News Category: Outbreak countries
The programme is focusing on reaching zero-dose children (children who are either un- or under-immunized), in identified ‘consequential geographies’.
But what exactly are consequential geographies, and why are they so vital to the global effort to eradicate polio?
In this explanatory video, long-time polio eradicator and Director for polio eradication at WHO’s Eastern Mediterranean Region, Dr Hamid Jafari, explains more.

2022 may well go down in history as the year of contrasts in the global effort to eradicate polio. At first glance, with polio detections in places such as New York and London and an increase in cases in Pakistan, it may seem that the effort is backsliding. And while any detection of any poliovirus is a setback—particularly in areas where the disease had been long gone, like southeast Africa—a deeper analysis reveals a more encouraging story: 2022 saw perhaps some of the most significant progress in the programme’s history, and has set up the global polio effort for a unique opportunity to achieve success in 2023.
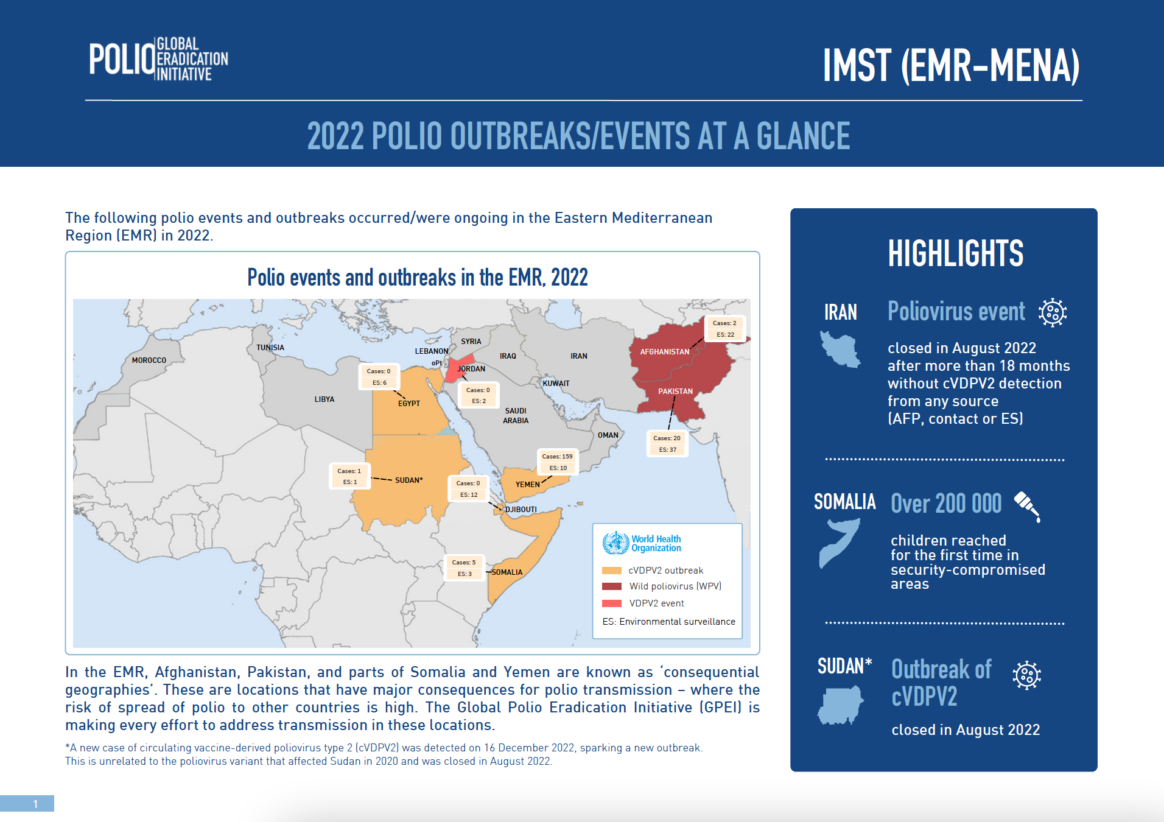
Endemic wild poliovirus transmission in both Pakistan and Afghanistan is becoming increasingly geographically restricted, with fewer virus lineages remaining active. The bulk of variant type 2 polio (cVDPV2) cases are also becoming more restricted, with 90% of all global cases restricted to three ‘consequential geographies’ (eastern Democratic Republic of Congo, northern Yemen and northern Nigeria). And emergency outbreak response efforts to wild poliovirus type 1 in southeast Africa continue to gain momentum.
To evaluate this progress as 2022 draws to a close, independent technical expert and advisory groups are taking an in-depth look at the prevailing epidemiology, assessing impact of eradication efforts and putting forth key strategic approaches to enable an all-out effort against the virus in the first half of 2023.
The first of these groups met in early October, when the Technical Advisory Group (TAG) for Pakistan reviewed vaccination coverage and disease surveillance across the country. Despite the increase in new cases, the TAG found the outbreak to be extremely geographically confined, thanks to concerted emergency efforts led by the government and supported by partners. Today, polio transmission is restricted to the six districts of southern Khyber Pakhtunkhwa province—a fraction of the country’s 180 districts. Encouragingly, the virus has not re-established a foothold outside the core outbreak zone, meaning the traditional reservoirs of Karachi, Peshawar and Quetta are no longer endemic to the virus, a historical first.
More good news came out of the TAG’s analysis of the genetic biodiversity of virus transmission. In 2020, Pakistan had 11 separate chains of virus transmission. This was reduced to four in 2021, and today, just one family of the virus remains in the country. The approaches being implemented in Pakistan are working—despite some serious challenges.
In September, Pakistan experienced catastrophic flooding that impacted more than 33 million people and submerged one third of the country under water. In the face of this tragedy, and despite being affected themselves, polio staff supported the broader relief efforts while adapting polio operations to ensure that the eradication effort could continue unabated. Long-time polio eradicator and Director for Polio Eradication in WHO’s Eastern Mediterranean Region, Dr Hamid Jafari, said: “Rarely have I seen such commitment and dedication than I have seen in Pakistan – from national leaders, to health workers, right to the mother and father on the ground.
They are making a huge difference to people’s lives, which goes far beyond the effort to eradicate polio.”
In December, a high-level delegation led by GPEI Polio Oversight Board (POB) Chair Dr Chris Elias, WHO Regional Director Dr Ahmed Al-Mandhari and UNICEF Regional Director George Laryea-Adjei visited Pakistan during a nationwide vaccination campaign. After meeting with women health workers, provincial and national polio coordinators and even the Prime Minister, the group concluded that there is unprecedented support and commitment to ending polio in the country in 2023.
In Afghanistan too, an epidemiological deep dive reveals a promising picture: just over twelve months on from the political developments in the country in 2021, access to all children in the country continues to improve, albeit against a tragic backdrop of a severe and acute humanitarian crisis. More than 3.5 million children in Afghanistan who had been out-of-reach for almost five years can now be reached with polio vaccines, and thanks to strong vaccination and disease surveillance efforts, polio transmission has been restricted to just two chains in two provinces. And following the country’s devastating earthquake in June, polio teams sprang into immediate action to both support the broader emergency relief effort and adapt polio operations.
This progress in Pakistan and Afghanistan is identical to what epidemiologists observed during the ‘end game’ efforts in global polio reservoirs in the past, notably Nigeria, India and Egypt, giving rise to optimism that these remaining two endemic countries are on the right track.
Expert groups focus on outbreaks…
2022 saw a number of high-profile polio events, like the detections in New York City and London, but it is important to recognize the distinction between these and the outbreaks that have the capacity to endanger, or at least significantly delay, the global eradication goal.
Aidan O’Leary, Director of the Global Polio Eradication Initiative (GPEI) at the World Health Organization (WHO), contextualized the situation: “90 percent of global media attention has been on the polio emergence in New York, London and Israel. However, 90 percent of actual cases are in eastern Democratic Republic of Congo, northern Yemen and northern Nigeria.” It is in those areas, commonly referred to as consequential geographies, that programmatic efforts must maintain their focus. Notably, these areas also overlap with some of the highest proportions of ‘zero-dose’ children—those who are either un- or under-vaccinated.

While the outbreaks in northern Yemen and eastern DR Congo continue to expand at an alarming rate in 2022, the situation in northern Nigeria is far more encouraging. Nigeria accounted for two-thirds of all global cases in 2021, seeding outbreaks in 19 countries. In the second half of 2022, however, there has been a dramatic decrease in new detections, with just nine cases reported during that time.
In November, the Nigerian Government, with GPEI partners in attendance, hosted the Global Roundtable Discussion on variant type 2 polio outbreaks, reviewing progress in outbreak response following the upsurge in cases in 2021. The Roundtable recognized efforts to reach zero-dose children in consequential geographies throughout the country, in particular with the novel oral polio vaccine type 2 (nOPV2), as well as Nigeria’s focus on strengthening routine immunization with bivalent OPV and inactivated polio vaccine (IPV). Whichever strategy is used, however, the group cautioned: “coverage is king!” Any vaccine is only as good as the proportion of children it reaches.
The group’s conclusions and recommendations will be further evaluated by Nigeria’s Expert Review Committee on Polio Eradication and Routine Immunization (ERC).
Meanwhile, in southeast Africa, a comprehensive Outbreak Response Assessment reviewed the regional response to wild poliovirus type 1 (WPV1), linked to virus originating from Pakistan, with cases confirmed in Malawi and Mozambique. Experts noted the high-level, comprehensive support for the outbreak response across the region, and that vaccination campaigns have been consistently improving with time.
At the same time, the group concluded that the outbreaks are not over. With simultaneous outbreaks of WPV1, cVDPV1 and cVDPV2 affecting in particular Mozambique, the group put forward key recommendations and strategies, building on the momentum and knowledge gained over the past six months. These conclusions were further endorsed by the Africa Regional Certification Commission for Eradication (ARCC), which met in South Africa.
Challenges remain ahead. Zero-dose children must be reached, particularly in consequential geographies. Remaining financial resources to achieve success must be mobilized. Campaigns must be strengthened in southeast Africa. But despite initial appearances, 2022 put the world on an extremely strong footing to interrupt all remaining chains of poliovirus transmission by end 2023—the goal of the GPEI Strategy 2022-2026.
There is a clear momentum as the year draws to a close. We must carry it into 2023 for a final, concerted push. Success is in our hands.

Members of the Regional Subcommittee for Polio Eradication and Outbreaks in the Eastern Mediterranean reviewed recent progress during the 69th session of the Regional Committee. It was the sixth meeting of the subcommittee since it was formed during the 67th Regional Committee.
During the meeting Member States and partners reiterated their commitment to freeing current and future generations of children from polio and called for sustained efforts to end polio once and for all, including the pockets of wild poliovirus that linger in Afghanistan and Pakistan.
Visit the EMRO website for the full story.
This two-year old outbreak of circulating vaccine-derived poliovirus (cVDPV) type 2 began after the virus was imported from neighbouring Chad.
Click on the photo gallery to see what it took to close the outbreak.

© WHO/Sudan
Two technical assessment missions worked on scrutinizing available evidence and analyzing the absence of polioviruses across Sudan. The first mission, conducted virtually in October 2021, shared their recommendations with Sudan’s polio eradication team to ramp up their efforts across the country.
A second official outbreak response assessment team undertook the next phase of this detailed task. They visited Khartoum and six of Sudan’s 18 states as part of their work from 24 July to 1 August 2022.

© WHO/Sudan
Both review teams comprised experts from the World Health Organization (WHO) and the United Nations Children’s Fund (UNICEF). Their skills and experience ranged from global public health, epidemiology and biostatistics to surveillance, vaccine management and communication.
They worked hand in hand with the Federal Ministry of Health of Sudan, with state-level ministry staff and with health workers at ground level.

© WHO/Sudan
After a close review of the functionality and sensitivity of the country’s surveillance system, the assessment team noted that Sudan’s acute flaccid paralysis (AFP) surveillance indicators are indeed meeting the necessary standards. The gold standard for polio surveillance is through searching for AFP in children, and testing stool samples to confirm the presence of the virus.
All poliovirus samples collected since 18 December 2020, the date of onset of paralysis of the last child affected in the outbreak, were processed like clockwork in Sudan’s laboratory. They were reported as poliovirus negative and recorded.

© WHO/Sudan
The missions noted Sudan’s 14 environmental surveillance sites are also collecting and testing waste water samples regularly, in line with international protocol.
During the polio outbreak, 14 sewage samples in the country’s bustling capital, Khartoum, tested positive for cVDPV2, indicating circulation there.

© WHO/Sudan
As part of their work, the technical mission also reviewed the core functions of Sudan’s laboratories and the country’s preparation mechanisms for poliovirus events or outbreaks. This also included data on population immunity, childhood immunization and vaccine management protocol.

© WHO/Sudan
A large part of Sudan’s success can be attributed to its swift response to the outbreak as soon as it was confirmed.
The country conducted two high-quality nationwide campaigns in all 18 states to curb virus spread in November 2020 and January 2021. Each campaign delivered monovalent oral polio vaccine type 2 (mOPV2) to over 8 million under-fives.

© WHO/Sudan
Weighing in on this milestone, senior experts in WHO’s polio eradication programme, including
Dr Hamid Jafari, WHO Director for Polio Eradication in the Eastern Mediterranean Region, and Dr Ni’ma Saeed Abid, WHO Representative to Sudan, lauded public health officials and immunization health workers on the ground for their swift response to the outbreak.
They reiterated the importance of maintaining sensitive AFP surveillance, ensuring better outbreak preparedness and response, enhancing coverage of essential immunization, and strengthening cross-border coordination. This is crucial given Sudan remains at high risk of importation of polioviruses.

© WHO/Sudan
Following this extensive work, the outbreak response assessment team concluded that the spread of cVDPV2 has indeed stopped, and that the outbreak is over.
The Global Polio Eradication Initiative (GPEI) has been informed of a case of paralytic polio in an unvaccinated individual in Rockland County, New York, United States.
The US Centers for Disease Control and Prevention (CDC) are coordinating with New York State health authorities on their investigation. Initial sequencing confirmed by CDC indicates that the case is type 2 VDPV.
Following the detection, the Global Polio Laboratory Network (GPLN) has confirmed that the VDPV2 isolated from the case is genetically linked to two Sabin-like type 2 (SL2) isolates, collected from environmental samples in early June in both New York and greater Jerusalem, Israel, as well as to the recently-detected VDPV2 from environmental samples in London, UK. Further investigations – both genetic and epidemiological – are ongoing to determine possible spread of the virus and potential risk associated with these various isolates detected from different locations around the world.
It is vital that all countries, in particular those with a high volume of travel and contact with polio-affected countries and areas, strengthen surveillance in order to rapidly detect any new virus importation and to facilitate a rapid response. Countries, territories, and areas should also maintain uniformly high routine immunization coverage at the district level and at the lowest administrative level to protect children from polio and to minimize the consequences of any new virus being introduced.
Any form of poliovirus anywhere is a threat to children everywhere. It is critical that the GPEI Polio Eradication Strategy 2022-2026 is fully resourced and fully implemented everywhere, to ensure a world free of all forms of poliovirus can be achieved.
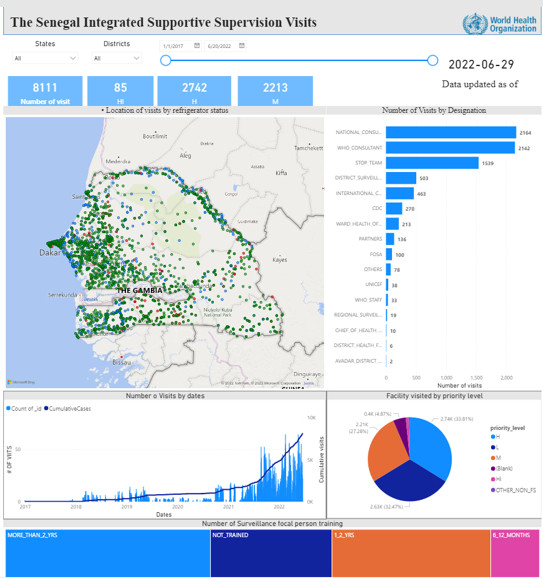
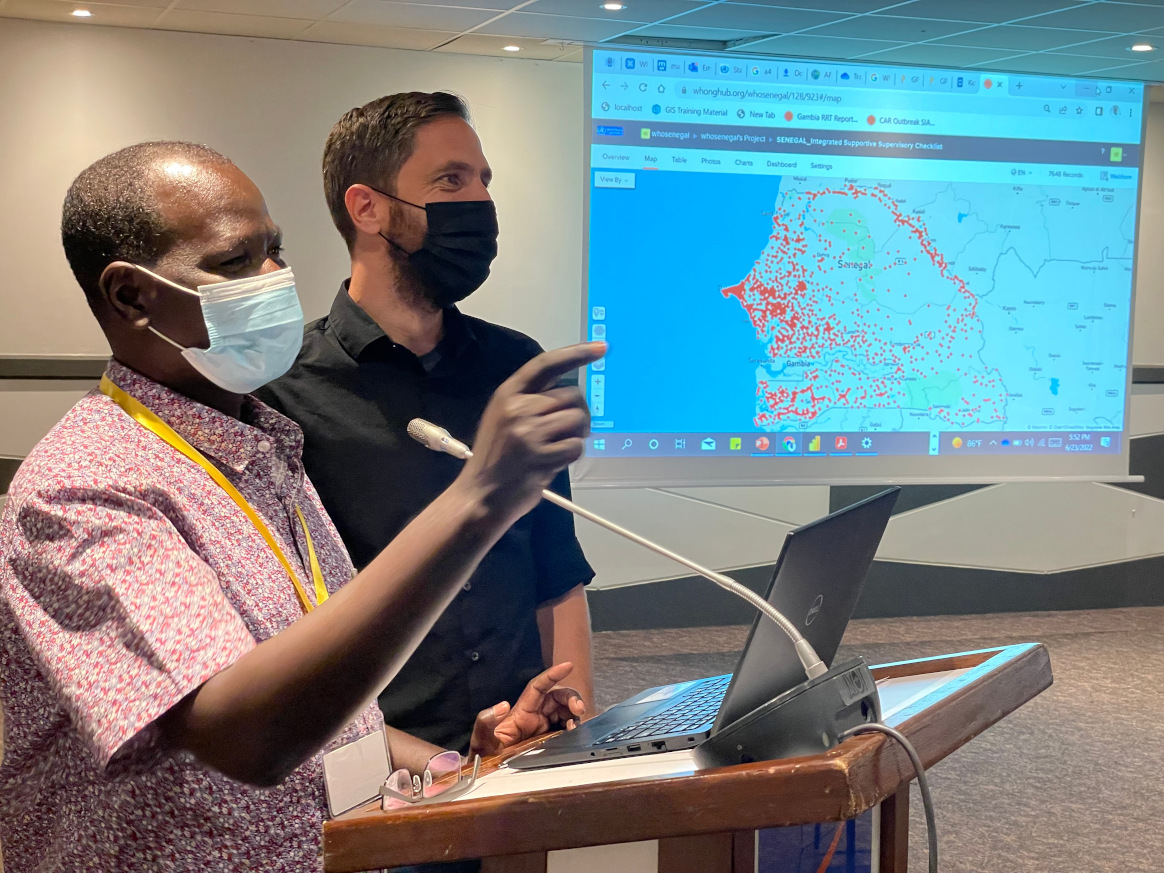
While the WHO Africa Region (AFRO) has been facing its last hurdle in eradicating polio of all types since being certified indigenous wild polio free in 2020, a circulating variant of polio virus type two has been present in 26 countries with more than 1,000 cases between them, coupled with the recent importation of two wild polio type 1 cases. To help reverse this trend, the WHO/AFRO Geographic Information Systems (GIS) Center is equipping over 200 key country office focal points and Ministry of Health personnel across 47 countries with essential innovative technologies to better address outbreaks with necessary speed and quality.
Concluding a series of one-week capacity-building workshops over the past six months and targeting of the WHO regions of Central, East & Southern, and West Africa – – the AFRO GIS Center, with the support of the Bill & Melinda Gates Foundation (BMGF), WHO HQ Polio Unit and GIS Centre for Health, the United States Centers for Disease Control and Prevention (CDC), and Novel-t on-boarded digital GIS and Mobile Health (mHealth) technologies to support regional and national agendas particularly on planning and analysis for improvement of surveillance, campaigns and outbreak response for polio and all other routine immunization and outbreaks. While the initial investment was made by polio these tools are being leveraged for all health interventions.
“These are solutions to advance national and regional agendas even beyond polio” stated Kebba Touray, Technical Manager – AFRO GIS Centre, “the COVID-19 pandemic response was able to advance using the AFRO polio GIS Centre’s technical support with the development of real-time data collection, analysis and monitoring tools and generated several products including dashboards (providing easy availability and visualization of information), which facilitated rapid decision making for response activities across the region.”
The GIS Capacity Building training transferred knowledge to key country office focal points and Ministry of Health personnel across Africa on innovations to better enable countries to:
- Design country-level specific static and dynamic maps – using platforms such as Microsoft Power BI, and ArcGIS – for the outbreak response and provide real time analysis through the dashboards.
- Provide country specific information visualization (using Dashboards) to publish in the existing AFR-mHealth workspace at AFRO and in their respective public health systems.
- Develop data collection, data validation and monitoring mechanisms that provides increased accuracy on immunization information and populations through the Open Data Kit (ODK) platform to enhance mobile data collection.
- Use AFRO GIS and information visualization innovative solutions at country level to receive real-time information on active surveillance visits conducted at health facility level, environmental surveillance site performance, rapid population estimates data, vaccination team movement during polio campaigns, among others.
“I am particularly eager to take back the new capacity I have on ODK and PowerBI when monitoring our entire Expanded Programme on Immunization (EPI) interventions” stated participant Dexter Merchant, Assistant Director for Monitoring and Evaluation at the Ministry of Health in Liberia, “using ODK as the process to collect data on where we have essential services and where we don’t is going to make things move a lot faster and more efficiently in identifying gap, I am confident these tools will now be integrated in Liberia”.
To ensure sustainability, country accountability and ownership, in-country GIS working groups which will constitute personnel from WHO and Ministries of Health will be established to continue efforts of knowledge transfer and capacity building principally amongst data managers, GIS analysts, and surveillance officers.
In closing, the WHO Representative in Senegal, Dr. Lucile Imboua and host of the last training series emphasized the “need to ensure harmonization of all the GIS tools and to be flexible to accommodate the use of other tools across different programs.”
The underlining consensus from all WHO, government and partner participants is that in order to end polio and strengthen health systems, the region heavily relies on the innovative technologies of GIS in executing health responses. The use of GIS innovations with precision in accuracy, transparency, accountability and ease of application and sustainability provides a huge opportunity to reach every last child across the 47 countries, eradicate polio from the region, and serve public health for all.

At his office in Sana’a, Yemen, Dr Mutahar Ahmed stands before a wall-sized map of his country and feels the weight of the world on his shoulders.
“The situation here in Yemen is very complex, and the problems we face are quite immense,” said Dr Ahmed.
As Yemen’s national surveillance coordinator, Dr Ahmed leads the country’s acute flaccid paralysis (AFP) surveillance efforts, the primary means of tracking poliovirus transmission. With an explosive outbreak of circulating vaccine-derived poliovirus type 2 having paralysed 115 children and counting, and with swathes of the country’s infrastructure – from roads to hospitals – decimated by conflict, you’d be forgiven for thinking that his and his team’s efforts to surveil for poliovirus were falling short or otherwise compromised. But you’d be wrong.
In Yemen, despite a long-running conflict and complex humanitarian disaster that has significantly impacted health care, AFP surveillance indicators tell a promising story of a functioning system where case detection, sample collection and laboratory analysis – the steps that enable us to detect poliovirus so we can respond to it – are, in fact, on track.
Surveillance data allows the polio programme to identify new AFP cases and to test those cases to determine whether polio infection is the cause. In this way, a robust and wide-reaching AFP surveillance system enables health workers to detect the presence and circulation of poliovirus.

“In addition to our work building the engagement and knowledge of pediatricians and clinicians, we are reaching the community and community-based health care providers including traditional healers. We also appeal to families for their support in reporting cases. The more aware they are of the symptoms of paralysis in a child, the quicker our surveillance coordinators can collect the stool sample for analysis,” said Dr Ahmed.
Early detection of symptoms such as AFP is a crucial step in the chain of polio surveillance. If a case of paralysis is not reported within the first 14 days of the onset of symptoms, the reliability of testing the sample in the lab reduces significantly. In Yemen, the AFP surveillance system in high-risk districts is supported by volunteers trained in community-based surveillance. In 2021, 82% of AFP cases were detected early, within the first seven days of the onset of paralysis, which is above the global target of 80%.
Once a case is detected and stool samples are collected, it’s vital to make sure the samples reach the laboratory in good condition.
“Two stool samples are required from each child showing symptoms of paralysis. Both samples need to be collected within the first 14 days, 24 hours apart. They need to be correctly labelled, and their temperature needs to be maintained at between 2 and 8 degrees. Otherwise, they are not adequate samples,” said Dr Ahmed.
In 2021, 921 AFP cases were detected. Of these cases, 87.84% had adequate specimens collected, which is above the global target of 80%.
Along with stool adequacy, another key performance indicator for surveillance is the non-polio AFP rate. This refers to the detection of diseases, other than polio, that can cause AFP. Yemen’s non-polio AFP rate is 5.96 per 100,000 children aged below 15 years in 2021, significantly higher than the global standard of three per 100,000 for polio outbreak countries like Yemen. This accomplishment points to the sensitivity of Yemen’s surveillance system due to the relentless efforts and commitment of the surveillance personnel working with Dr Ahmed.

Due to electricity shortages, maintaining the cold chain (keeping vaccines cold) and reverse cold chain (keeping stool samples cold) poses a significant challenge for the programme. To overcome this and further increase the efficiency and sensitivity of the surveillance system to detect polioviruses as quickly as possible, solar power panels have been installed in health facilities at the central and governorate levels to support the storage and transfer of stool samples. One indicator of the impact of this change is Yemen’s non-polio enterovirus rate, which tells us what percent of stool samples tested negative for poliovirus, but were in such condition that they could still test positive for enteroviruses. In 2021, that rate was 20 percent above the global target of 10 percent.
Because Yemen does not have a poliovirus laboratory in-country for testing, samples are first collected at the central level in Sana’a and then sent by road to Muscat, Oman. The journey can take up to seven days, barring any obstacles or emergencies.
“Working in this role is a challenge, but what I particularly enjoy is how we are able to turn these challenges into opportunities for the AFP surveillance programme. The AFP indicators for the last year show us how far we have come in our journey,” said Dr Ahmed.
He explained why these indicators are so critical to the polio programme.
“The fact that our indicators are above the minimum global standards shows that the surveillance system is functioning, sensitive and responsive, despite the critical humanitarian situation. The data from our surveillance work has helped us identify the outbreak of circulating vaccine-derived polioviruses type-1 and type-2. The situation is quite fragile, but we are committed to addressing these challenges, and we will continue to do so.”
WHO has supported Yemen to establish an environmental surveillance system to supplement its AFP surveillance system and support early detection of polioviruses and more timely responses.

Following wide engagement of stakeholders – from lab workers to engineers to certification bodies responsible for signing off on the lockdown of poliovirus strains after certification of eradication – WHO’s chief guidance document for poliovirus containment has been given an overhaul. The update to the WHO Global Action Plan for Poliovirus Containment (GAP-IV, previously GAP-III) comes at the request of the WHO Containment Advisory Group (CAG) and streamlines the tool with other relevant WHO guidance and technical recommendations made by CAG. Its availability is expected to help accelerate containment implementation worldwide.
Containment involves biosafety and biosecurity requirements for laboratories and vaccine production sites, or any other place handling and storing eradicated polioviruses, to minimize the risk of these pathogens being released into communities. It also concerns risk mitigation measures associated with field use of some live oral polio vaccines. WHO urges facilities holding virus to move through its Containment Certification Scheme, and follow guidance contained in GAP-IV.
“Retention of poliovirus materials for what their governments deem to be critical functions is a risk and responsibility for all countries that choose to do so,” said Prof David Heymann, Chair of the CAG and professor of infectious disease epidemiology at the London School of Hygiene and Tropical Medicine. “GAP provides guidance that aims to minimize the risk of escape of the poliovirus from a retention facility, and we hope that the revised publication ̶ which stakeholders in polio eradication helped shape ̶ will ensure faster action by countries that decide to retain poliovirus materials,” he said.
“The revision of the guidance has been a long time in the making and comes with a lot of anticipation,” stated Dr Harpal Singh, WHO polio technical officer and CAG secretariat. “WHO and CAG have taken on board the numerous concerns and feedback from Member States with regards to carrying out the guidance, and a certain degree of flexibility based on local risk mitigation measures has been applied in some areas, whilst maintaining the rigor of evidence-based best practice,” he added. “We anticipate that this will result in a better implementation of the requirements for Member States opting to retain [poliovirus] materials, and having their facilities certified,” he added.
To date, two of three strains of wild poliovirus have been declared globally eradicated – type 2 and type 3. Countries around the world, however, continue to handle and store these viruses for functions including polio vaccine manufacture, diagnostics and research, among others. It is essential that any facility holding poliovirus types 2 and/or wild or VDPV type 3 stocks, regardless of purpose, either put in place the necessary biorisk management measures outlined in GAP or destroy their virus stocks.
“The world is on the precipice of eradication of wild poliovirus type 1 with the lowest ever case count recorded in 2021, and we got rid of WPV2 and WPV3 in 2015 and 2019, respectively. While some progress has been made, we’re actually quite behind schedule in ensuring those two eradicated serotypes are properly contained, and more needs to be done in this regard,” said Aidan O’Leary, head of WHO’s polio eradication programme.
“Importantly, Member States all committed to accelerating poliovirus containment action in 2018 through a World Health Assembly Resolution,” he reminded. “WHO will continue to work with and encourage Member States to move on their targets, and reprioritize these actions. Failure to do so not only heightens but prolongs the risk of the reintroduction of virus, the effects of which could be devastating,” he added.
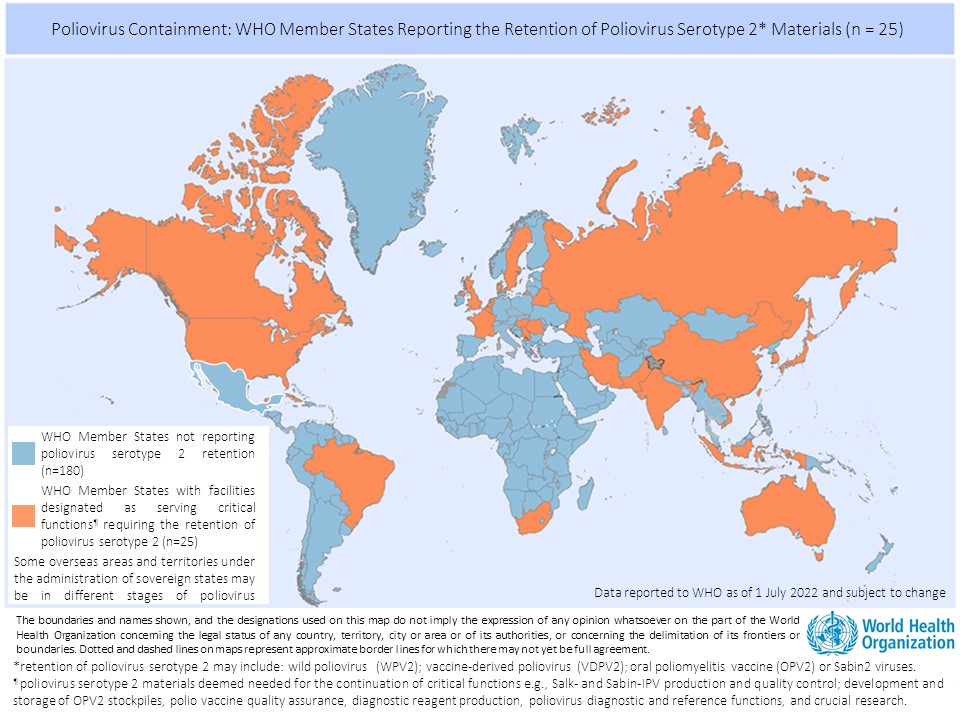
There are currently 25 countries hosting 65 facilities officially designated by their respective governments to retain poliovirus materials. The majority of countries have established a National Authority for Containment for domestic oversight over containment action, in line with commitments from the 2018 resolution, and work is underway to progress their facilities through the Containment Certification Scheme.
For now, containment measures apply to all type 2 and wild and vaccine-derived type 3 materials.
Leaders at this week’s G7 Head of State meeting in Germany and last week’s Commonwealth Heads of Government meeting in Rwanda renewed global commitment to polio eradication. In their official Communiqué, the Leaders of the Group of Seven (G7) vowed to ‘continue our support for polio eradication through the Global Polio Eradication Initiative’, while the Commonwealth Heads of Government, in their joint Communiqué on ‘Delivering a Common Future’, urged the continued intensified effort to eradicate polio, even amid other pressing health and development issues. These calls and commitments follow similar engagements made at previous global political fora this year, notably the recently-held G7 Development and Health Ministers meeting, and the World Health Assembly.
Global partners of the eradication effort, notably led by Rotary International and Rotarians around the world, are working with the public sector to ensure political commitments are fully operationalized.
In April 2022, GPEI partners, led by WHO Director-General, launched the ‘Investment Case for Polio Eradication’, the sister document to the Polio Eradication Strategy 2022-2026, which lays out the economic and humanitarian rationale for investing in a polio-free world, as well as the broader benefits of polio eradication.
In October 2022, Germany will generously co-host a global pledging moment, giving the international development community and polio-affected countries the opportunity to publicly re-commit to this effort, including to support a stronger and sustainably-funded WHO, so that the organization can maintain its capacity to support countries in achieving and sustaining polio eradication, and continue to benefit broader public health efforts, including support for pandemic preparedness and response.
The Global Polio Laboratory Network (GPLN) has confirmed the isolation of type 2 vaccine-derived poliovirus (VDPV2) from environmental samples in London, United Kingdom (UK), which were detected as part of ongoing disease surveillance. It is important to note that the virus has been isolated from environmental samples only – no associated cases of paralysis have been detected. Recent coverage for the primary course of DTaP/IPV/Hib/HepB vaccination, which protects against several diseases including polio, in London suggests immunization coverage of 86.6%.
Initially, vaccine-like type 2 poliovirus (SL2) had been isolated from samples taken from the same site between February and May 2022. Genetic analysis suggests that the new VDPV2 and previous SL2 isolates have a common origin, still to be identified, but the technical definition and criteria for ‘circulation’ of VDPV2 are not met at this time. Additional sewage samples collected upstream from the main waste-water treatment plant’s inlet are being analysed.
Investigations and response by the UK Health Security Agency are ongoing to:
- assess both origin and risk of circulation associated with these isolates;
- strengthen poliovirus surveillance including enterovirus and environmental;
- explore routine immunization catch-up of children who are under-immunized, including of families that have recently arrived in the UK from countries with recent use of type 2-containing oral polio vaccine; and,
- enhance communications about this incident to health professionals and caregivers.
It is important that all countries, in particular those with a high volume of travel and contact with polio-affected countries and areas, strengthen surveillance in order to rapidly detect any new virus importation and to facilitate a rapid response. Countries, territories, and areas should also maintain uniformly high routine immunization coverage at the district level and at the lowest administrative level to protect children from polio and to minimize the consequences of any new virus being introduced.
Any form of poliovirus anywhere is a threat to children everywhere. It is critical that the GPEI Polio Eradication Strategy 2022-2026 is fully resourced and fully implemented everywhere, to ensure a world free of all forms of poliovirus can be attained.

It’s been a long day for Dr. Nabeel Abdu Omar Ali. Since early morning, he has been going from one house to the next in a community in Aden, Yemen – listening to the concerns of parents and speaking to them about the importance of vaccination to save their children from polio. And he plans to continue till the sun goes down.
“The weather is pleasant now and I want to meet as many parents as possible, especially those who have concerns about vaccines. In a month’s time, the heat and humidity will be unbearable, making it difficult to walk from house to house,” says Dr. Nabeel.
Nicknamed “the mobile imam” by his peers, Dr. Nabeel is a pediatrician by profession, and a certified imam (Islamic teacher) from the Ministry of Endowment in Southern Yemen. He uses his religious knowledge and medical facts to educate the public about the importance of vaccination in protecting children from polio and other deadly diseases.
A few weeks back, he visited several families who were refusing vaccines in a nearby neighborhood. In addition to speaking to them about the safety and benefits of the polio vaccine, the ‘mobile Imam’ administered polio drops to his grandchildren in front of everyone at the community meeting.
“When the people saw a doctor and Imam like me vaccinating my own grandchildren, I think it was easier for them to believe that the vaccine was safe for their children too,” says Dr. Nabeel with a smile.
Reaching out to other Imams for support
Dr. Nabeel frequently reaches out to other Imams, training them about the benefits of vaccination and encourages them to share with the public during their Friday sermons.

“Imams are very influential in our communities – to raise awareness, shape social values, and promote positive attitudes, behaviours and practices. For example, a single sermon is powerful enough to change misconceptions about vaccines in some communities. If Imams are fully equipped with accurate information, it goes a long way in build trust and creating vaccine acceptance among the people – helping children in the community to stay health and free from polio and other vaccine-preventable diseases,” he adds.
The ongoing conflict in Yemen has severely damaged the health and basic infrastructure. There are frequent interruptions in power supply, and this often creates suspicion among community members as well as Imams whether vaccines are being stored safely.
“I was training a group of imams and they shared their doubts about the safety of the vaccine. They were skeptical about how refrigerators could store polio vaccines safely when there are so many power cuts in the area.”
In response, Dr. Nabeel organized a tour for the group to a vaccine storage facility where they were able to see and learn about special refrigerators that are powered by solar energy when there are power cuts.
Promoting the benefits of vaccination for over a decade
Dr. Nabeel has been working for the immunization programme in Yemen for over 12 years, partnering with UNICEF for numerous polio vaccination campaigns and routine immunization services.
When he first started out as pediatrician, he met many children who were paralyzed by polio. He felt frustrated that so many children would have to suffer for the rest of their lives by a disease that could have been easily prevented by a vaccine. That is when he decided to dedicate his time to educate caregivers and parents on the benefits of vaccination.

“There are many misconceptions about vaccines. Throughout my career I have been confronted by people who were resistant to the idea of vaccination. Some people think that the vaccine will make them infertile, while others believe it’s some kind of a conspiracy. However, my many years of work in immunization and knowledge of religious scriptures has proven to be valuable so far in building trust in vaccine in communities,” says Dr. Nabeel.
The ‘mobile Imam’ is also quite adept in working with the media to promote vaccination. He is often seen and heard on TV and radio talk shows speaking about the benefits of vaccination and answering to questions from concerned parents and caregivers.
“I use a mixed approach to address vaccine hesitancy and dispel misinformation about vaccines. Sometimes it is helpful to talk about vaccines during Friday sermon, while other times, it is more effective to explain to a caller on a radio programme why vaccines are important,” he explains with a smile.

Over four days in the middle of May, parents in the governorates of Bethlehem and Jerusalem were urged to take their children under age five to health facilities for a supplementary dose of oral polio vaccine. The aim: boost immunity to poliovirus in the face of increased regional risk.
Unlike most polio campaigns in the Eastern Mediterranean Region, the mechanism for the campaign in occupied Palestinian territory (oPt) was via health facilities, rather than house to house. This can be a major ask for parents, who must organize time and transport to get children to health facilities during a relatively brief window.
Round 1, from Monday 16 May through Thursday 19 May, tested the resolve of a community that is famously pro-vaccine (routine immunization coverage across oPt is typically between 98% and 100%), but like parents everywhere, juggling work, childcare and other commitments.
While most often, mothers took their children for vaccination, in many of the health facilities where vaccination took place, grandmothers were seen supporting mothers or even stepping into their shoes.
“I brought my granddaughters today to take the polio vaccine because their mother is studying in university and their father is working,” said Abeer Nasrallah, who brought Zeina (two) and Mariam (three) to El-Azariyeh, a Palestinian Ministry of Health clinic in Jerusalem governorate.

In Biddo, an area of Jerusalem governorate where the main UNRWA clinic serves both local families and those from more remote regions, a steady stream of clinic visitors climbed out of mini-buses and taxis after lengthy journeys.
“Many Bedouins come to us from remote areas like Bani Samuel and Beit Iksa, although the transportation from their areas is very hard for two reasons. First, the roads are very difficult, and second, there are a lot of checkpoints that could keep you waiting for hours,” said Tamam Taha, a nurse at the Biddo UNRWA health facility.
“We have good numbers of people coming to the clinic, both refugee and non-refugees, and we give the vaccine to all of them,” she said.
One of the groups she served was headed by Samar Al-Sheikh, a mother of one who arrived with three girls in tow.
“I brought my brother’s daughters because he can’t come. Usually, I would walk from my home, but I took public transportation today because I have three kids with me. It was hard to manage them, but it’s important to give them the vaccine,” she said.
In some cases, the hurdles parents faced to bring their children to health facilities were starkly visible.
Nidal Kandeel, father of Janette (three) and Jolan (21 months), arrived at Biddo UNRWA health facility on crutches.
“I got an injury in my work a year ago, and I’m now disabled for the rest of my life. It was hard for me to come to the clinic using public transportation, but I know how important it is for my children to take the polio vaccine, and this is why I am here,” he said.

While the results of this preventative campaign are still pending, clinics promoted the campaign heavily through their own social media groups, and health workers explained that logistics aside, it wasn’t difficult to convince Palestinian parents of the need to vaccinate under-fives.
“There is a lot of demand for this vaccine. Many people have been coming since this morning to get their children to take the vaccine. In the last hour, we have vaccinated more than 100 children,” said Khawla Abu Khdeir a nurse running the registration desk at El-Azariyeh.
Following the four-day vaccination blitz at health facilities, nursing teams will review registers of children vaccinated and cross-reference these with patient lists. Parents of children who weren’t vaccinated will be telephoned and efforts made to reach those children through in-clinic follow-up or outreach.
Round two of the bivalent oral polio vaccine (bOPV) campaign is expected in mid to late June, with the aim of raising immunity levels in these two governorates.
Palestine has been polio-free for more than 25 years, thanks to a robust routine immunization programme and a strong culture of vaccine acceptance.

But following the detection of circulating vaccine-derived poliovirus type 3 (cVDPV3) in sewage outflow in Wadi Alnar site, a junction between wastewater coming from inside the green line with wastewater coming from Bethlehem and Jerusalem, the Palestinian Ministry of Health launched efforts to boost immunity in the areas deemed most at risk.
The campaign was carried out with support from WHO, UNICEF and UNRWA’s Palestine country offices.
WHO’s Palestine office provided technical support to the Ministry in planning and executing this campaign, drawing on the extensive expertise of our regional polio eradication programme.
The vaccination campaign in Palestine is part of the global effort to eradicate poliovirus, spearheaded by the Global Polio Eradication Initiative.
In this two-part video series, we chat with Dr Ananda Bandyopadhyay, Deputy Director of Polio Technology, Research & Analytics, BMGF, about the new tool in GPEI’s kit to combat cVDPV2: novel oral polio vaccine type 2 (nOPV2).
As a result of ongoing disease surveillance, the Global Polio Laboratory Network (GPLN) has confirmed that a child in Changara district, Tête province, Mozambique, was paralyzed by type 1 wild poliovirus (WPV1).
The child experienced onset of paralysis on 25 March 2022, and sequencing of the virus confirms that it is linked to the imported WPV1 case confirmed in Malawi in February.
While this detection of another WPV1 in the southeast Africa region is a concern, it is not unexpected following the Malawi detection in February and further underscores the importance for all countries to prioritize immunization of children against polio.
Mozambique has participated in the multi-country coordinated vaccination campaigns in response to Malawi’s imported WPV1, with two vaccination rounds already conducted. The most recent took place at end of April, with 4.2 million children vaccinated across the country, and the Global Polio Eradication Initiative (GPEI) is supporting countries to strengthen disease surveillance and prepare for the remaining two campaign rounds. These will cover Malawi, Tanzania, Mozambique and Zambia, with Zimbabwe joining the later rounds to ultimately help reach over 23 million children under five years with polio vaccine by end of August 2022.
Mozambique last recorded a case of wild polio in 1992 though the country has more recently been affected by an outbreak of circulating vaccine-derived poliovirus type 2 (cVDPV2). Three cases have been detected since April 2021 and vaccination campaigns in response to the outbreak are continuing, which include use of the novel oral polio vaccine type 2 (nOPV2).
Wild polio remains endemic in just two countries – Pakistan and Afghanistan. The WPV1 detection in Mozambique does not affect the WHO African Region’s wild poliovirus-free certification status officially marked in August 2020, as the virus strain originated in Pakistan. However, any child paralysed by polio is one too many. The polio eradication programme has seen importations from endemic countries to regions that have been certified wild poliovirus-free in the past and has moved quickly to successfully stop transmission of the virus in these areas.
Polio anywhere is a threat to children everywhere. It is vital that all parties ensure that the GPEI has the support it needs to implement its five-year eradication Strategy in full and ensure no child is paralysed by polio ever again.

On Monday 16 May, the Palestinian Ministry of Health will launch round one of a polio vaccination campaign targeting all children under age five in Bethlehem and Jerusalem.
The vaccination campaign is scheduled to run over three days: Monday 16 May through Wednesday 18 May 2022. Vaccination, using bivalent oral polio vaccine (bOPV), is free and will be offered at maternal and child centres and UNRWA centres throughout Bethlehem and Jerusalem.
Palestine has been polio-free for more than 25 years, thanks to a robust routine immunization programme and a strong culture of vaccine acceptance. But following the detection of circulating vaccine-derived poliovirus type 3 (cVDPV3) in sewage outflow in Wadi Alnar site, where there is a junction between wastewater coming from inside the green line with wastewater coming from Bethlehem and Jerusalem, the Ministry of Health has taken the decision to launch a preventative vaccination campaign to boost children’s immunity in the two areas deemed most at risk: Bethlehem and Jerusalem.
“It is all of our duty to keep Palestine polio-free by making sure that our children under the age of five receive the polio vaccine every time it is offered. I encourage every parent to make it a priority to vaccinate their children – for their sake, and for Palestine,” said Dr Mai al-Kaila, Minister of Health, Palestine.
The vaccination campaign is being carried out with support from WHO, UNICEF and UNRWA’s Palestine country offices.
“WHO’s Palestine office has provided technical support to the Ministry in planning and executing this campaign, drawing on the extensive expertise of our regional polio eradication programme. Palestine is in a strong position thanks to its routine immunization programme and to the value Palestinian parents put on childhood immunizations, but the regional risk of polio is increasing and it is absolutely crucial that we reach and vaccinate every child under age five in the target areas,” said WHO occupied Palestinian territory Representative Dr Rik Peeperkorn.
“It is critical that every child can access their right to a life free from polio and other vaccine-preventable diseases. UNICEF and its partners in this campaign are making every effort to ensure no child in Palestine will be affected by this debilitating disease. It is a duty upon all of us to keep Palestine polio free,” said UNICEF’s Special Representative to the State of Palestine Lucia Elmi.
Round two of the campaign will take place in June and will offer all children under age five a second two drops of polio vaccine, further boosting their immunity. Children living outside of Jerusalem and Bethlehem do not currently require an additional dose of oral polio vaccine. If their routine immunizations are up to date, they are well protected from poliovirus and other vaccine-preventable diseases.
Poliovirus primarily affects children under age five and can lead to lifelong paralysis. It can easily be prevented through vaccination. Parents are urged to accept polio vaccines every time they are offered.
The vaccination campaign in Palestine is part of the global effort to eradicate poliovirus, spearheaded by the Global Polio Eradication Initiative.
It is a hot afternoon in Chagai, a small community on the south bank of the River Gambia when the polio vaccination team arrives to a rapturous welcome. Children and women jump to their feet, some waving and swinging their hands as they pound their feet on the ground in near perfect sync with the beat of the drum.
This excitement is caused by one certain member of the vaccination team wearing a bush hat and playing the drums. Lamin Keita, 60, is a cultural musician supporting the vaccination team in raising awareness about polio and encouraging parents to vaccinate their children. Lamin, popularly called Takatiti, because of one of his songs, is immediately surrounded by excited children, as he adjusts his beats to respond to the ecstasy and rigor of the dancers.
“When I arrive on the back of a pick-up truck with my megaphone and drums, children from the communities run after us in full excitement and jump up and down and ask me to play my drums,” Takatiti explains.

This is what Takatiti is popular for – pulling crowds with his drums to communicate important messages like polio vaccination. For almost four decades, he has toured communities in the region, accompanying health workers as they seek to persuade parents and caregivers to vaccinate their children during mass vaccination campaigns like the polio campaign.
Local voices are the most powerful voices
Building trust in vaccines among parents and caregivers is the first critical step towards achieving high immunization coverage to stop the spread of polio. UNICEF, as a leading partner of the Global Polio Eradication Initiative (GPEI) for social and behaviour change, supports the government in strengthening engagements with communities, as the voices of local leaders and influencers like Takatiti play a powerful role in helping allay fears and concerns of parents and caregivers about vaccines.
“I have been making town announcements since the mid-1980s. I am aware of polio and its terrible consequences. Families hear myths and rumours and get concerned about vaccines. As they already know and trust me, I try my best to give them accurate information and clear their doubts, so that they can vaccinate their children against polio and other dangerous diseases,” Takatiti says.
“It’s important to deliver messages that are supported by facts in an effective way”
Days before the start of a polio vaccination campaign and during the campaign itself, Takatiti walks up and down the streets of villages, playing his drums and using his megaphone to talk to communities about the dangers of polio, how vaccination is the only way to protect children, and that polio vaccines are safe and free.

“I always try to promote peace and healthy life for all. It’s important to deliver messages that are supported by facts in an effective way. The Government and UNICEF provided me correct information and facts about polio and vaccines, so I am happy to volunteer for the campaign.”
A country mobilizes to stop polio
“If people trust health workers to cure other diseases, then it makes sense to trust the same health workers to protect our children from polio. Health workers even give the polio vaccine to their own children – so we should not doubt their good intentions. It is my job to let people know this truth, without offending them, and encourage them to vaccinate their kids,” Takatiti said.
In August 2021, The Gambia declared a national public health emergency in response to outbreaks of non-wild variants of polio in the country.

The Gambian government, with support from WHO, UNICEF, US Centres for Disease Control and Prevention (CDC)and GPEI partners, quickly responded and started preparing for nationwide immunization campaigns – managing supply and safe storage of vaccines, strengthening surveillance and monitoring, training health workers and vaccinators, and engaging with local leaders and influencers to build trust in vaccines.
The country undertook its first national polio vaccination campaign in November 2021 and followed up with a second round in March 2022.
Thanks to thousands of health workers, vaccinators, and community influencers like Takatiti, the vaccination campaigns have reached over 380,000 children aged five years and below in The Gambia.

Infectious diseases like poliomyelitis (polio) know no borders. Importation and subsequent spread of the virus led to the paralysis of 34 children, and 26 others tested positive without developing symptoms of paralysis. Extensive immunization efforts began in February 2021, and no child, adult or environmental sample in Tajikistan has tested positive since August 2021.
The outbreak in Tajikistan marked the first detection of circulating vaccine-derived poliovirus type 2 (cVDPV2) in the WHO European Region. It is now the first cVDPV2 outbreak in the world to be declared officially closed following supplemental immunization using the novel oral polio vaccine type 2 (nOPV2).
The Region has been free of endemic poliovirus since 2002. Detection of just 1 case of polio – whether from a wild or vaccine-derived poliovirus – is considered an outbreak, and requires an immediate and comprehensive response.
“Tajikistan’s success in stopping this outbreak is a major achievement and a clear demonstration of the highest level of political commitment of the Government of Tajikistan,” says Dr Hans Henri P. Kluge, WHO Regional Director for Europe.
“This outbreak and the subsequent response came at a time when the health system was already overstretched by the COVID-19 pandemic and the country was mounting a massive COVID-19 vaccination drive. Both outbreak responses had to be done without disrupting the vitally important provision of other routine vaccines to children. We acknowledge the efforts of the Ministry of Health over the past several years, which resulted in a resilient immunization system able to successfully manage all these competing immunization priorities.”
Actions taken to stop the outbreak
Following confirmation of the outbreak, the Ministry of Health and Social Protection of the Population took immediate steps, with support and guidance from WHO and other Global Polio Eradication Initiative partners. Actions included enhanced poliovirus surveillance, intensive contact tracing and a thorough review of immunization coverage at subnational levels. A rigorous risk assessment was conducted to determine the outbreak response scale and choice of vaccine, and the country rapidly completed a comprehensive verification process for readiness to use the nOPV2 vaccine.
In February 2021, a high-quality nationwide inactivated polio vaccine campaign was conducted to close the immunity gap against poliovirus type 2 among the more than half a million children born from 2016 to 2018 who had been left vulnerable as a result of global inactivated polio vaccine (IPV) supply constraints following cessation of trivalent oral polio vaccine use.
From June to September 2021, 2 nationwide and 1 subnational nOPV2 immunization rounds were implemented for all children under 6 years of age, with coverage confirmed (through external assessment) to be greater than 95%. Extensive social mobilization and communication strategies were deployed to reach groups who were at risk of being missed, including internal migrants in urban areas and unregistered children.
Assessment of the outbreak response
Several criteria must be met to officially close an outbreak, including at least 6 consecutive months in which no poliovirus is detected. The independent experts of the Global Polio Eradication Initiative who conducted the assessment in Tajikistan also looked at the performance of routine polio vaccination, the coverage achieved during the supplemental immunization rounds, and the capacity and sensitivity of the polio surveillance system to detect any poliovirus circulation.
Following the thorough assessment, which included briefings at the national level and field visits to national referral hospitals, public hospitals, polyclinics, regional and district immunization programme offices, and public health centres, the team recommended closure of the outbreak.
nOPV2 – a new chapter in global efforts to eradicate polio
Ending this outbreak using nOPV2 is an important milestone for the global polio programme. The innovative vaccine is a key part of the new strategy to stop cVDPV2s. Clinical trials show that nOPV2 is safe and effective, and more genetically stable than the traditional type 2 oral polio vaccine.
Since the rollout of nOPV2 began in March 2021, over 265 million doses have been administered across 14 countries. The majority of countries using the vaccine have also managed to stop transmission of cVDPV2; however, this is the first official closure of an outbreak to take place following nOPV2 use.
In addition to successfully halting transmission and lowering the risk of infection for millions of people, Tajikistan contributed to global research on nOPV2 with the support of WHO through an nOPV2 immunogenicity study. The country also participated in a global vaccine wastage study.

On 21 March, the Federal Government of Somalia, World Health Organization (WHO) and members of the Global Polio Eradication Initiative (GPEI) recommitted to stopping the ongoing outbreak of circulating poliovirus type 2 (cVDPV2) in Somalia at a three-day meeting convened in Nairobi, Kenya. High-level delegates at the meeting included HE Fawziya Abikar Nur, Federal Minister of Health and Human Services, Dr Mamunur Rahman Malik, WHO Representative to Somalia and Head of Mission, alongside senior representation from the Bill & Melinda Gates Foundation (BMGF), the Centers for Disease Control and Prevention (CDC), Rotary International, Save the Children, the United Nations Children’s Fund (UNICEF), and other UN agencies and partners.
Together, the Government, GPEI partners, which include WHO, UNICEF, the BMGF, CDC, Rotary International, GAVI, the Vaccine Alliance, and other key partners endorsed the Somalia Polio Eradication Action Plan 2022 to reaffirm their commitment.
The Somalia Polio Eradication Action Plan 2022 outlines a four-point call to action to stop the spread of the current outbreak, which is one of the longest lasting cVDPV2 outbreaks to be reported so far. The robust plan aims to direct partners’ efforts and resources towards boosting population immunity, making concerted efforts to reach high-risk populations — including inaccessible and nomadic communities and internally displaced persons — to strengthen their immunity, enhancing the search for poliovirus circulation, and strengthening coordination among all stakeholders. Some of the strategies that will be deployed include intensifying efforts to offer 5 opportunities for vaccination against polio in 2022, providing routine childhood immunization in high-risk locations, where children have missed out on vaccinations, and strengthening community engagement. Given how easy it is for the cVDPV2 virus to spill over international borders, the emergency plan also advocates for stronger cross-border coordination among the polio eradication programmes in Somalia, Kenya, Ethiopia and Djibouti.
“In the midst of the ongoing drought, and while recovering from the effects of the COVID-19 pandemic, our stakeholders must not forget how important it is to contain the ongoing poliovirus outbreak so that it does not spread any further and does not affect any more children’s lives,” said HE Fawziya Abikar Nur, Federal Minister of Health and Human Services. “On this occasion, I would like to extend my sincere gratitude to all our partners, and donors, for the immense efforts they have put into shielding millions of Somali children from polio over the years.”
“Since its inception 25 years ago, Somalia’s polio eradication programme has made progress, including by stopping outbreaks of wild poliovirus and, recently, one of circulating poliovirus type 3 in 2021. The programme has established a vast network of polio workforce and assets and we can do more not only to stop the current outbreak but to achieve broader health system goals through integration and effective use of our human and operational resources. Since 2018, Somalia has conducted several supplementary immunization campaigns. Despite these efforts, pockets of unvaccinated children remain, due to insecurity and limited access to health services,” said Dr Mamunur Rahman Malik, WHO Representative to Somalia.
The Somalia Polio Eradication Action Plan, which will be implemented in 2022, complements one of the goals outlined in the GPEI ‘Polio Eradication Strategy 2022–2026: Delivering on a Promise’, to stop cVDPV transmission and prevent outbreaks in non-endemic countries. It is also in line with Somalia’s national goals and UN Sustainable Development Goals (SDGs).
17 March 2022 — On Monday 7 March 2022, a case of circulating vaccine-derived poliovirus type 3 (cVDPV3) was confirmed in an unvaccinated girl aged three years and nine months in Israel. The girl had developed acute flaccid paralysis and upon testing of her stool, poliovirus was confirmed.
Further testing of the virus isolated from the girl revealed genetic links to VDPV3-strains detected in environmental samples collected between September 2021 and January 2022 from sites in Jerusalem and Bethlehem.
Circulating VDPV3 has also been confirmed in a sample taken from a contact in Jerusalem. This child does not display any symptoms of paralysis.
A previous statement published on 10 March 2022 had indicated circulation of this VDPV3 also in occupied Palestinian territory; further field investigations concluded that at this time, circulation can only be confirmed in Israel. This classification does not however change the risk this cVDPV3 presents to children in Israel and in the occupied Palestinian territory, nor the planned response activities.
Although there is currently no evidence of circulation of this cVDPV3 in occupied Palestinian territory, the proximity and interconnectedness of communities on both sides of the border and the volume and frequency of cross-border population movement underscore the risk to unvaccinated children in both places.
Local health authorities in both Israel and occupied Palestinian territory are conducting field, epidemiological and virological investigations, to determine more clearly the source and origin of the isolated virus and potential risk of further spread associated with it. Discussions are ongoing to plan an immunization response as appropriate (extent and scale to be determined, potentially to include a series of immunization outreaches with both inactivated polio vaccine and bivalent oral polio vaccine, both in high-risk areas of Israel and occupied Palestinian territory). At the same time, efforts are continuing to strengthen surveillance comprehensively in both Israel and occupied Palestinian territory.
Experts from headquarters, regional and country offices of the Global Polio Eradication Initiative (GPEI) partnership, which includes WHO, Rotary International (RI), the US Centers for Disease Control and Prevention (CDC), the United Nations Children’s Fund (UNICEF), Bill & Melinda Gates Foundation (BMGF) and Gavi, the Vaccine Alliance, are working together to help ensure an appropriate response and cessation of this outbreak.
Detection of this cVDPV3 underscores the importance of strong disease surveillance and high population immunity levels, in order to minimize the risk and consequences of any poliovirus introduction or emergence.
The GPEI partnership urges all health authorities to enhance surveillance for poliovirus and implement enhanced vaccination response to prevent further transmission, so that no child is at risk of lifelong paralysis from a disease that can so easily be prevented. GPEI is committed to assisting the health authorities in their efforts to stop the cVDPV3 outbreak.
Yemen is currently experiencing twin outbreaks of circulating vaccine-derived poliovirus type 1 and type 2 (cVDPV1 and cVDPV2). Both strains of poliovirus emerge in populations with low immunity and both can result in lifelong paralysis and even death.
Since 2019, 35 and 14 children have been paralysed by cVDPV1 and cVDPV2 respectively, three of the cVDPV2 cases confirmed in the past 10 days alone. The cVDPV2 outbreak, in particular, is ongoing and expanding and has already spread to other countries in WHO’s Eastern Mediterranean Region and UNICEF’s Middle East and North Africa Region. At its fourth meeting on 9 February 2022, the Eastern Mediterranean Ministerial Regional Subcommittee on Polio Eradication and Outbreaks issued a statement, expressing deep concern around these expanding outbreaks and requesting all authorities in Yemen to facilitate resumption of house-to-house vaccination campaigns in all areas.
The Global Polio Eradication Initiative (GPEI) partners strongly recommend high-coverage mass vaccination campaigns to stop a cVDPV outbreak. The vaccination response must achieve at least 90% of children vaccinated repeatedly with polio vaccine to protect them from polio and prevent seeding new vaccine-derived emergences. Therefore, the guidelines in the Polio Outbreak Response Standard Operating Procedures recommend that the vaccination response to polio outbreaks should be conducted using the house-to-house vaccine delivery strategy to maximize coverage of vulnerable children.
The GPEI urges the health authorities in Sana’a to conduct high quality house-to-house vaccination campaigns to stop the two concurrent outbreaks as soon as possible. If the current conditions in parts of Yemen do not permit house-to-house vaccination, then an intensified fixed-site vaccination campaign with appropriate social mobilization by the community and religious leaders trusted by the local communities should be implemented to maximize coverage among all vulnerable children.
Yemeni children face no shortage of threats: prolonged conflict, a devastated healthcare system, hunger and disease. But polio is one disease that can easily be prevented. Its circulation can be stopped in Yemen or anywhere else by vaccinating all children with oral polio vaccine.
The GPEI partners – WHO, Rotary International, the U.S. Centers for Disease Control and Prevention, UNICEF, the Bill & Melinda Gates Foundation and Gavi – are committed to providing support to all stakeholders in Yemen for responding to the polio outbreaks including in conducting polio vaccination campaigns that can reach all vulnerable children.
The Global Polio Eradication Initiative (GPEI) is extremely concerned about the unfolding effects of the current crisis in Ukraine on the country’s health system. A functioning health system must be kept neutral and protected from all political or security issues affecting countries, to ensure that people have continued access to critical and essential care.
At the same time, we have seen time and again that large-scale population movements, insecurity and hampered access contribute greatly to the emergence and/or spread of infectious diseases, such as polio.
Ukraine is currently affected by a circulating vaccine-derived poliovirus type 2 (cVDPV2) outbreak, with the most recent case detected in January 2022 (with disease onset in December 2021).
A national supplemental polio immunization campaign targeting nearly 140,000 children throughout Ukraine who had not been vaccinated against polio began on 1 February 2022, but is currently paused, as health authorities have shifted focus towards emergency services. Surveillance to detect and report new cases of polio is also disrupted, increasing the risk of undetected spread of the disease among vulnerable populations. The GPEI is working to urgently develop contingency plans to support Ukraine and prevent further spread of polio.
The GPEI has a long history of working in a variety of complex environments, and will continue to adapt its operations to the reality on the ground, to the degree possible, without compromising on the safety and security of health workers. At the same time, immunization and surveillance is being assessed in neighbouring countries, to minimize the risk and consequences of any potential infectious disease emergence/spread resulting from the current large-scale population movements. It is critical that necessary resources are mobilized and made available to assist with the humanitarian needs, including relief, disease response/prevention efforts both in Ukraine and in neighbouring countries.
Cairo, 10 February 2022 – The fourth meeting of the Regional Subcommittee on Polio Eradication and Outbreaks was convened on Wednesday 9 February, by WHO’s Regional Director for the Eastern Mediterranean Dr Ahmed Al-Mandhari. The meeting was attended by health ministers or their representatives from Djibouti, Egypt, the Islamic Republic of Iran, Pakistan, Qatar, Saudi Arabia, Sudan, United Arab Emirates and Yemen.
The Subcommittee declared the ongoing circulation of any strain of poliovirus in the Region to be a regional public health emergency and called on all authorities to enable uninterrupted access to the youngest and most vulnerable children through the resumption of house-to-house vaccination campaigns. It issued statements on wild poliovirus circulation in Afghanistan and Pakistan and on the circulation of vaccine-derived poliovirus strains in Yemen, where limits on house-to-house vaccination are preventing access to the most vulnerable children.
The spread of polio in the Eastern Mediterranean Region is a pressing emergency and it remains a Public Health Emergency of International Concern (PHEIC) under the International Health Regulations (IHR 2005).
Members noted a sharp decrease in cases of wild poliovirus in Afghanistan and Pakistan in 2021 but warned against complacency.
“Wild poliovirus transmission is at a historic low in the endemic countries of Afghanistan and Pakistan. The progress is remarkable, but it is fragile. The opportunity to end polio is knocking at our door, and we must seize it,” said Dr Al-Mandhari.
Speaking to the progress made in the last year, the Special Assistant to the Prime Minister on Health, Dr Faisal Sultan, assured members that the programme in Pakistan was leaving no stone unturned in the pursuit of zero polio transmission.
“We have intensified efforts in the hardest districts and core reservoirs and we are closely monitoring transmission across the border in coordination with Afghanistan, taking measures to respond to outbreaks if they occur and making every effort to ensure that the virus doesn’t spill over in either direction. To boost the confidence of marginalized communities, we are also providing essential services and vaccination of other antigens and diseases,” he said.
Outbreaks of circulating vaccine-derived polioviruses type 1 (cVDPV1) and type 2 (cVDPV2) continued to emerge and spread in the Region in 2021. As of February 2022, Afghanistan, Djibouti, Egypt, Pakistan, Somalia, Sudan and Yemen are responding to transmission of vaccine-derived polioviruses.
“The increasing outbreaks of circulating vaccine-derived poliovirus type 2 in the Eastern Mediterranean Region and neighbouring countries of Africa are deeply concerning and must be stopped rapidly. To do so, we need to ensure that we are creating an enabling environment for health workers to reach children with those two drops of polio vaccine,” said newly nominated co-chair H.E. Dr Hanan Mohamed Al Kuwari, Minister of Public Health of Qatar.
During the meeting, Djibouti’s Public Health Minister, Dr Ahmed Robleh Abdilleh, shared plans for vaccination campaigns and increased surveillance in response to the transmission of cVDPV2, recently detected through the newly launched environmental sampling programme.
Reflecting on the work of the Subcommittee, co-chair and Minister of Health and Prevention of the United Arab Emirates H.E. Abdul Rahman Mohammed Al Owais urged members to sustain the commitment seen in in 2021.
“We have together advocated for an increase in domestic funds, we have driven collaborative public health action in our own countries, and collectively pushed for a regional response to address the regional public health emergency of the poliovirus. But these things alone will not end transmission,” he said.
Dr Al-Mandhari expressed appreciation for Egypt’s role as the first country in the Region to roll out a nationwide vaccination campaign using the novel poliovirus vaccine, and Chris Elias, Chair of the Polio Oversight Board, praised the remarkable progress made in polio eradication in Pakistan with support of the United Arab Emirate’s Pakistan Assistance Programme.
“This regional solidarity and commitment we have seen, through this Subcommittee, is something I am proud of. It is this commitment to the end goal that will help push us over the last mile,” said Dr Hamid Jafari, director of the regional polio programme and co-facilitator of the Regional Subcommittee.
Dr Pascal Mkanda, Director for the Polio Eradication Programme in the World Health Organization’s Regional Office for Africa (AFRO), also famously known as our ‘villager in polio’, is this month (February 2022) entering a well-deserved retirement. Pascal’s contribution over the years to polio eradication in Africa, and indeed broader immunization, is second to none.
Under Pascal’s stewardship and leadership, wild polioviruses were successfully eradicated from the continent, the polio infrastructure integrated into broader public health efforts, new technologies and innovations for reaching the most marginalized children established and new vaccines successfully rolled-out. His expertise, knowledge, dedication, zeal, and passion to work and more importantly his mentorship to fellow colleagues and health workers to alleviate the lives of vulnerable children across the continent, will be sorely missed.

“I have worked with Pascal for close to 7 years, and during that time, I have witnessed first-hand Pascal’s dedication, and what he often refers to as ‘tough’ decision making, which we owe to the successes we have seen in the polio program” said Dr Matshidiso Moeti, WHO Regional Director for Africa.” My first interaction with Pascal was during the first meeting for Program Managers in the region, in Johannesburg, South Africa, in 2016. During this meeting Pascal expressed very passionately that the only way we can get results in Polio is by holding everyone accountable. To use his words, global health, very much like soccer, requires a coach to put his best players on the field. Throughout the continent, children are healthier and better protected from infectious diseases, most notably of course from polio, thanks to the tremendous efforts and tireless work of Pascal. This continent owes a huge debt of gratitude to Dr. Mkanda. On behalf of all mothers of Africa, I can simply only say one thing: Thank you, Pascal!”
“Rotary and Rotary members across Africa have been at the forefront in the fight against polio since President Nelson Mandela shouted his rallying call in 1996 to ‘Kick Polio Out of Africa’,” according to Dr Tunji Funsho, Chair of Rotary’s Nigeria National PolioPlus Committee and one of TIME Magazine’s 100 Most Influential People in 2020. “We went from 75,000 children paralyzed each year, all over Africa in 1996, to Zero wild polio cases since 2016. An unparalleled public health achievement, which could not have happened without Pascal’s leadership, engagement, and expertise. On behalf of Rotary members across Africa, Pascal – thank you so much for everything that you have done. We all wish you a more than well-deserved retirement.”
“I can only echo what others have already said,” commented Professor Rose Leke, Chair of the African Regional Certification Commission, which independently certified Africa as wild poliovirus free in 2020. “It was my great honour, and together with my fellow Commission Members, to certify our continent free of all wild polioviruses. Dr Mkanda and his team across the continent were absolutely instrumental in this. As Director of Polio in the Region, he exhibited great leadership. He and his team helped us verify the absence of wild poliovirus, even from the most inaccessible and remote areas of Africa. They helped ensure that children everywhere, no matter where they lived, were reached with the life-saving polio vaccine. Dr Mkanda demonstrated truly the best of Africa. All I can say is a tremendous ‘thank you’ to him and his team. I wish him well in all his future endeavours.”

Dr Mkanda’s career started from humble beginnings in a small and remote village, Chintheche in northern Malawi, with virtually no infrastructure. Pascal, son of a stay-home mother and a primary school teacher in Nkhata Bay, started making ‘tough decisions’ very early in life. At a tender age of 13, he and his elder brother Justin left their home on foot, and walked 18 miles with no shoes, to look for what would eventually be their family’s home in search of a better education for him and his siblings.
This was only the beginning of the ‘tough decision making’ that Dr Mkanda is well-known for today. The young Pascal Mkanda continued with his education and was eventually identified as his district’s best performing student. At the time, the president of Malawi, His excellency Dr Hastings Kamuzu Banda, had initiated a programme offering the brightest pupils (top 2.5%) from each district in Malawi irrespective of sex or socio-economic status, the opportunity to attend higher education, at the prestigious Kamuzu Academy, and through this educational opportunity, Dr Mkanda performed exceptionally and was awarded a full sponsorship to study Medicine in the United Kingdom where he attained a medical degree at the Imperial University College London.
To just show how intelligent he was – Pascal was afforded an opportunity to also study for a degree in microbiology/infectious diseases at the London School of Hygiene and Tropical Medicine while at the same time pursuing a degree in medicine. In later life he went to the Rollins School of Public Health at Emory University in Atlanta, USA, and obtained a Master of Public Health.
Putting his theoretical knowledge into practical experience, it was not long before Dr Mkanda began making a very real impact on Malawi’s public health system, improving the health and lives of remote communities. He rapidly developed a reputation for solid, practical and effective work. Here he developed the traits that would characterize his entire career and for which he became so respected: the courage of standing up for his convictions; an ability to identify and promote new and excellent talent, that would help him establish relevant and pragmatic support teams across the region; a fearless dedication to step out of group thinking even if it meant standing alone against adversity; and, an absolute and unwavering commitment to achieving results.

Respected by peers and more importantly communities themselves, he rapidly caught the attention of the international development community while working in some of the most remote communities in Malawi. During a visit by the USAID Mission in Malawi to Nsanje District Hospital in the south of Malawi, Dr Mkanda’s work caught the attention of the Country Representative who immediately recommended him for a USAID-sponsored Global Health Programme which subsequently led to the beginning of his international career.
Starting out as a National Programme Officer in Malawi for the World Health Organization, and moving on to Zambia as an international staff, he met and established a long-term friendship with Dr Francis Kasolo (former VPD Regional Virologist). By the year 2000, Dr Mkanda was managing immunization activities for Eastern and Central Africa and would eventually lead polio activities in Nigeria and Ethiopia.
It was during his time as WHO Polio team leader in Nigeria and Ethiopia that these countries were able to make significant inroads in interrupting wild polio transmission. One contributing factor for this achievement was the introduction of the famous accountability framework that held every staff accountable for their work with those underperforming being replaced by “fresh legs on the football field”, in Pascal’s own words.
It was therefore not a surprise that when the position of WHO African regional polio coordinator was advertised, that Dr Moeti – then the new Regional Director for Africa – appointed Pascal to lead the fight against this disease in the Region.
Never losing focus on the need to reach every last child with polio vaccines, with support from Dr Moeti and the Bill and Melinda Gates Foundation, Dr Mkanda established a regional center for the Geographic and Information Systems (GIS). According to Dr Joseph Cabore, Director of Programme Management at WHO’s African Regional Office: “One very critical contribution by Pascal to the regional office, is the introduction of innovative technologies and solutions. It’s amazing to see in real time, where our frontline workers can reach during mass campaigns and outreach activities. Pascal, thank you for ensuring that we remain accountable to our African children and their families.”

“It has been a privilege to work alongside Dr. Mkanda in pursuit of a polio-free world,” said Dr. Chris Elias, President of Global Development, the Bill & Melinda Gates Foundation. “His commitment and dedication to eradicating polio have been vital to helping protect millions of children from this debilitating disease and helped achieve a WHO African Region that is now free of wild polio – a monumental achievement in global health. I am forever grateful to Dr. Mkanda for his work and partnership on ending polio.”
Michael Galway, Deputy Director Polio at the Bill & Melinda Gates Foundation, added this personal comment: “Working with Pascal over the past decade has been one of best parts of the job in helping to get rid of polio in Africa. I’ve always appreciated the passion and conviction he’s brought to the work, and his keen understanding of how to get the polio programme to perform at its best in some of the most difficult places. He’s been a role-model and a friend, and I’m grateful for both!”
It was in Nigeria – for a long time the global epicentre for polio – that Pascal’s leadership really came into its own.
Dr Faisal Shuaib, Executive Director of the National Primary Healthcare Development Agency in Nigeria, said: “Pascal Mkanda’s contribution to making Nigeria free of wild poliovirus cannot be overstated. It took innovative strategies and approaches to ensure that every child could be reached, and virus transmission effectively tracked, in hard-to-reach and inaccessible areas. Pascal helped develop and trailblaze novel approaches which ultimately led to our success. It really took rewriting the strategic rulebook, and these approaches are now being implemented in other high-risk polio areas. All for the benefit of the most marginalized children. Thank you, Pascal, we could not have done it without you and your leadership. We will miss you!”
Indeed, it is this same leadership by Dr Mkanda that led to the establishment of the Rapid Response Team (RRT), coordinated by Dr Ndoutabe Modjirom in the WHO Regional Office in Brazzaville to tackle the remaining form of polio, the circulating vaccine-derived polioviruses (cVDPVs): “Pascal, you are leaving big shoes to fill. We will need your kind of leadership to end all remaining forms of polio in our region once and for all. It will not be easy to finish this job without you.”
Pascal will be missed, as underscored by Aidan O’Leary, Director for the Global Polio Eradication at WHO Geneva. “On behalf of all partners and stakeholders, the Global Polio Eradication Initiative wishes you all the very best in your retirement and/or in your next chapter of life. We know of course that you will stay engaged in one capacity or another in this fight, and we look forwards to one day, very soon, to celebrate together with you the victory over all forms/types of polio worldwide once and for all. A big thank you, in particular for your leadership in certifying the Region free of wild polioviruses and for facilitating the introduction and roll-out of novel oral polio vaccine type 2.”
Congratulations on your retirement! Now you’ll have more time for sleeping in, fishing, reading, golfing and if you want to be a DJ-from G22, where it all started!
Shine on, le Mystique Dr Mkanda!