.
Member States also almost unanimously offered their support and commitment to closing outbreaks of vaccine-derived viruses (cVDPVs), endorsing new and concerted efforts. With Africa on the verge of being certified free of wild poliovirus, WHO Regional Director for Africa Dr Matshidiso Rebecca Moeti emphasised that the continent will continue to fully commit to eradication efforts until the cVDPV2 emergency is overcome. “New approaches and rapid response teams across the continent are intensifying their efforts in ensuring every child is reached during outbreak response, and that new outbreaks are rapidly detected and responded to.”
To this effect, the Executive Board endorsed in a Decision a new cVDPV2 outbreak response strategy, including accelerated roll-out of novel oral polio vaccine type 2 (nOPV2) to more effectively address the cVDPV2 health emergency currently affecting parts of Africa, the Middle East and the Southeast Asia region. Novel OPV2 – a brand new tool to address outbreaks – could be available to address this health emergency as early as mid-2020 under WHO’s Emergency Use Listing procedure.
The new vaccine, however, is only half the battle, cautioned Zaffran, stressing that resources and operational improvements are needed to ensure the vaccine reaches every last child. “We also need to implement stronger outbreak response and ensure more comprehensive surveillance, both things that cost money. With thanks to the generosity of the international development community, we have mobilized pledges of US$2.6 billion made at the Last Mile Forum in Abu Dhabi just two months ago. But this will not be enough to eradicate polio and tackle these increasing number of outbreaks. We are therefore calling on member states to mobilize domestic resources to respond to outbreaks, where possible.”
Zaffran continued: “On the horizon I witness a new epidemiological situation slowly beginning to emerge. I see a new, re-launched programme which has the building blocks in place to lead us to success. Let us not be under illusions however. This will not happen overnight and this will not be easy. The nature of the virus is that every operational improvement will take several months or longer to be reflected in epidemiology. This is the way polio eradication works: there is always a time-lag. So for now, we need to measure our progress in programmatic and operational success. We must continue our new commitments, action our new strategies, introduce new tools, monitor results and maintain our drive. Significant impact on epidemiology will subsequently follow.”
“We have a lot to do,” Zaffran concluded. “But the programme is starting 2020 on a very strong footing. I am convinced 2020 will go down in history as the year which turned the programme around, and back onto the path towards lasting success.”
Concluding the polio deliberations and speaking on behalf of 1.2 million Rotarians worldwide, Judith Diment, Chair of the Rotary Polio Advocacy Task Force, stated: “Rotary remains fully committed to the pursuit of a polio free world, as evidenced by our extended commitment to raise 50 million dollars annually through 2023. We urge all countries to devote the national financial and human resources needed to sustain high levels of population immunity through routine immunization, mitigate the risk of polio outbreaks and avoid significant unnecessary human and financial cost. The window of opportunity to achieve a polio-free world will not remain open forever. The time for urgent action is now.”
From a small prefabricated container where the walls host detailed maps and desks prop up computer screens beaming data, tables and graphics, the Rapid Response Team at the World Health Organization’s (WHO) Regional Office for Africa coordinate polio outbreak response. The team work across the continent, where 12 countries are battling the vaccine-derived strain of the virus.
Dr Ndoutabe Modjirom, a former Chadian university professor-turned WHO medical officer, coordinates the multi-agency team, which was formed in September 2019. It is composed of twenty experts in operations and vaccination management, epidemiology, logistics, and communications. They are drawn from the core partners of the Global Polio Eradication Initiative (GPEI): WHO, the United Nations Children’s Fund (UNICEF), Rotary International, the US Centers for Disease Control and Prevention, the Bill & Melinda Gates Foundation, and Gavi, The Vaccine Alliance.
The team is mobilized whenever a new polio outbreak is confirmed in the African region.
The first 72 hours
“Our work starts once the lab confirms that a sample collected from either the environment or a paralysed child is caused by a poliovirus. Every minute that passes after the lab confirmation means that the poliovirus is circulating and risks infecting more children,” says Dr Modjirom.
Within the first 72 hours, the Rapid Response Team deploys Team A. This team includes the GPEI Coordinator alongside an epidemiologist, an operations officer, a vaccine manager and a communicator for development. The team works closely with the health authorities in the affected country along with the relevant WHO and UNICEF country offices to prepare a risk assessment and outbreak response plan. The emergency response vaccination campaign, called ‘Round Zero’, starts within 14 days.
Team B takes over from Team A after the first eight weeks and continues the outbreak response activities.
According to standard operating procedures for responding to outbreaks, the polio programme must implement three rounds of high-quality vaccination campaigns in response to every outbreak. Parallel to vaccination, countries must intensify disease surveillance activities to detect new cases of acute flaccid paralysis, a clinical symptom of poliomyelitis.
“Priorities are constantly shifting for the Rapid Response Team,” says Dr Christopher Kamugisha, who has been working with WHO since 1998. He has been a member of the Rapid Response Team since its inception and like the rest of the team has been chasing new polio outbreaks across the region.
“In August I was in Somali Region in Ethiopia supporting the outbreak response, conducting the first vaccination campaign round. On the second day of the campaign, Dr Ndoutabe informed me that a new case was detected in Cheporoni in Ghana and asked me to go and provide technical support,” Dr Kamugisha recalls.
Within 24 hours, he was on a plane to Accra through Addis.
“I arrived at noon the next day and went straight to support the national technical team in their preparations and risk assessment. I assisted with ensuring that their plans are in line with the international standard operating procedures set by the GPEI,” Dr Kamugisha says.
No cure for polio
Polio is a viral disease, multiplying in the intestines and transmitted from person to person mainly through a faecal-oral route or, less frequently, through contaminated water or food.
While there is no cure for polio, the disease can be prevented through administration of a simple and effective vaccine. That is why efforts are underway across the country to rapidly boost immunity levels in children and protect them from polio paralysis.
Thanks to the efforts of the GPEI and country governments, no wild poliovirus has been detected anywhere in Africa since 2016. This stands in stark contrast to 1996, a year when wild poliovirus paralysed more than 75,000 children across every country on the continent.
In 2020, the central challenge for the African Region is overcoming outbreaks of circulating vaccine derived poliovirus. Vaccine-derived polioviruses are rare, but can affect unimmunized and under-immunized populations living in areas with inadequate sanitation and low levels of polio immunization.
Countries experiencing outbreaks of vaccine-derived poliovirus in Africa are Angola, Benin, Cameroon, Central African Republic, Chad, Côte d’Ivoire, Democratic Republic of the Congo, Ethiopia, Ghana, Nigeria, Togo and Zambia. Reasons these outbreaks have occurred include weak routine vaccination systems, vaccine hesitancy, difficulty accessing some locations and low-quality vaccination campaigns, which have made immunization of all children challenging.
In addition to the response activities, the Rapid Response Team work to build the capacity of health workers and decision makers in countries that are not experiencing polio outbreaks, training them to be ready to respond if virus is ever detected.
The team also aims to recruit more women with expertise in outbreak response. Achieving gender balance amongst personnel through a more equitable recruitment process forms part of the GPEI Gender Equality Strategy 2019 – 2023, which was launched in May 2019.
By supporting countries during outbreaks, and building health system resilience in vulnerable settings, the polio programme is working to establish a sustainable legacy that will improve health long after global eradication of the virus.
Brazzaville, 19 December 2019 – Kenya, Mozambique and Niger have curbed polio outbreaks that erupted in different episodes over the past 24 months, World Health Organization (WHO) announced.
Transmission of vaccine-derived poliovirus was detected in the three countries in 2018, affecting 12 children. No other cases have since been detected.
“Ending outbreaks in the three countries is proof that the implementation of response activities and ensuring that three rounds of high-quality immunization campaigns are conducted can stop the remaining outbreaks in the region,” said Dr Modjirom Ndoutabe, Coordinator of the WHO-led polio outbreaks Rapid Response Team for the African Region.
“We are strongly encouraged by this achievement and determined in our efforts to see polio eradicated from the continent. It is a demonstration of the commitment by Governments, WHO and our partners to ensure that future generations live free of this debilitating virus,” added Dr Ndoutabe.
Vaccine-derived polioviruses are rare, but these viruses affect unimmunized and under-immunized populations living in areas with inadequate sanitation and low levels of polio immunization. When children are immunized with the oral polio vaccine, the attenuated vaccine virus replicates in their intestines for a short time to build up the needed immunity and is then excreted in the faeces into the environment where it can mutate. If polio immunization coverage remains low in a community and sanitation remains inadequate, the mutated viruses will be transmitted to susceptible populations, leading to emergence of vaccine-derived polioviruses.
No wild poliovirus has been detected anywhere in Africa since 2016. This stands in stark contrast to 1996, a year when wild poliovirus paralysed more than 75,000 children across every country on the continent. The WHO African Region however, is currently facing outbreaks of a rare poliovirus strain known as circulating vaccine derived poliovirus.
The work of the Rapid Response team starts once the lab confirms that a sample collected from either the environment or a paralysed child is caused by a poliovirus. Every minute that passes from then means that the virus is circulating and risks infecting more children that is why the Rapid Response Team deploys with 72 hours. The team supports local health authorities in the affected country in preparing the risk assessment and outbreak response plan. Then assist with launching the emergency response vaccination campaign, called round zero, within 14 days. A second team then takes over after the first eight weeks and continues the outbreak response activities including ensuring that three more rounds of high-quality vaccination campaigns are conducted.
To end outbreak activities in an affected country national and regional disease surveillance and laboratory teams need to confirm that no polio transmission is detected in samples collected from paralysed children, children in contact, and the environment have been negative for at least nine months. Response to the polio outbreak requires a strong multisector collaboration. In these efforts, WHO with other Global Polio Eradication Initiative spearheading partners: UNICEF, Rotary International, the US Centers for Diseases Control (CDC), the Bill and Melinda Gates Foundation (BMGF) and other stakeholders have been supporting the Government of Angola in implementing measures to end the transmission of the poliovirus.
Countries still experiencing outbreaks of vaccine-derived poliovirus in Africa are: Angola, Benin, Cameroon, Central African Republic, Chad, Côte d’Ivoire, Democratic Republic of the Congo, Ethiopia, Ghana, Nigeria, Togo and Zambia. The risk factors for these outbreaks include weak routine vaccination coverage, vaccine refusal, difficult access to some locations and low-quality vaccination campaigns, which have made immunization of all children difficult.
Countries of the region experiencing outbreaks are continuing to implement outbreak response, following internationally-agreed guidelines and strengthening surveillance activities to rapidly detect any further cases. To successfully implement the outbreak response required, the engagement of government authorities at all levels, civil society and the general population, is crucial to ensure that all children under the age of five are vaccinated against polio.
Health workers and community volunteers in remote and security-compromised areas across ten African countries now rely on an SMS-based application to ferret out any possible poliovirus hiding in their midst.
The application is called AVADAR, short for “auto-visual AFP detection and reporting”, with AFP referring to acute flaccid paralysis, which is the main visible clinical symptom of poliomyelitis. AVADAR is an SMS-based mobile application used for reporting, monitoring and surveillance of poliovirus. It was developed in 2016 by the World Health Organization (WHO), in collaboration with the Bill & Melinda Gates Foundation and the Swiss software company Novel-T, to ensure that every case of wild poliovirus is detected.
On a weekly basis, the health workers and volunteers in selected hard-to-reach districts use the AVADAR application to report whether they have noticed any child with paralysis of a limb. The districts are selected based on being deemed high risk yet having the sufficient telecommunications infrastructure that allows the health workers and community volunteers to communicate with the investigations team.
“In the last mile of polio eradication, we are not sparing any resources to reach a polio-free world. That is why we developed the AVADAR app,” says Dr Pascal Mkanda, WHO Regional Coordinator of the Polio Eradication Programme for Africa.
In the WHO African Region, no outbreaks of wild poliovirus have been detected since 2016, when the last case was found in Nigeria’s Borno State. This brings the region closer towards being certified free of wild poliovirus in 2020.
Health workers and community volunteers use AVADAR to recognize and report cases of acute flaccid paralysis, which is the sudden onset of paralysis or weakness in any part of the body that can be caused by polio, among children younger than 15 years. Acute flaccid paralysis could be caused by other diseases than poliomyelitis.
“Polio eradication requires that the surveillance system is sensitive enough to detect all acute flaccid paralysis cases -regardless of the disease behind it- and that such cases are promptly reported and investigated by disease surveillance personnel. This system starts at the community level,” Dr Mkanda adds.
Health workers and community volunteers first received training in workshops on how to use AVADAR and then they were each handed a smartphone with the application installed. On a weekly basis, the app sends them video reminders illustrating acute flaccid paralysis cases. The app then asks: “Have you seen a child with weakness of the legs or arms that you have not previously reported?” They then select between yes or no. If yes, the health workers and community volunteers input extra information about the case, such as the child’s name, date of onset of symptoms and geographic information.
Once the health worker presses the “send” button, a text message is sent to a system that triggers the sending of an SMS to the government and a WHO team that will investigate the case.
“In the AVADAR training workshops, we realized that some health workers and the majority of volunteers do not know the implications of acute flaccid paralysis and are unable to accurately identify such cases within their communities. The weekly AVADAR reminder videos helped improve that significantly,” says Dr Godwin Akpan, WHO Regional Polio Data Manager for Africa.
Dr Godwin is part of the team behind the innovation of the AVADAR application and trains health workers and community members on its use.
AVADAR was first piloted in Nigeria in 2016 and has been rolled out since 2017 in 99 districts of ten African countries: Burkina Faso, Cameroon, Chad, Democratic Republic of the Congo, Liberia, Mali, Niger, Nigeria, Sierra Leone and South Sudan.
As of October 2019, AVADAR has detected 1019 confirmed acute flaccid paralysis cases after health workers and community volunteers sent out 25,747 alerts through the application. None of those cases were polio cases. This marks a significant enhancement to the existing surveillance system that faces difficulties in remote and high-risk areas.
“Innovation and new technologies are our hope to finally make the feat of eradicating polio a reality. Thanks to the Global Polio Eradication Initiative, today, we are closer than ever to eradicating polio,” concludes Dr Mkanda.
When we visited Junaisa in her relative’s home in Lanao del Sur in the southern part of the Philippines, she was timid with a fever. Despite feeling under the weather, she was well-behaved and quietly clung to a jar of snacks.
Junaisa’s mother, Salma, told us that the toddler is usually chatty when there are no visitors around. But Salma explained that Junaisa has gradually become frightened of people, especially those wearing white, ever since she was admitted to the hospital a few months back.
“Junaisa was healthy,” shared Salma. “She was full of energy when she was walking.”
The last time the three-year-old was able to stand up and walk on her own was in June. She stood up, used the chamber pot and fell down.
“A sample of her faeces was brought to Manila; they did everything. And then the pediatric doctor told us they’ll call about the results,” said Salma. “After around two months or over one month, that’s when we found out. It was polio.”
Read more of Junaisa’s story on the World Health Organization Western Pacific regional site. Her name, photograph, and story are published with permission from her mother Salma.
Abdullahi Mahamed Noor, hailing from Mogadishu in Somalia, wears multiple hats. By day, he is an experienced and dedicated polio programme zonal coordinator. By night, you can find him racing down the court as president of the Somali Basketball Federation.
Mahamed’s journey to end polio started in 1999, as a vaccinator in Adale District of Middle Shabelle in Southern Somalia. Since then, he has worked to combat multiple polio outbreaks in his country, including the current cVDPV outbreak.
Mahamed strongly believes that eradicating polio isn’t just about delivering the vaccine. To maintain high immunity levels, the programme must deliver a clear message about the safety and importance of the vaccine and help communities become better informed. To achieve this goal, Mahamed uses his sporting connections to combine basketball with innovative polio immunization messages, with the objective of increasing awareness throughout his community.
Last year, Mahamed took advantage of a Vaccination Week to deliver messages on polio eradication at several basketball games held in Mogadishu. “When people come to the stadium, they see messages on polio awareness and how important it is to vaccinate children to build their immunity against polio virus. They pass those messages to family and community members,” he explains.
From 1999 to 2010, a period during which Somalia suffered several polio outbreaks, the inaugural ceremonies of most of the major sports activities in Somalia would begin with statements encouraging people to vaccinate their children against polio.
Currently, Mahamed supports polio officers to develop comprehensive microplanning for immunization campaigns in Somalia. He emphasizes fostering trust between frontline workers and communities, since the polio workers in Somalia travel door to door to deliver vaccine. The basketball games that he organizes in his spare time help to increase acceptance of polio workers in the community.
“Part of my job is to convince the families who refuse to vaccinate their children. I quite often use my experience of being involved in basketball to educate them on benefits of polio vaccination and preventing disability related to poliovirus.”
Sportspeople are active in the fight to end polio the world over. Ade Adepitan, a British Paralympian, wheelchair basketball player and broadcaster, who is himself a polio survivor, is a strong advocate for polio eradication. In Pakistan, cricketers often promote polio eradication campaigns during the highly watched and well-attended matches.
In many parts of Somalia, poverty, conflict, internal displacement and weak health infrastructure often mean that vaccination levels remain relatively low. Amidst these trying circumstances, dedicated workers like Mahamed are playing a critical and innovative role in educating communities about polio and the absolute importance of vaccination to defeat the disease.