In 1996, wild poliovirus was paralysing more than 75 000 children in the African Region every year, and Nelson Mandela and Rotary International issued a call to “Kick Polio Out of Africa!” The task was daunting. Polio staff had to deal with highly mobile populations, restricted access to children because of conflict and insecurity, fragile health systems and a fast-moving virus. Nigeria, as recently as 2012, accounted for more than half of all wild polio cases worldwide.
Ridding Africa of the wild poliovirus in the face of such daunting obstacles was, in the words of WHO Director-General Dr Tedros Adhanom Ghebreyesus, “one of the greatest public health achievements of our time”. It is an achievement built on the dedication of health workers – mainly women – who traveled by every available means – foot, car, boat, bike and more – to reach children with the polio vaccine.
One of the greatest public health achievements of our time.
One of those workers, Lami Isah Kyadawa, supported polio “immunization plus days” for almost 12 years before joining the network of volunteer community mobilizers in Sokoto State, Nigeria, in 2015. In her time fighting polio, she has overcome vaccine hesitancy, countered misinformation and even lost the sight in one eye in an accident returning from a polio mobilization campaign. But, for Lami, the sacrifices have all been worth it:
“It makes me proud to know that I was part of those that ensured the eradication of polio came to pass in Nigeria and now we can focus on improving routine immunization and other diseases.”
Eradicating wild polio in the African Region is a monumental feat, not just because of the scale of the task but because of the coordination and leadership required at all levels of the Global Polio Eradication Initiative (GPEI) to get the job done. It involved strategists with imagination, who found solutions to reaching children in regions rife with conflict and insecurity. It required constant surveillance to test cases of paralysis and check sewage for the virus, and it relied upon the commitment of all 47 countries in the African Region.

Since 1996, nine billion doses of oral polio vaccine have been provided, averting an estimated 1.8 million cases of wild poliovirus on the continent. Building on this success, countries in the African Region are now using the polio eradication infrastructure’s robust immunization and surveillance capacities to strengthen their health systems. The infrastructure, with thousands of health workers and volunteers, community and religious leaders, parents and families mobilized to “Kick Polio Out of Africa”, provides a strong foundation for countering other public health threats.
Responding to the pandemic and laying a foundation for the future
Long before the coronavirus pandemic, stopping wild polio brought far-reaching benefits beyond saving children from paralysis, including protecting them from other vaccine-preventable diseases and detecting and responding to outbreaks.
Thus, when COVID-19 struck, the GPEI’s staff and infrastructure were in place and equipped to be the first to respond. Thousands of polio workers in the WHO’s African, Eastern Mediterranean and South-East Asian Regions shifted their focus to COVID-19. Polio emergency operation centres quickly adapted to respond to the pandemic through surveillance, contact tracing and specimen transport, provision of soap and hand sanitizer, distribution of training materials for medical personnel and front-line workers and coordinated engagement with community and religious leaders and media on mitigation measures.
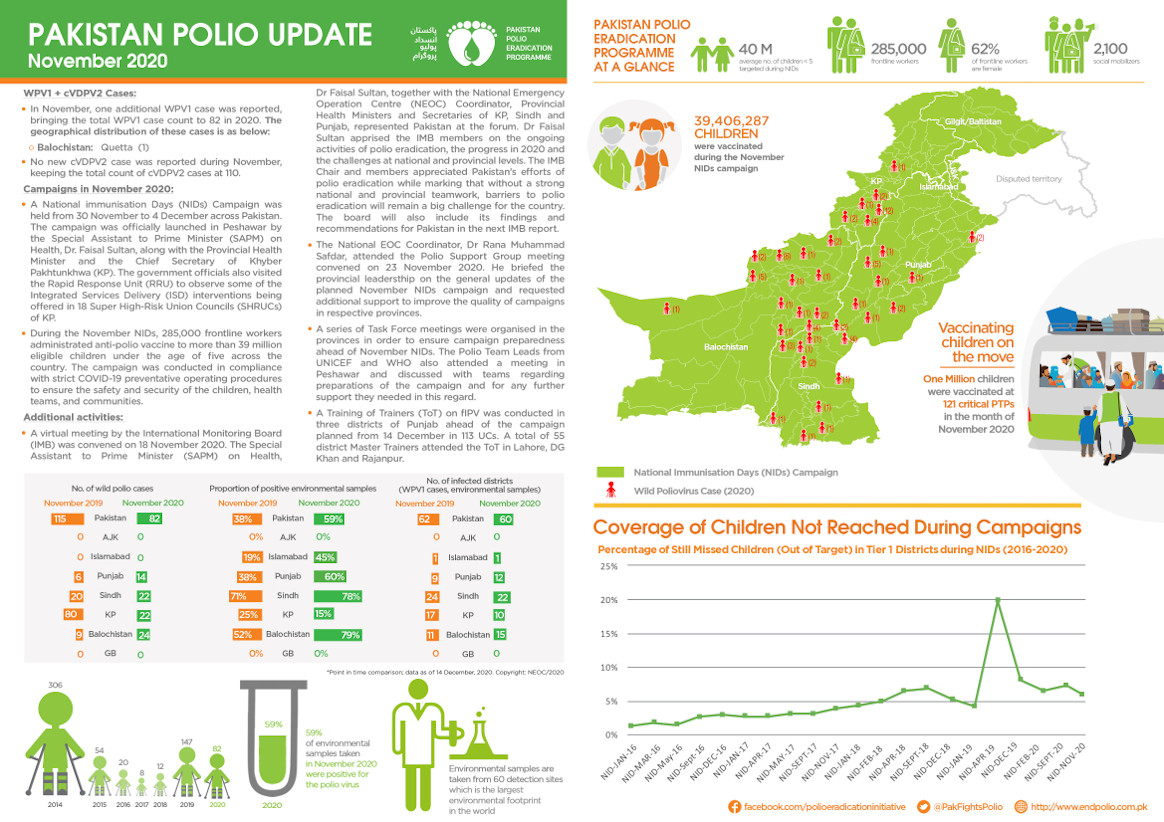
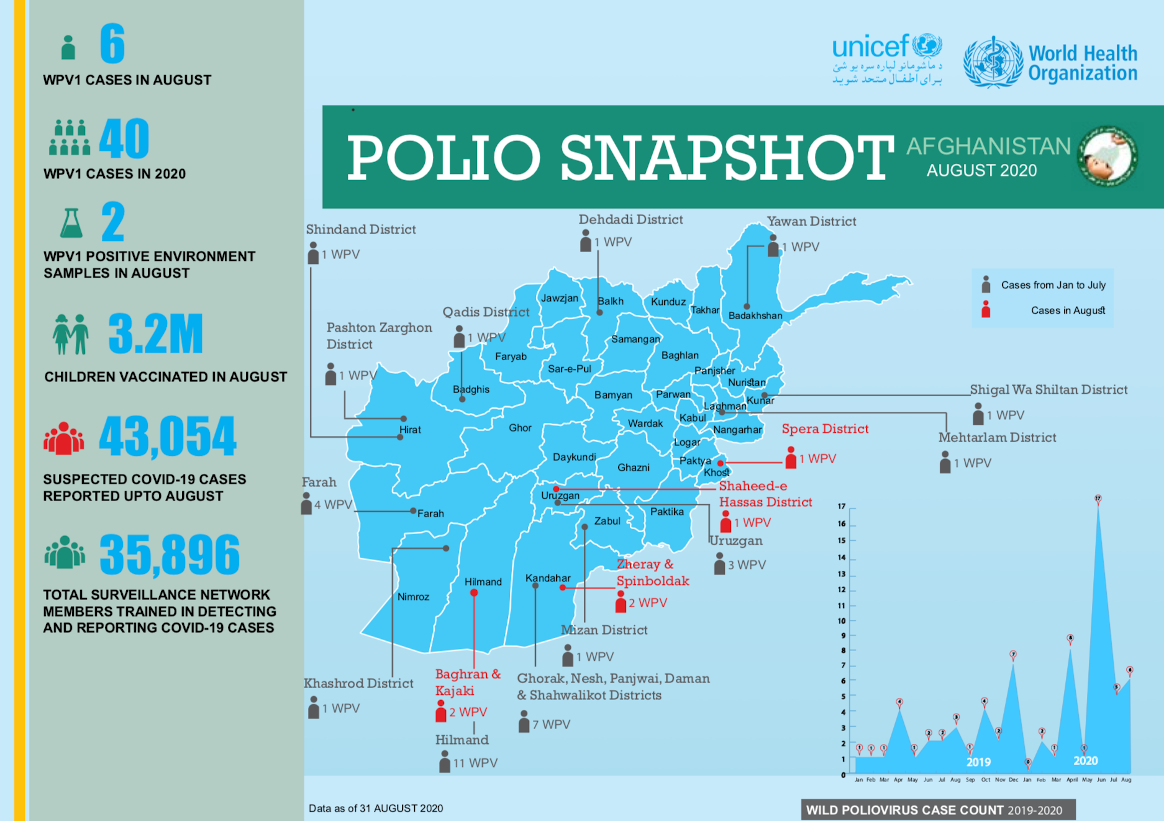
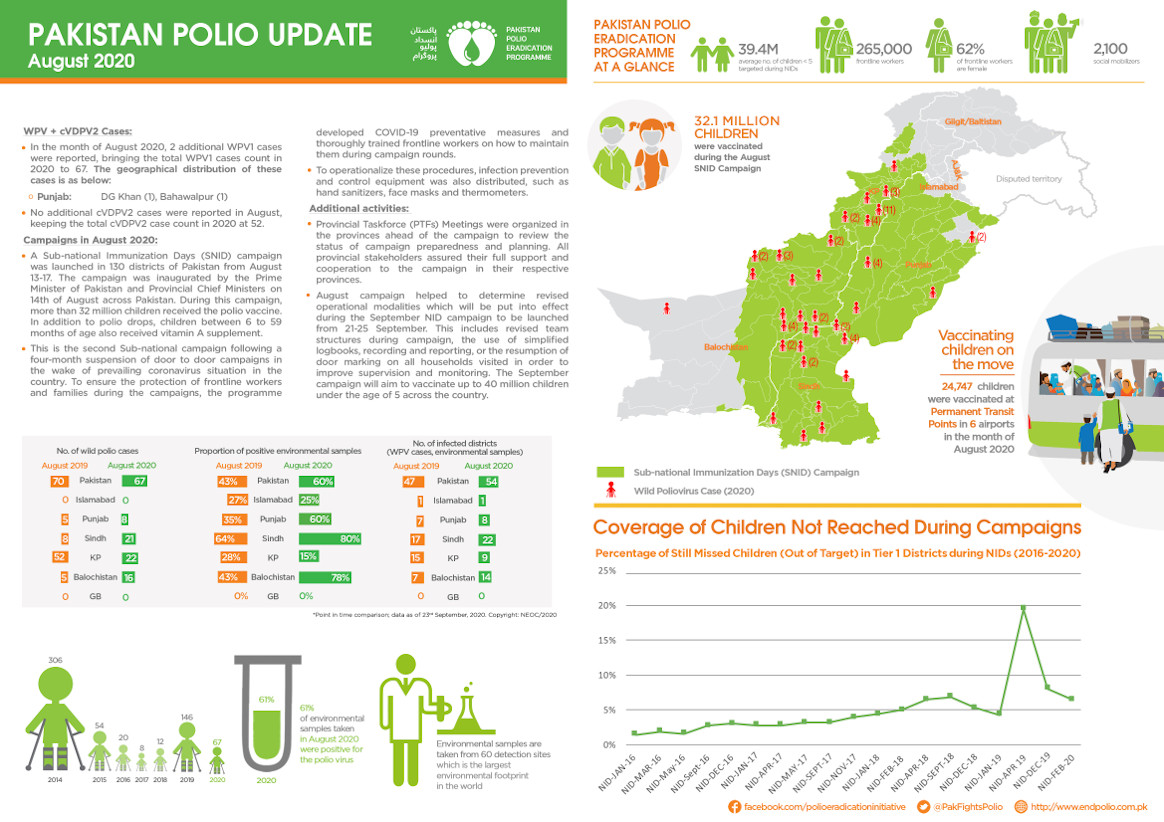
Polio staff have long been the eyes and ears of national health systems. In one example, polio laboratories in Pakistan provided COVID-19 testing and sequencing, while the polio eradication call centre became (and remains) the national COVID-19 hotline, dealing with up to 70 000 calls a day
Polio staff trained more than 18 600 health professionals, and polio community mobilizers engaged 7000 religious leaders and 26 000 influencers to provide information on COVID-19 to their communities. Through messaging applications, mosque announcements and public address systems on motorbikes and rickshaws, polio community outreach networks have reached millions of households.

How polio staff in Pakistan shifted their focus to COVID-19:
The pandemic has shown that the polio network can continue to serve other public health programmes, especially in health emergencies. For instance, in Pakistan, active polio surveillance at high-priority sites helped to confirm more than 1000 COVID-19 cases, more than 4400 suspected cases and nearly 500 probable cases. Staff have also used their expertise in data management to improve the quality and timeliness of data during the pandemic. This adaptable skill set makes polio personnel invaluable to health systems and communities.
Looking ahead, transition of polio personnel and infrastructure into public health systems is being planned in countries with large polio eradication programmes, led by national authorities. In places where there is insufficient national capacity, critical immunization, disease detection, emergency preparedness and response capacities will be supported by WHO’s immunization and emergencies programmes until national authorities can fully take over. Sustaining these capacities will require sustainable funding, but, as Africa’s remarkable achievement confirms, the wisdom of investing in polio eradication and sustaining its legacy is clear, as the networks set up for polio eradication will prove vital to advancing global public health security and achieving healthier populations.
Reposted from who.int.