28 May 2018, Geneva, Switzerland: ‘Eradicate first’ was the mantra at last week’s World Health Assembly (WHA). While holding detailed discussions to plan for a polio-free world, delegates emphasized the need to finish the job of eradication.
With wild poliovirus transmission levels lower than ever before, Ministers of Health and delegates reviewed progress being achieved through national emergency action plans in the remaining endemic countries. As at May 2018, only eight cases due to wild poliovirus had been reported globally, from just two countries: Afghanistan and Pakistan.
To prepare for a polio-free world, Member States adopted a landmark resolution on poliovirus containment. A limited number of facilities will retain poliovirus after eradication, to serve critical national and international functions such as the production of polio vaccine or research. It is crucial that these poliovirus materials are appropriately contained under strict biosafety and biosecurity handling and storage conditions, to ensure that virus is not released into the environment, either accidentally or intentionally, to again cause outbreaks of the disease in susceptible populations.
WHO and countries that are currently funded by the Global Polio Eradication Initiative (GPEI) face significant financial, human resource, and programmatic risks as a result of the scaling down of the GPEI budget (2017-2019) and its eventual closure. Hence, Member States requested the Director-General to develop a strategic action plan on polio transition that will mitigate these risks, as well as strengthen country health systems. Delegates considered the resulting 5-year strategic action plan on polio transition, which has 3 key objectives: (i) sustaining a polio-free world after eradication of polio virus; (ii) strengthening immunization systems, including surveillance for vaccine-preventable diseases; and (iii) strengthening emergency preparedness, detection and response capacity in countries to ensure full implementation of the International Health Regulations. The strategic action plan outlines how essential polio functions like surveillance, laboratory networks, and some core infrastructure can support the implementation of the Post Certification Strategy to sustain a polio-free world, and can be integrated into the immunization or health emergencies’ programme, or mainstreamed into national health systems. The plan provides detailed costing for the integration of essential polio functions into WHO’s Thirteenth General Programme of Work, and some financing options. The three polio-endemic countries (Afghanistan, Pakistan and Nigeria) and a few high-risk countries battling outbreaks have been excluded from transition planning until eradication. All other GPEI-funded countries are expected to plan for polio transition.
Member States expressed overwhelming commitment to fully implement and finance all strategies to secure a lasting polio-free world in the very near term. Rotary International, speaking on behalf of the GPEI, which includes WHO, Rotary, CDC, UNICEF and the Bill & Melinda Gates Foundation, offered an impassioned plea to the global community to eradicate a human disease for only the second time in history, and ensure that no child will ever again be paralysed by any form of poliovirus anywhere.
Almost everyone in the Killa Saifullah district of Balochistan, Pakistan, knows and respects 35-year-old Taj Muhammad. A dedicated and passionate doctor by profession, Dr Taj spends his days working as a Union Council Medical Officer in his local public health facility, and his evenings running a free medical clinic for local residents.
In his capacity as Medical Officer, he coordinates polio eradication efforts at the Union Council level, which is the smallest administrative unit in Pakistan.
His role includes coordinating microplanning, training frontline health workers, and supervising polio vaccination campaign activities. Since the start of his medical career in 2007, he has supervised more than 100 polio vaccination campaigns.
Dr Taj says he became a doctor to fill the existing health care gap in his area. “During my childhood, my mother was seriously ill and she died because of the absence of medical facilities in our area. She often used to tell me that I must become a doctor to help poor people with their health. She died afterwards but her words are still in my heart,” he explains.
His hometown, Killa Saifullah, is located 135 kilometers away from Balochistan’s provincial capital Quetta. Economic and social deprivation is widespread, and the district lacks basic health facilities, particularly for women and children. “There is only one hospital, serving only 150 people per day in the district, whereas the current population is more than 200,000. In these conditions, working as a medical officer is quite challenging,” Dr Taj says.
His job is tiring, and the demands are huge, but Dr Taj perseveres. As well as supporting polio vaccination activities, and endorsing vaccination, each day he tends to the large crowd of people who gather outside his evening clinic, often desperately needing health care.
His work to serve his community is particularly important because Killa Saifullah lies close to Dukki, where the only case of polio in Pakistan so far in 2018 was reported. Nawabzada Dara Khan, who chairs the Killa Saifullah’s Municipal Committee, notes that the community feels “vulnerable” knowing that the virus is close by.
Since the first polio case of 2018 was detected, polio vaccination campaigns have been conducted in response in all neighboring districts, including Killa Saifullah. But whilst this has increased immunity to the virus, it has also caused vaccine hesitancy amongst some parents, who question the need for multiple vaccination campaigns.
“We are trying hard to vaccinate each and every child; however, repeated campaigns and misconceptions are posing a big challenge for us,” Dara Khan says.
Luckily, the efforts of dedicated doctors like Dr Taj are helping to remove misconceptions and doubt. With the immense trust and respect he enjoys from his community, he has been able to use his free evening clinic as a local platform to advocate for polio eradication and the safety of the vaccine, extending his critical role in the polio programme.
Dara Khan adds, “The contribution of Dr Taj in polio eradication is commendable. His goodwill is playing a very positive role within our community to remove these misconceptions.”
His impact is also wide ranging, reaching multiple different families.
The proof? In April, thanks to the intensive efforts of Dr Taj and others, no parents or caregivers in Killa Saifullah refused vaccination.
That’s 70,690 children who now have lifelong protection from polio.
How do vaccinators ensure that every child is reached?
Every child needs to be vaccinated to protect them from poliovirus. To achieve this, detailed plans are prepared for vaccination teams. The aim is to find each child under 5 years of age – in Afghanistan, that’s around 10 million – and to reach them with vaccines.
A heavy steel gate opens on a quiet suburban street in central Herat. The city lies in a fertile river valley in Afghanistan’s west, an area rich with history. Over the centuries, invaders from Genghis Khan’s army to the troops of the Timurid empire, the Mughals and the Safavids have opened the gates to rule the city once known as the Pearl of Khorasan.
Now, a far more peaceful group can be seen walking down the streets of Herat. Equipped with blue vaccine carrier boxes and drops of polio vaccine, the teams knock on one door after another to vaccinate any children they find inside. The aim is to eradicate polio in Afghanistan.
Four-year old girl Fariba peeks from behind the gate and steps out on the street, followed by her father Mashal.
Mashal encourages his daughter to open her mouth to receive two drops of polio vaccine, and a drop of vitamin A. Fariba looks at the vaccinators with suspicion, but follows her father’s guidance.
The vaccinators thank them and continue down the street.
Locating all children
In March, vaccinators in Herat gave oral polio drops to over 150 000 children.
In a country with one of the highest rates of population growth in the world and frequent population movement, it is no easy feat to tell how many children live in each province, district, village, block, house or tent.
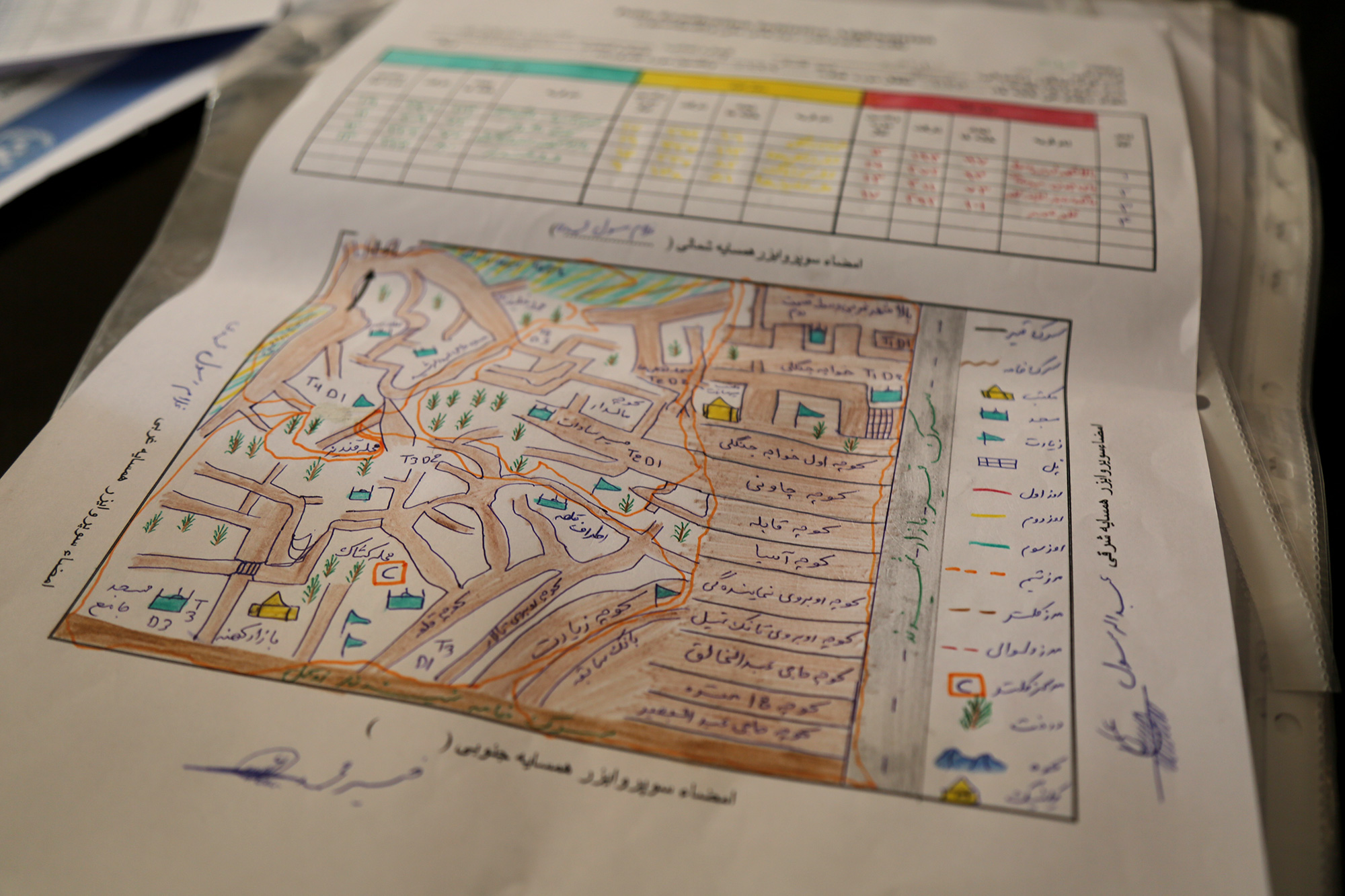
How do vaccinators know where the children in each area are located then? Through a simple but elegant guide known as a ‘microplan’. This is what the vaccinator follows: Where to start the day, how many children live on that street, which is the next house to visit?
No coincidence: Who goes where
A few kilometres from Fariba and Malik’s home, Dr Khushal Khan Zaman is sifting through printed plans on his desk at the World Health Organization office.
Dr Khushal explains that once a year, health workers physically count the houses in their area. Then they check that the plans from the previous year still match the numbers.
Campaign supervisors know the approximate number of children in each house from the last campaign. But the data is complemented by their personal knowledge. As locals, they often know of any changes in the composition of their community – where new children have been born, or the location of nomadic groups who have settled in the area.
This helps keep the plans accurate. For instance, if a nomadic group has stayed in an area for a longer time, their tents may be added to the microplans. For shorter stays, a separate checklist is used instead to monitor nomadic population movement. This improves the programme’s ability to trace and reach every child with vaccines, even if they are on the move.
Once the plans have been updated, teams of vaccinators are assigned to visit specific homes on a particular day during the upcoming campaign.
The final plan indicates not only the numbers of houses and children, but also details on how many related items are needed for each team: vaccine vials, vaccine carriers, ice packs (to keep the vaccines at optimum temperature), chalk, tally sheets, pens, leaflets, finger markers, plastic bags and scissors.
This is a contrast to a few years ago, when the plans listed only the name of the area with the estimated number of children to be vaccinated. The newer plans include even the smallest houses, and information on the closest mosque and local elders.
“It needs to be clear to everyone, which team is responsible for which area. We mark where the teams start and which direction they take using arrows,” Dr Khushal explains.
And it is no coincidence who goes where. To ensure that parents allow their children to be vaccinated, vaccinators may be allocated parts of their community that they know well, to increase trust when they deliver the vaccine.
Children like Fariba might not understand yet why the vaccine is important, but their father does. When vaccinators knock, it is not chance that brings them, but care and commitment.
Karachi, the capital of Sindh province, is Pakistan’s largest city, with an estimated population of more than 16 million people. It is also by far the most challenging place in Pakistan to eradicate polio. Difficulties include the large and frequent movement of people, poor water and sanitation conditions, and pockets of community resistance to vaccination.
In 2017, two of Pakistan’s eight total cases of polio were located in Karachi, and multiple environmental samples continue to test positive for the virus.
In the northwestern part of the city lies Orangi Town. The fifth largest slum in the world today, it is a tough place to live for the children who run around and play games in the streets outside their homes.
One of their most pressing needs is a supply of clean, drinkable water. In Orangi Town, the sewage system is basic, and poorly maintained. At many points, human waste mixes with drinking water lines. The quality of potable water is low and filled with pathogens including bacteria and viruses, and it is the main cause of many water-borne illnesses in adults and children, including hepatitis A, acute watery diarrhea and typhoid. Polio can also be spread through drinking water contaminated with the stools of an infected person.
Health workers for the polio eradication programme work tirelessly to immunize every child. But there are other ways to reduce the spread of the virus – and provision of uncontaminated drinking water is one of them.
Thanks to the efforts of Rotarians, who raised 50% of funds, 55 000 residents of Orangi now have access to a new water filtration plant. By ensuing that there are no viruses or bacteria present in the water, the plant will protect children from water-borne illness. As the plant runs using solar energy, it will work consistently through the regular power outages that affect the city, and won’t require expensive oil or electricity to run, placing fresh water within the reach of all.
Speaking on 8 May at the opening of the plant, Mr Aziz Memon, Chairman of Pakistan’s National Rotary PolioPlus Committee said: “This is the 15th water filtration plant installed in Pakistan, and the sixth in Karachi, and we will do all that we can with our partners to help raise the community’s standard of living including health.”
Dr Shafiq, a representative of Orangi Town, thanked Rotary International for its continuous support of polio eradication in the area. Combined with vaccination activities, children drinking the clean water provided by the new plant will now have an improved chance to grow up polio-free.
National Chair Aziz Memon said: “Orangi Town is one of the most underprivileged urban slums in Karachi and the supply of safe drinking water will improve health issues of the community and save children from water borne diseases.”
He added that “Rotary is making intensified efforts in this impoverished area and has established a Resource Center in Bijli Nagar Orangi Town.”
These extra steps towards ensuring that children are safe from disease also help to gain community trust, and form part of Rotary’s work to raise awareness of polio, and overcome vaccine hesitancy. In 2016, Rotary International contributed over US$ 106 million to polio eradication worldwide, and in Pakistan, Rotarians are at the forefront of the fight against the virus.
By chance, the opening ceremony of the plant coincided with the second day of this month’s subnational immunization days, when over 20 million children across different parts of the country were targeted with oral polio drops. Emphasizing the link between safer water, and polio eradication, children were given polio vaccine by high profile individuals attending the event.
Kicking off a safer future for some of Orangi’s children, Mr Memon and Rotary District Governor Ovais Kohari pushed a button at the plant to allow clear, safe water to flow from the taps. They then had a drink of water to test the quality and taste.
Simultaneously, polio vaccinators were going from house to house all over the city. For some families, Rotary was providing two life changing interventions in just one day – an effective vaccine, and water that they could finally trust.
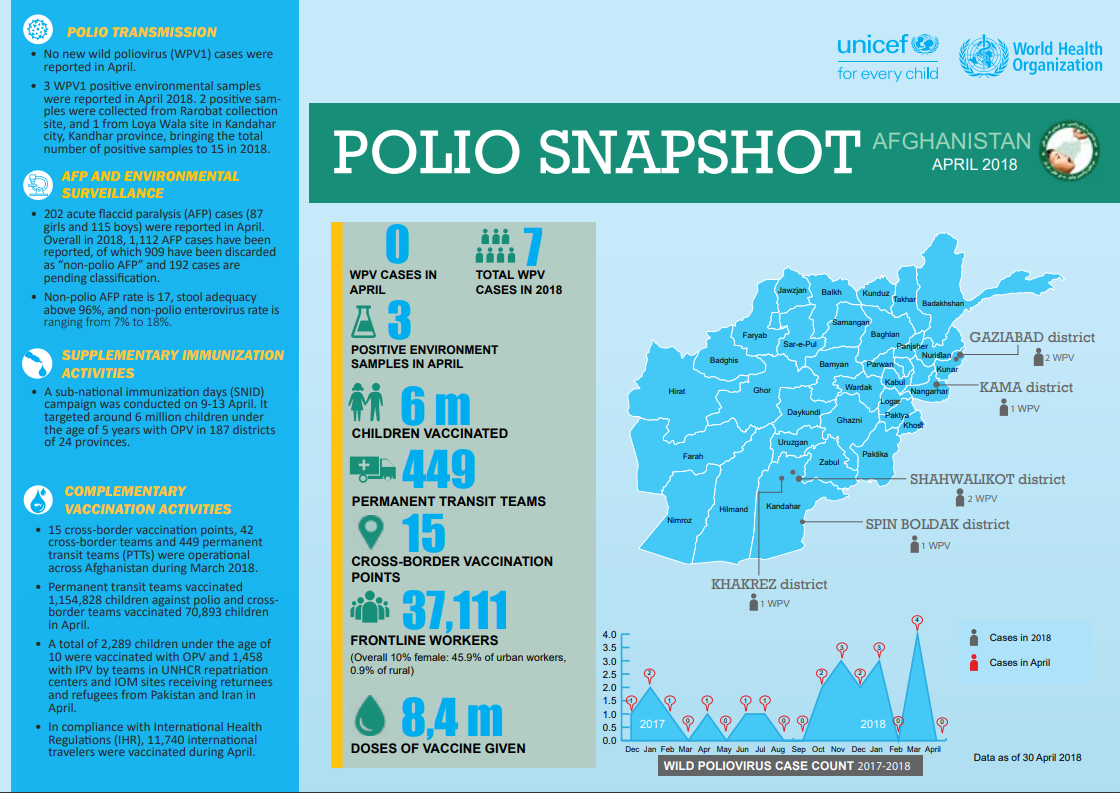
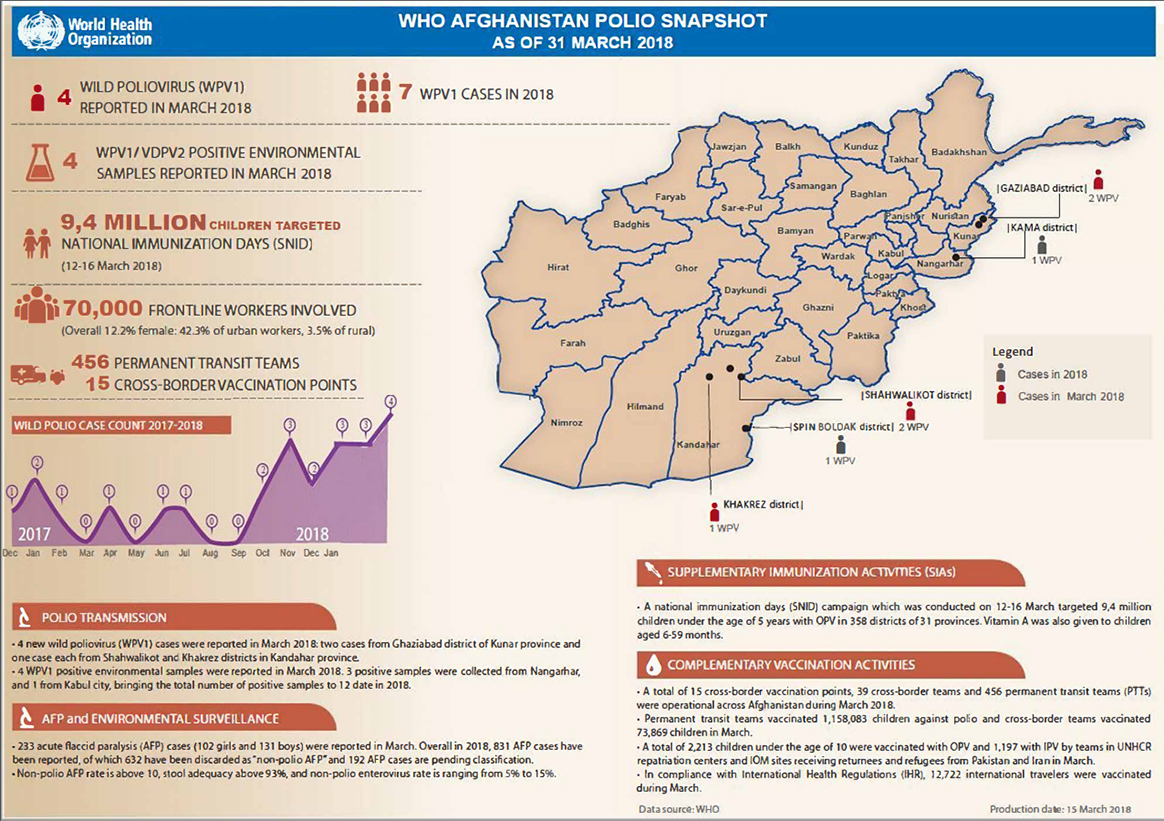
Four cases of wild poliovirus type 1 (WPV1) were reported, two cases from Ghaziabad district of Kunar province, and one case each from Shahwalikot and Khakrez districts in Kandahar province.
4 million children under five years of age were targeted during national immunization days in 358 districts of 31 provinces.
Permanent transit teams successfully vaccinated 1 158 083 children against polio, whilst cross-border teams vaccinated 73 869 children.
Last month, Canada signed a generous pledge of Can$ 100 million to help eradicate polio in Afghanistan as well as in the two other endemic countries, Nigeria and Pakistan, and to continue to protect many polio-free countries. The pledge was announced by the Honourable Marie-Claude Bibeau, Minister of International Development and La Francophonie, at the 2017 Rotary International Convention in Atlanta.
In addition to previous donations of approximately Can$ 650 million, this most recent funding consists of Can$ 30 million to WHO and UNICEF to support programme activities in Afghanistan, and Can$ 70 million of flexible funding that can be used to support vaccination campaigns, rapid outbreak response, poliovirus surveillance and other critical eradication strategies and activities to reach every last child worldwide with a safe vaccine.
This latter funding is especially valuable to the programme, as it will help sustain the priority areas of work that make global polio eradication possible. In 2017, there were 22 cases of wild poliovirus reported worldwide, from only two countries, Afghanistan and Pakistan. In Nigeria, wild poliovirus was last detected in 2016. However, since 2001, there have been wild polio outbreaks in 41 countries that were previously polio-free.
Flexible funding, such as that provided by Canada, is critical to allow the programme to react quickly to the most urgent needs, successfully stopping each outbreak, and ensuring that every child is protected from polio worldwide.
Minister Marie-Claude Bibeau used the signing as an opportunity to underline Canada’s ongoing commitment. “Canada has been a supporter in the fight against polio from the very beginning and we are committed to seeing it through to the end,” she said. “Keeping the momentum is key, particularly in Afghanistan, Pakistan and Nigeria, where polio still exists. Canada remains committed to ensuring every child is immunized, particularly girls, who continue to face barriers.”
As a champion of feminist development, Canada has particularly emphasized the role played by women in the programme, from the front lines, to programme management and political leadership. Polio eradication moreover forms a crucial part of Canada’s “Right to Health” commitment, and has the potential to become one of the first tangible outcomes of the UN Sustainable Development Goals.
Akhil Iyer, Director of the Polio Eradication Programme at UNICEF said, “Whilst polio exists in the smallest geographic area in history, this includes some of the most dangerous and difficult-to-reach parts of the world. Canada’s long-standing political and financial commitment helps our dedicated health workers, mostly women, go the extra mile and vaccinate every child to build a polio-free world.”
With this funding and ongoing support, Canada is striving to protect every girl and boy child. In doing so, Canada is making history.
The funding is also a testament to the major role played by the Canadian people at every level of the polio eradication programme. To date, Canadian Rotarians have raised and contributed more than US$ 52 million to eradication efforts, whilst Canada’s citizens have played an important role in tracking progress and publically voicing their support to end polio through the Scientific Declaration on Polio Eradication, and the One Last Push Campaign.
Michel Zaffran, Director of the Polio Eradication Programme at the World Health Organization said, “The ongoing support of Canada is fundamental to the programme’s success. With their global advocacy in international forums such as the G20 and G7 and their strategic and high quality support in Afghanistan and across the world, we can ensure that polio is eradicated forever.”
Canada’s contribution comes at an important time for the programme, in the run up to the 2018 G7 Summit. Previous summits have recognized polio eradication efforts, noting that programme assets also help to strengthen other aspects of health and development. This year, the Presidency is held by Canada, the first country to place polio eradication on the G7 agenda.
The Global Polio Eradication Initiative partners extend their profound gratitude to the Government and to the citizens of Canada for their tremendous support and engagement to end polio globally.
Binta Tijjani works to eradicate polio in her native Kano state of Nigeria. She is one of the over 360 000 frontline workers dedicated to ending polio in her country, the vast majority of whom are women. Nigeria is one of only three countries in the world yet to stop poliovirus circulation, together with Afghanistan and Pakistan.
Binta has worked in polio eradication for over 14 years. Starting as a house-to-house vaccination recorder, she was soon promoted to the role of polio campaign supervisor and now works as an independent polio campaign monitor.
“My biggest strength is my ability to work closely with our teams to ensure we reach every last child with vaccines, and advising teams so they can ask the right questions and raise important issues in each household they visit,” Binta says.
Working with the polio programme often opens up other opportunities for women to enter the workforce and utilize their skills to contribute to their communities, leading to positive investments beyond polio eradication.
“My work with the polio programme has enabled me to buy land and take care of my children’s school fees and our household needs. Currently I’ve enrolled in a course to get a certificate in catering. My dream is one day to open a restaurant,” Binta says.
Similar to Binta, Halima Waziri has been serving the polio eradication cause in different roles since 2005. Currently Halima works as a lot quality assurance sampling interpreter in Kano state, assessing the quality of vaccination coverage after immunization campaigns in her area.
“I am most proud of engaging in many productive dialogues about polio vaccination in remote and hard-to-reach areas and high-risk communities in Nigeria. This has helped me to improve my interpersonal communication skills and given me confidence in public speaking and influencing people,” Halima says.
With the money she has earned as a polio worker, Halima has opened a medicine store where she sells medicines and also acts as a community informant and focal point for disease surveillance.
Nigeria was on the brink of eradicating polio when a new wild poliovirus case was reported in 2016 after two years without any confirmed cases. Low overall routine immunization coverage is a key stumbling block to eradication, combined with ongoing violent conflict in the northeast where over 100 000 children remain inaccessible for vaccination teams.
Nigeria continues to implement an emergency response to vaccinate all children under the age of 5 to ensure they are immunized and protected, including implementing vaccination campaigns whenever security permits, vaccinating children at markets and cross-border points, and conducting active outreach to internally displaced people.
Without the critical participation of women as vaccinators, surveillance officers and social mobilizers, Nigeria would not be as close to eradicating polio as it is today. The latest nationwide immunization campaign, synchronized with countries in the Lake Chad basin, aimed to reach over 30 million children in Nigeria in April.
No wild poliovirus cases have been reported in 2017 or 2018. Binta and Halima, together with an army of frontline workers, are determined to keep it this way and secure a polio-free future for Nigeria.
Forty-year-old Auta A. Kawu says the only thing predictable about working in the conflict-affected northeastern Nigerian State of Borno is its unpredictability.
“No two days in my week are alike,” he says.
As a Vaccine Security and Logistics facilitator, Auta is one of 44 specialists working with the Government, UNICEF and partners in Nigeria, who strive to ensure sufficient vaccine stock, appropriate distribution and overall accountability for vaccines in the country. Through careful management, Auta works to give every accessible child in Borno protection from vaccine-preventable diseases, including polio.
Describing a typical week in his life, he explains that if on Monday he is arranging for the vaccination of eligible children among a group of Nigerians returning back from neighbouring countries where they had fled due to fear of violence, by Tuesday he could be speaking with government personnel to find a way to safely send vaccines to security compromised areas. On Wednesday, he may find himself rushing extra vaccines to an internally displaced persons (IDP) camp, where more people have arrived than initially expected, whilst on Thursday you may find him trying to locate a cold chain technician to fix a fridge where the heat-sensitive polio vaccine must be stored.
Evidencing the energy and commitment required to work on the frontline of vaccination, Auta notes that the work never lets up. Despite an exhausting week, on a typical Friday, you might find him on the road again, travelling to a remote location where health workers have just been given access. When he gets there, he will help out once more – trying to ensure that vaccines are distributed as effectively as possible to maximize the number of children reached.
He recounts a recent story of reaching the reception area of an IDP camp in Dalori, which is located in a highly volatile area of the state. Arriving with 300 doses of oral polio vaccine, and 200 doses of measles vaccine, he was told that new arrivals were expected later that day. Many of the people coming had been under siege by non-state armed groups since 2016, and had taken the opportunity of improved security and mobility to flee to the nearest town. Very few of the young children arriving had ever been reached with vaccines.
With the screening of children eligible for measles and polio vaccines starting around 9 am, and plenty more children yet to arrive, it was quickly clear that the available doses would not be enough.
Springing into action, Auta notified the head of the security team accompanying him of the need to go to nearest health facility to bring additional doses. Once clearance was given, he rushed to Jere Local Government, a district nearby, to collect more vaccines.
In the meantime, however, there were sudden changes in the security environment. The return journey to Dalori was not cleared until late noon.
Luckily, giving up isn’t in Auta’s nature.
By the end of the day, he had successfully delivered 580 doses of oral polio vaccine and 460 doses of measles vaccines for the children in the camp, providing some of them with their first ever interaction with a health system.
The crucial role of Vaccine Security and Logistics facilitators like Auta cannot be over-emphasized. In addition to his central work, Auta also conducts advocacy visits to traditional and religious leaders and supports the planning and implementation of vaccination campaigns in inaccessible areas.
Vaccine facilitation may be unpredictable work, but Auta is secure on one thing. Thanks to the work of him, and thousands of other determined health workers, community mobilizers and with support from donors and partners including the Bill & Melinda Gates Foundation, the Government of Canada, the Dangote Foundation, the European Union, Gavi – The Vaccine Alliance, the Government of Germany, the Government of Japan, the Japan International Cooperation Agency (JICA), Rotary International, the US Centers for Disease Control and Prevention, the World Bank and others, Nigeria is steadily on its way to being declared polio-free.
On top of the US$ 120 million committed in 2013, last year, HH Sheikh Mohamed bin Zayed pledged an additional US$ 30 million towards polio eradication, and the UAE is active on the ground in Pakistan through the UAE-Pakistan Assistance Program
UAE support also funded more than 5000 committed full-time vaccinators in highest-risk districts of Pakistan
Last year saw the lowest number of wild poliovirus cases in history (22 worldwide); Pakistan reported a 97 percent decline in cases between 2014 and 2017
GENEVA (16 April 2018) – The Global Polio Eradication Initiative (GPEI) announced today that the UAE has completed the US$ 120 million commitment made by His Highness Sheikh Mohamed bin Zayed Al Nahyan at the 2013 Global Vaccine Summit in Abu Dhabi.
“We thank the UAE for their long-term generous support and unwavering dedication to polio eradication, and particularly the personal commitment of His Highness Sheikh Mohamed bin Zayed Al Nahyan, Crown Prince of Abu Dhabi,” WHO Director General Dr Tedros Adhanom Ghebreyesus said. “This is the kind of support that will ensure we reach every last child to complete the job and to show the way to delivering health to all.”
Polio is a highly infectious disease that can cause lifelong paralysis, but it is entirely preventable with vaccines. Only three countries remain which have never stopped polio: Afghanistan, Pakistan and Nigeria. When the polio eradication effort was launched in 1988, 350 000 children were paralyzed by polio every year across 125 countries.
Polio eradication efforts have since made remarkable progress and there were only 22 cases in 2017 – the lowest ever recorded number. However, a number of key challenges remain. Reaching the most vulnerable children with the polio vaccine is hampered by a range of hurdles including difficult terrain, insecurity, and large-scale population movements.
Following the Global Vaccine Summit, the UAE expanded its role through the UAE Pakistan Assistance Program (UAE-PAP) to ensure that further gains would be made where it was needed the most. Through the “Emirates Polio Campaign” initiative, the UAE has helped drive on-the-ground eradication efforts within the most vulnerable communities in Pakistan.
Speaking about the UAE’s work, His Excellency Mohamed Mazrouei, Undersecretary of the Crown Prince Court of Abu Dhabi said: “The UAE’s pivotal role in eradicating polio completely is not limited to being a donor only, but extends to include its capacity to convene key groups and provide on-ground support to deliver vaccines in the highest risk areas of Pakistan.
“The UAE’s support – both as a leading donor and passionate advocate – has been critical for getting as close as we’ve ever been to making history by eradicating polio,” UNICEF Director of Polio Eradication Akhil Iyer said. “This is a gift not only to the children of Pakistan but to all future generations of children, everywhere, who are so close to the goal of being able to be born and be raised in a polio-free world.”
Dr. Chris Elias, President of the Global Development Program, Bill & Melinda Gates Foundation, said: “The UAE and His Highness Sheikh Mohamed bin Zayed Al Nahyan have shown an unwavering commitment to end polio, and we are delighted to partner with them in this effort. Without their involvement, achieving a record low number of polio cases in 2017 would not have been possible.”
The UAE is a longtime supporter of the polio eradication program. In addition to the US$ 120 million that His Highness Sheikh Mohamed bin Zayed Al Nahyan pledged in 2013, he pledged a further US$ 30 million to polio eradication, announced by Bill Gates at the Rotary International Convention in Atlanta, USA in June 2017. With additional commitments in 2011 and 2014, in total, the UAE has contributed US$ 167.8 million since 2011 to help end polio, with direct support to Pakistan, Afghanistan, Somalia, Ethiopia, Kenya, and Sudan.
The Global Polio Eradication Initiative (GPEI) is led by national governments and spearheaded by the World Health Organization (WHO), Rotary International, the US Centers for Disease Control and Prevention (CDC), and the United Nations Children’s Fund (UNICEF), with the support of the Bill & Melinda Gates Foundation. Since its launch at the World Health Assembly in 1988, the GPEI has reduced the global incidence of polio by more than 99%.
The GPEI receives financial support from governments of countries affected by polio, private sector foundations, donor governments, multilateral organizations, private individuals, humanitarian and non-governmental organizations and corporate partners. A full list of all contributors is available on the GPEI website, https://www.archive.polioeradication.org/financing/donors/
We talk to Professor Rose Leke, Chair of the African Regional Certification Commission, to get her views on progress on the continent, and prospects for certifying the region polio-free in 2019.
A unique group of people gathered last month in Sokoto state to commit to the twin goals of eradicating polio, and working to rapidly strengthen routine immunization. Bill Gates, and Africa’s richest man, Alhaji Aliko Dangote, joined traditional leaders from across northern Nigeria, Federal Ministry of Health officials, representatives from several State governments, and partners including UNICEF and WHO.
The two billionaires play a significant role in the fight to eliminate polio in Nigeria, where no wild virus has been detected since 2016. The Bill & Melinda Gates Foundation has committed US$1.6 billion in the country to date to fund pilot projects targeted at health care, agriculture and financial inclusion, a contribution which makes up their biggest investment in Africa. Aliko Dangote, who is Nigerian, has previously worked with Mr Gates to help interrupt transmission of the poliovirus in his country, and helps fund other health programmes as president of the Dangote Foundation.
During their visit, Mr Gates and Mr Dangote witnessed first-hand the progress Nigeria is making in polio eradication, routine immunization and primary health care provision.
At meetings held at the Sultan’s Palace and Governor’s House, Mr Gates highlighted the commitment of traditional leaders and reiterated the importance of engaging communities to reach every child with vaccines. Expressing his concern over the high infant mortality rate in Nigeria, he noted that vaccination is a cost effective way to save children’s lives.
Mr Gates also talked about the need to plan for the future of a polio-free Nigeria. Looking to how the polio eradication infrastructure can be used to help meet other health needs, Mr Gates said that the strong existing polio infrastructure – including vaccine supply chains, disease surveillance, laboratory systems and social mobilization networks – can be used to develop and improve routine immunization coverage for other diseases.
“We can prevent millions of deaths through routine immunization,” Mr Gates said. “We will not relent in our commitment towards this.”
Mr Dangote further highlighted that the fight against polio requires commitment from all stakeholders.
Drawing attention to malnutrition as one of the biggest factors undermining Nigeria’s progress, Mr Dangote urged the government and partners to reach out to private sector companies and ask them to donate at minimum 1% of their profits to financing the health sector.
At the meeting, the governors of Bauchi, Borno, Kebbi, Kaduna, Kano, and Sokoto States signed extensions of their Memorandum of Understanding on routine immunization. In doing so they reaffirmed their commitment to maximizing immunization coverage in their respective states, helping to protect every child against polio and other vaccine-preventable diseases.
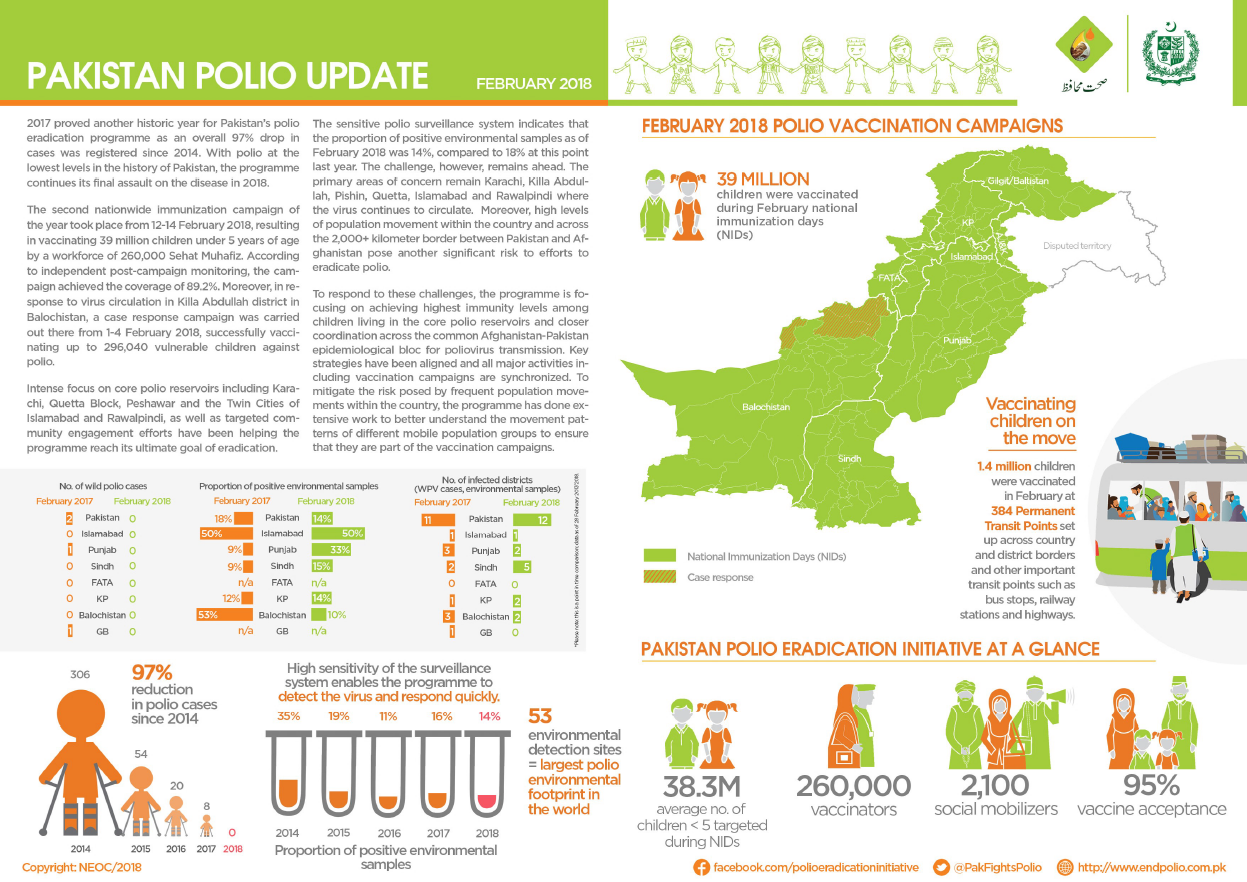
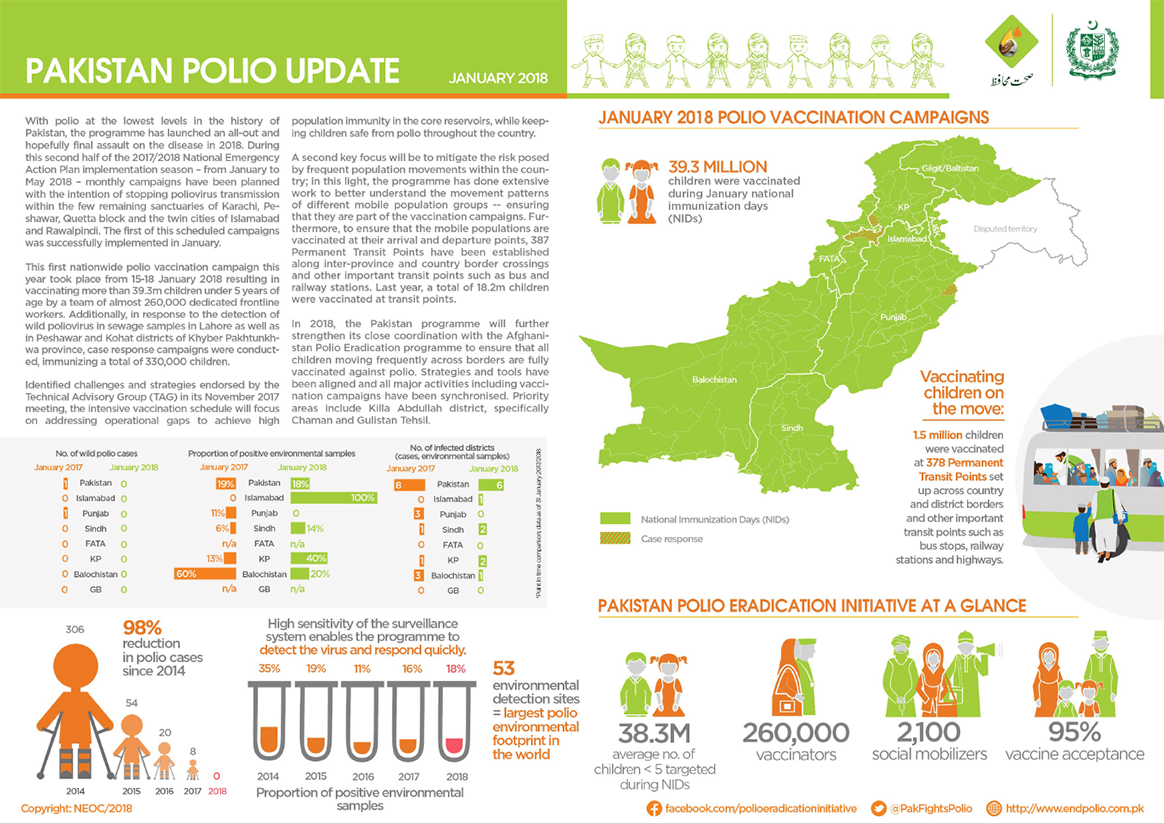
The Pakistan polio snapshot gives a monthly update on key information and activities of the polio eradication initiative in Pakistan.
In February:
No new cases of wild poliovirus (WPV1) were detected.
39 million children were vaccinated against poliovirus by a team of almost 260 000 dedicated frontline workers.
Teams at transit points and borders successfully vaccinated 1.4 million children.
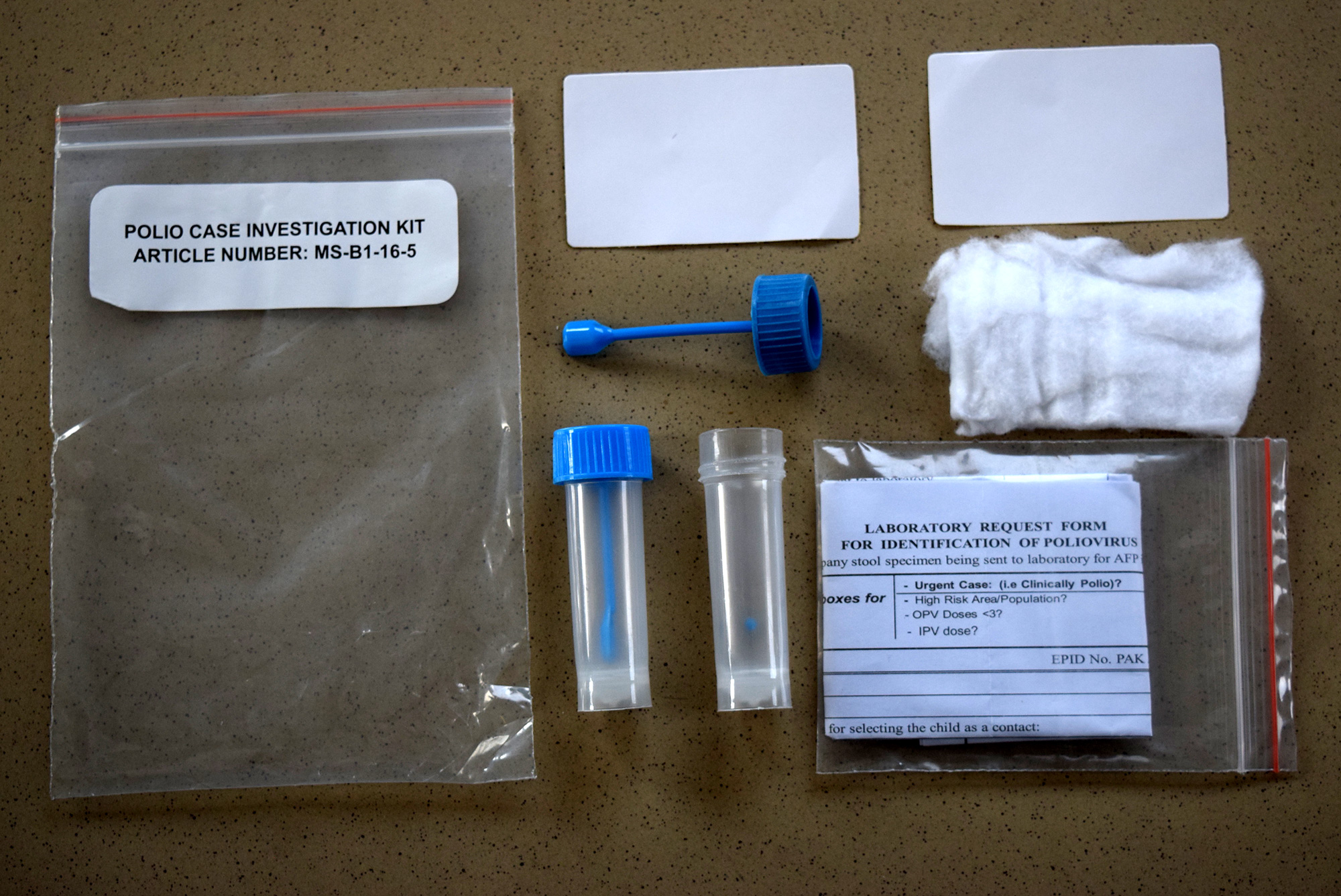
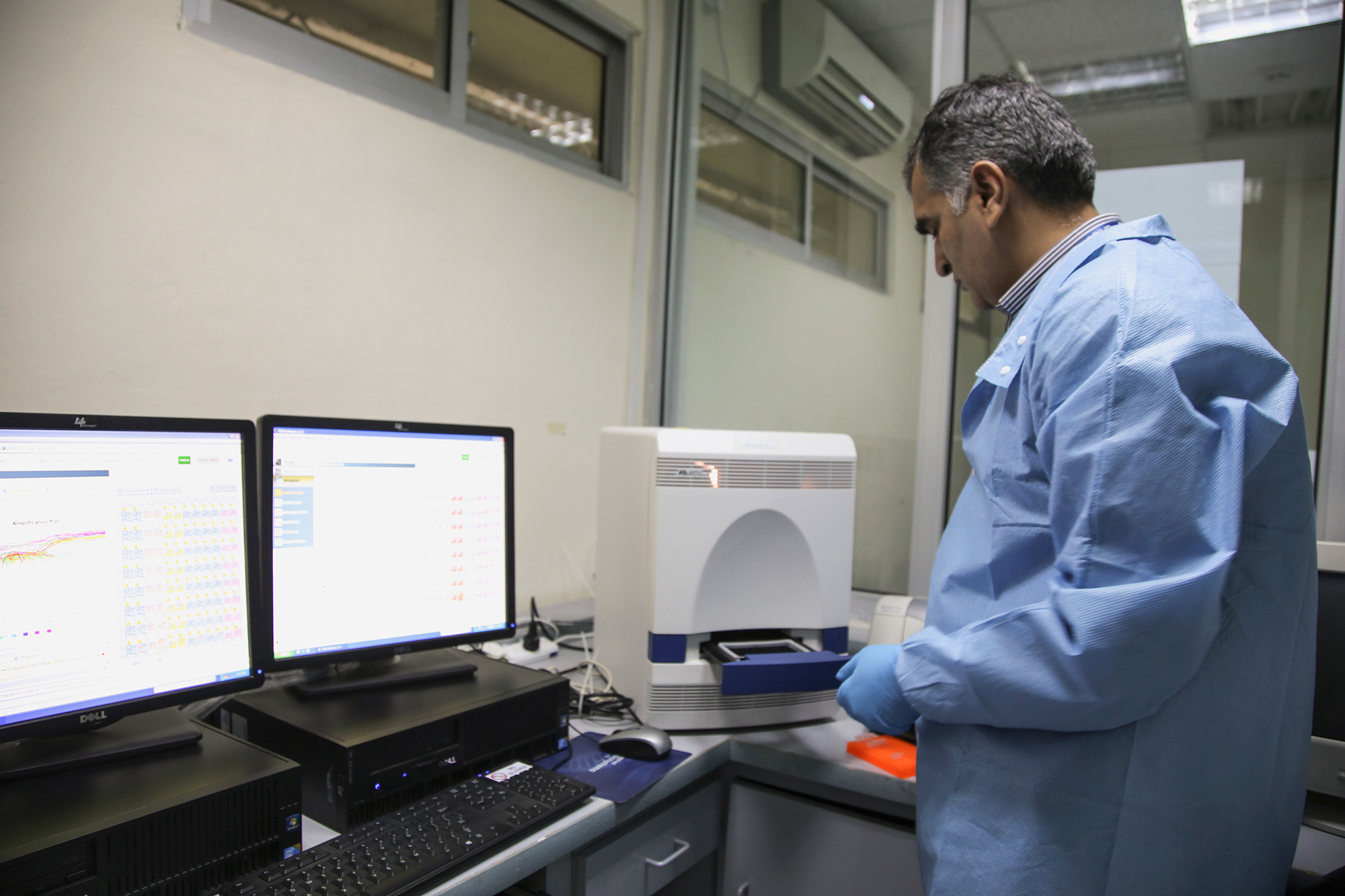
Surveillance is one of the main pillars of the polio eradication initiative. By testing stool samples collected from children suffering acute flaccid paralysis – the clearest symptom of the virus – as well as samples taken from sewage water, we are able to find the poliovirus wherever it is hiding.
Pakistan’s polio surveillance system is one of the largest ever established in the world. Click through these pictures to learn about the journey of a stool sample there: From a child with suspected polio to the laboratory.
In Pakistan, a wide network of health workers, teachers, and other community members vigilantly look out for signs of polio in children in their area. These volunteers detect and report to the polio surveillance system children showing possible symptoms of the virus, often floppy or weakened limbs with rapid onset of paralysis, known as acute flaccid paralysis. Every suspected case acts as a signal that polio might be circulating in the area, and triggers an investigation.
The poliovirus lives in children’s intestines, where it multiplies, and is finally excreted. When a child with acute flaccid paralysis is reported to the surveillance system, health workers collect the child’s stool samples and transport them to the lab in specially designed cool boxes. The boxes ensure a constant temperature of between 4 to 8 °C, so that the viruses in the samples remain high enough quality to test. Once collected, stool samples from all corners of the country must reach the Pakistan Regional Reference Laboratory for polio eradication, based in Islamabad, within 72 hours.
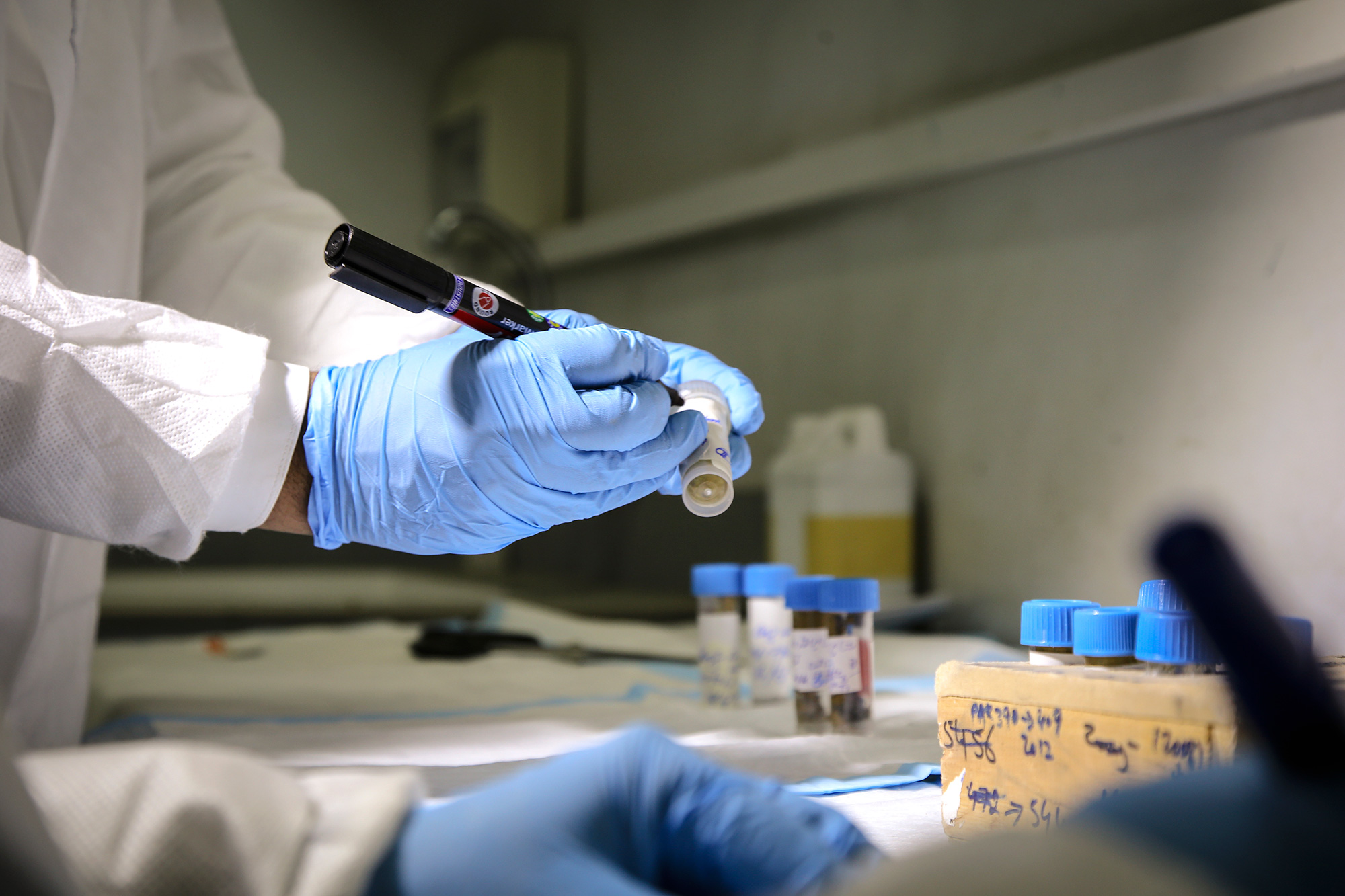
The Regional Reference Laboratory was established in 1991 and tests around 30 000 stool samples each year from both Pakistan and Afghanistan. More than 99% of these stool samples come back negative for polio. This is because most cases of acute flaccid paralysis are not caused by poliovirus. However, the tiny fraction of positive results tells the programme where the virus may be hiding.
Dr Salmaan Sharif is a Molecular Biologist, and the Coordinator of the Regional Reference Laboratory in Islamabad. He supervises a team of 34 lab staff, each responsible for a different component of surveillance sample testing. With an increase in reported acute flaccid paralysis cases, and environmental sampling sites, the workload of Dr. Sharif and his team is increasing. This is a sign that the polio surveillance system is working well, as a large number of reported acute flaccid paralysis cases and environmental samples gives us our best chance of finding the virus.
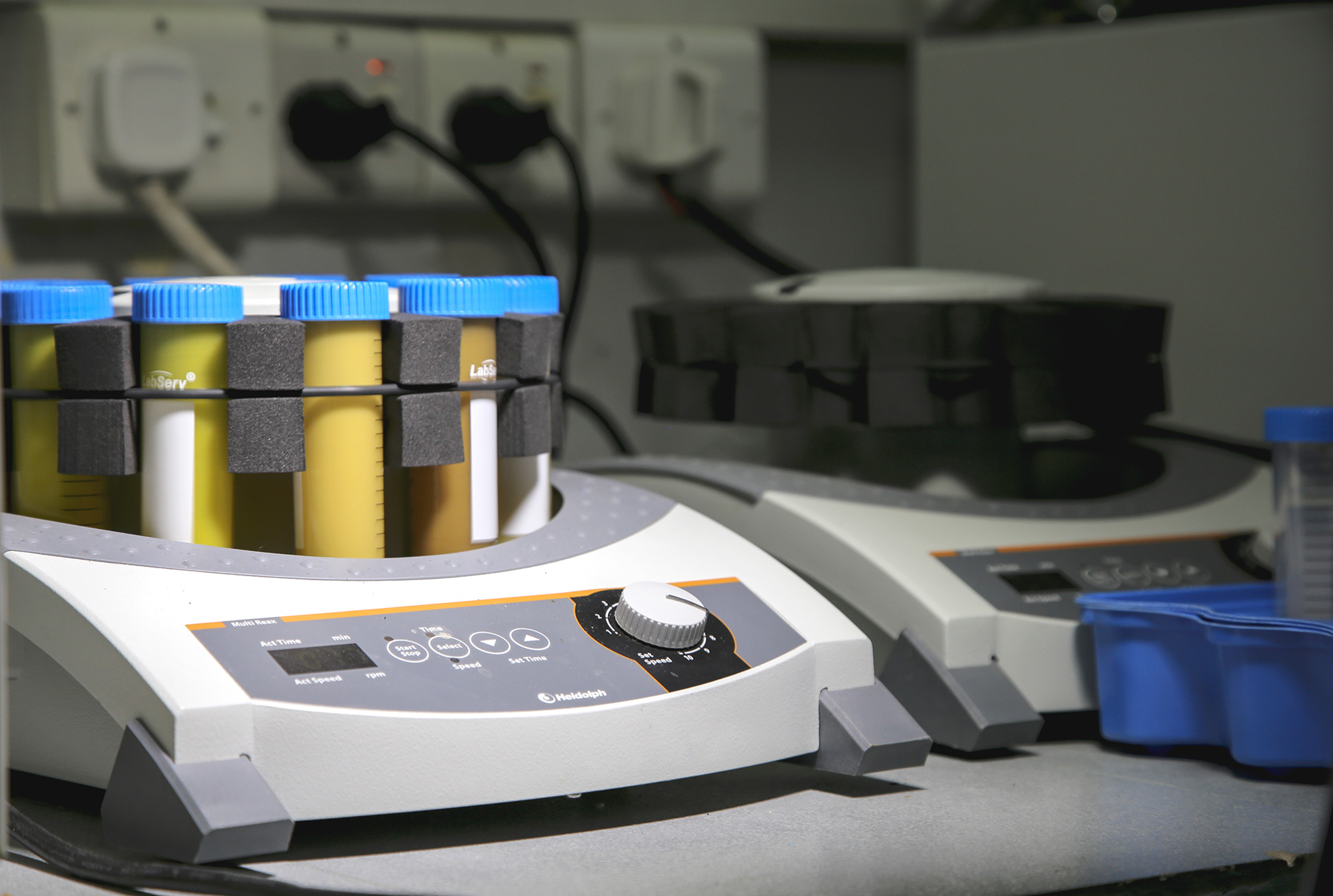
Each sample is then processed in a centrifuge, which separates the components of the sample. Solids will drop to the bottom and liquids will remain at the top. Any poliovirus will remain in the liquid component. Once separated, a scientist is ready to inoculate a healthy cell.
From the processing room onwards, extensive biosafety measures are taken to ensure that all virus is kept in the controlled environment, that contamination of other samples does not occur, and humans are not at risk of exposure. During the primary screening, healthy cells are mixed with the liquid component of the processed stool sample, and are then grown in an incubator at 36 °C for up to ten days. An incubator mimics the natural environment of the virus, creating the ideal conditions for the virus to grow. If the virus is present in the processed stool sample, it will infect the healthy cells.
A daily microscopic examination is performed to determine whether poliovirus is present in the processed stool sample. Infected cells are visibly broken in pieces, while healthy cells are seen as long strands.
If poliovirus is isolated in a stool sample, further tests are carried out to determine what type of virus this is and where the strain may have originated. A Polymerase Chain Reaction (PCR) machine is used to determine the kind of poliovirus detected (known as the serotype), and to distinguish further between wild poliovirus and that related to the vaccine-derived.
The next step is genetic sequencing. By reading the genetic code of the virus, wild viruses can be compared to others and classified into genetic families. From this, the geographic origin of the virus can be determined. This helps to guide the programme when deciding the best immunization strategies to stop transmission, and to prevent further spread of the poliovirus.
The polio surveillance system stretches even further than stool sample testing. In carefully selected places where the virus could be hiding, surveillance officers collect sewage samples. These are also sent to the Regional Reference Laboratory for processing, using a method similar to the testing of the stool samples. Crucially, environmental surveillance can help find polio in the environment before it has a chance to paralyse a child.
In Pakistan, the programme has used environmental surveillance to test and detect the presence of poliovirus in the sewage in high-risk locations since 2009. The network has continued to expand over time with a wider coverage. Currently, there are 53 sampling sites in 33 districts and towns of the country, making it the largest environmental polio surveillance network ever established.
The sensitive polio surveillance system finds the poliovirus wherever it exists – from the most remote villages to huge cities. With the polio case count at the lowest level in the history of Pakistan, the country intends to make 2018 the year of poliovirus interruption, keeping current and future generations of children safe from this disease. Thanks to the generous support of the Government of Japan, the Islamabad laboratory is continuing to expand operations, now able to procure new state-of-the-art molecular biology equipment to help detect the last remaining reservoirs of the virus.
In March, the Afghanistan polio eradication initiative conducted its first nation-wide immunization campaign for polio eradication in 2018. In just under a week, around 70 000 workers knocked on doors and stopped families in health centres, city streets and at border crossings to vaccinate almost ten million children. What an incredible achievement.
But what does a huge campaign like this take?
We had a look behind the scenes and followed the week in Herat, western Afghanistan. See what the campaign looked like from beginning to end through this photo essay.
First there are the vaccines. Throughout the year, millions of doses of vaccines are stored in cold rooms across the country, ready to be used in immunization campaigns. Here, cold chain manager Ghulim Said shows oral polio vaccine vials − the primary vaccine used for polio eradication − which are stored in the Herat regional EPI vaccine storage facility.
Before each vaccination campaign, the polio programme draws detailed maps of where each team will head. These maps are called “microplans” and they show streets, landmarks and each house that vaccinators must visit during the campaign days.
A week before vaccination begins, polio workers start preparing. For this campaign, more than 70 000 volunteer vaccinators and other polio workers were selected and trained in vaccination, finger marking and campaign monitoring. In Herat, students Jami Mansoora (left) and Asma Hakimi (right) were trained as campaign monitors.
One day before the campaign, vaccines and other supplies were picked up from storages to be taken to the teams. These vaccines were taken from Herat regional hospital to a nearby district. They were kept in cold boxes to maintain vaccine quality.
To mark the start of the week-long effort, inauguration ceremonies were held across the country. Herat provincial governor Asef Rahimi vaccinated local children during one such ceremony.
On the first day of the campaign, banners were hung on roadsides, mosques, and health centres all over the country announcing the campaign and encouraging parents to vaccinate their children. This banner was hung on the side of a busy street in Herat city.
In the morning, the blue boxes used to keep vaccine vials cold were packed and picked up by the vaccination teams. Shireen Gul Azizi packed her bags before leaving for the day’s work. She works as a supervisor and manages three vaccination teams.
With the teams on their way, vaccination began. They walked from door to door, knocked and gave two drops of polio vaccine to every child they could find.
Ali Yaser, age 4, was vaccinated on the first day of the campaign in Herat city. All vaccinated children were also given drops of vitamin A to boost their immunity.
In addition to the house-to-house teams, mobile and transit teams worked across the country to reach any children on the move. At the border crossings, travellers were stopped and their children vaccinated. At these points, all children under ten years old are vaccinated. Mohammed Hussain Farhang, age 6, was returning from a holiday in Iran with his family. At Islam Qala border crossing vaccinator Bashir Ahmad gave him two drops of polio vaccine. He found finger-marking funny and couldn’t stop giggling.
During the campaign week, mobile teams also vaccinated children on the streets and outdoor markets. Farzad, age 16, was working by himself in the centre of Herat. In a single day, he vaccinated tens of children.
Every evening after the rounds, the vaccinators and cluster supervisors got together for a meeting to discuss any problems that might have been encountered during the day’s work.
On Thursday, three days into the campaign, the vaccinators took a break and collected numbers on how many children had not been home or had missed vaccinations for other reasons. Detailed plans were drawn and maps created showing each team which houses still needed to be revisited on the last day.
In some places, more vaccines were needed. Rickshaw driver Khalil Ahmad played his part in ensuring that every team had enough vaccines, driving more supplies to a neighboring district for the final revisit day.
On the morning of the last campaign day, cluster supervisor Ahmad Rashid examined his map to see where the five vaccinator teams he managed would be heading. He knew the revisit day was important during every campaign: this was the chance to reach every last child in his area.
One of Ahmad Rashid’s teams, vaccinators Sumaya Hakimi (left) and Sohaila Hamidi (right), started working at eight in the morning. From their maps they could see that they had missed 36 children during the week. By 11 a.m., they had already found 30 of the children at home and had vaccinated them.
Success! Moheburrahman, age 3, was not vaccinated earlier in the week when the team visited, as his mother was worried about the vaccine’s safety. The team talked with the family again, carefully explaining why the polio vaccine is so important, and taking time to discuss their concerns. Reassured that the vaccine is safe, little Moheburrahman’s mother allowed the vaccination to go ahead.
One last child protected against paralysis. Little one-day-old Fatima received her first ever vaccination on the last day. She could not be vaccinated earlier, as she had not been born yet.
After the campaign, more than 1 800 independent monitors were deployed to find any missed children and record the reason they were missed. This information will help preparations for the next campaign.
In a local health centre in Herat, Najibullah Mohammadi conducted a finger-marking survey to check if every child had a little blue pen mark on their fingers. On little babies the mark was drawn on the ear – an easy way to show they have been vaccinated whilst keeping them wrapped up warm. 45-day-old Rokshana was found to be vaccinated.
Rokshana and every child deserves a healthy, polio-free life. Thanks to the work of the thousands of volunteers and polio workers, Afghanistan is one step closer to eradicating the disease.
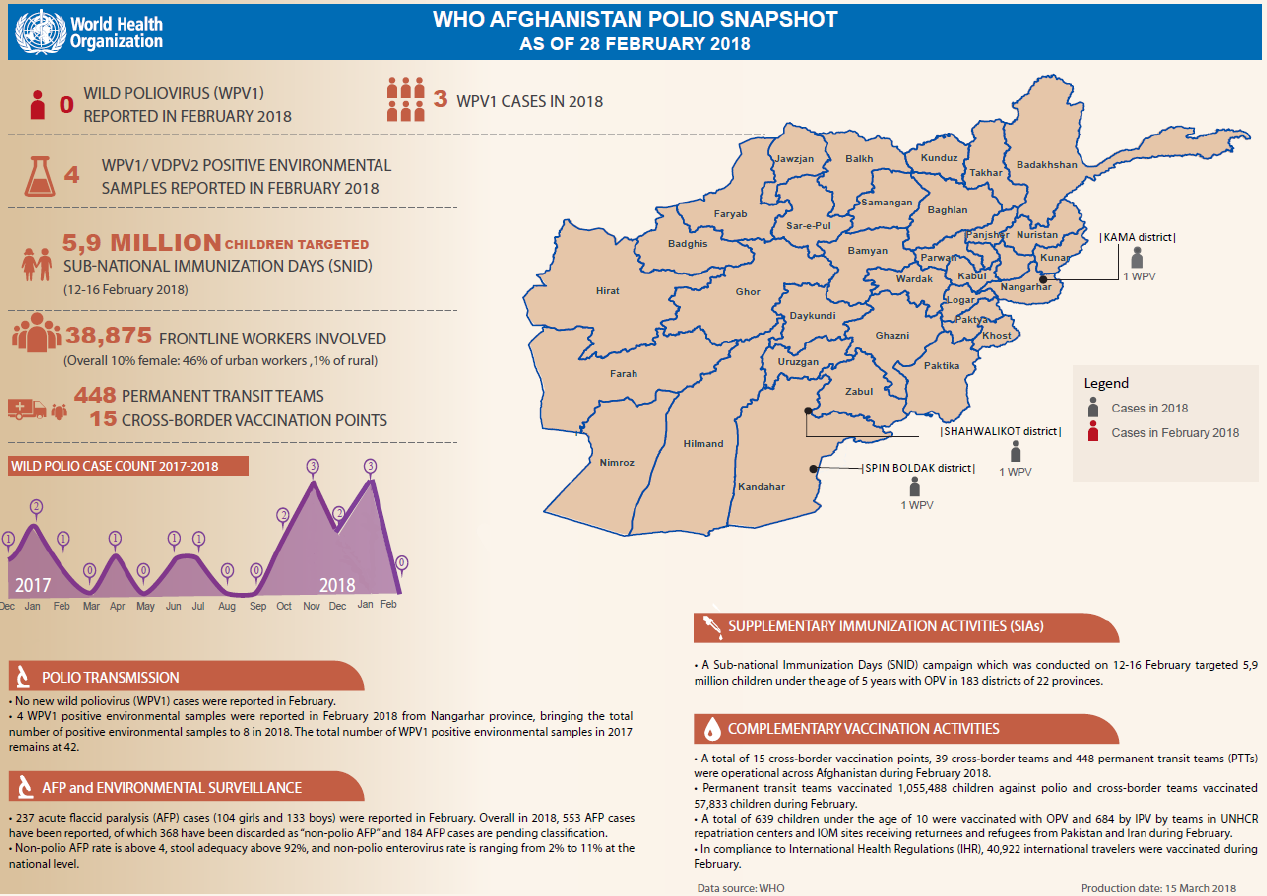
The Afghanistan polio snapshot gives a monthly update on key information and activities of the polio eradication initiative in Afghanistan.
In February:
No new cases of wild poliovirus type 1 (WPV1) were reported.
5.9 million children under five years of age were targeted during subnational immunization days across 22 provinces.
Permanent transit teams successfully vaccinated 1 055 488 children against polio, whilst cross-border teams vaccinated 57 833 children.
“When I received the confirmation of the first case of Lassa fever…nothing prepared me for the tasks ahead other than my work in polio eradication” – Mrs Faith Ireye, WHO State Coordinator in Edo state.
In the first two months of 2018, there were 110 deaths in Nigeria from suspected Lassa fever. Outbreak response, led by the Nigerian government and WHO, is focused on detecting every case, and tracing the virus wherever it is hiding.
Bolstering this effort are individuals with experience of guarding against a different disease – polio.
Ms Ireye, who has worked with the Global Polio Eradication Initiative for over ten years, is currently helping to coordinate the Lassa fever outbreak response in Edo State, one of the hardest hit by the outbreak.
“My experiences in polio eradication activities allowed me to immediately swing into action. So, when the [Lassa fever] outbreak was confirmed, I realized the need to use my expertise to serve communities at risk,” she says.
Part of her job is to help coordinate surveillance, specifically ensuring that everyone who has come into contact with someone with Lassa fever is found, and tested for the virus.
Her work is critical to help prevent further fever cases. Deputy Governor of Edo State, His Excellency Philip Shaibu said, “WHO…is one of the pillars that have helped lead surveillance in Edo state… In this particular outbreak, WHO was the first to draw attention to the fact that we need to galvanize resources from all partners, from other parts of the country, to ensure that things get done.”
The polio infrastructure
When outbreaks of other diseases happen, the knowledge and experience of polio personnel like Ms Ireye can make a significant difference to outbreak response. For example, polio workers were essential to containing the Ebola virus outbreak in 2014. For the Lassa fever response, 271 polio workers are involved in active case search, 235 in contact tracing, and 320 in community sensitization activities across the 18 at-risk states.
“The polio infrastructure was originally designed towards achieving the polio eradication goals,” said Dr Wondimagegnehu Alemu, WHO Country Representative to Nigeria. “Now polio infrastructure has expanded its support to broader disease surveillance strengthening, outbreak response and basic health care services including immunization.”
Other activities carried out by polio workers include data collation and analysis, and case reporting.
“The polio teams on ground in the states were crucial for mounting the initial response to the Lassa fever outbreak, and have continued to be WHO’s frontline technical support to the NCDC, States Ministry of Health and local government area teams,” Dr Emmanuel Musa, WHO Incident Manager for Lassa fever Management Team in Nigeria observed.
A legacy for posterity
Investments by donors and partners have gone far beyond polio eradication. Reflecting the positive impact that polio infrastructure and knowledge has had on other health priorities such as Lassa fever, WHO and other partners are currently supporting the development of a national transition plan. This will ensure that the investments that have brought the world to the brink of eradication are made available to support other national public health efforts, long after polio has been defeated.
“We must carefully consider how we transition many of the polio workers and the polio infrastructure to help with managing other health needs,” Dr Alemu said. “Future funding and partnerships will be a key part of this work.”
For now, experienced polio personnel continue their work to end the Lassa fever outbreak. Thanks to them, and the support of governments, partners and donors, we are ending polio, and are also helping to strengthen other health interventions.
Support for immunization to the Federal Government of Nigeria through the World Health Organization is made possible by funding from the Bill & Melinda Gates Foundation (BMGF), the United Kingdom, the European Union (EU), Gavi, Global Affairs Canada (GAC), the Government of Germany, the Japan International Cooperation Agency (JICA), the Korea Foundation for International Healthcare (KOFIH), the Measles and Rubella Initiative (M&RI) through the United Nations Foundation (UNF), Rotary International, the United States Agency for International Development (USAID), the United States Centers for Disease Control and Prevention (CDC) and the World Bank.
Zulaihatu Abdullahi is well known in her community, particularly to the mothers. As a volunteer community mobilizer in Kaduna state, northern Nigeria, her mission is to ensure that no child contracts polio, or any other preventable childhood disease.
This is difficult, as immunization programmes are sometimes treated with suspicion in her part of Nigeria. As a ‘change agent’, Zulaihatu’s job is to go door to door, counselling parents about the importance of the polio vaccine.
This particular lunchtime, she is visiting an 18 year-old mother living in a compound in a densely-populated, urban district of Kaduna State.
The young mother puts down the pole she is using to pound millet and welcomes Zulaihatu, recognising her royal-blue UNICEF hijab. She sits, and pulls on a hijab for cover as she settles down to breastfeed her baby. She has three other small children at home, a fifth on the way and she is new to the area.
“Before I came here I was rejecting all vaccines,” she says, “but because of this woman, Zulaihatu, I decided to accept. She told me the usefulness and I was convinced to do it.”
Thanks to Zulaihatu’s patience, and her work to build trust with the younger woman through regular visits, four more children are now protected against polio who might otherwise still be at risk. The mother has also been encouraged to seek anti-natal care, and the youngest child has just received his routine immunization shots.
“Sister Zulaihatu was one of the first women I met when we moved here,” the mother recalls. “She came here every day. She told me how she takes care of her own children. What she feeds them. How they all take vaccines. Little by little I started to change my thinking.”
Zulaihatu is trained to make her community aware of important household and parenting practices to keep their children thriving. The list is extensive and includes tips to treat diarrhoea, the importance of basic hygiene and sanitation, how to protect the family from malaria, the benefits of neonatal care and breastfeeding for infants, and the importance of registering their births.
She is one of nearly 20 000 UNICEF-trained community mobilizers, influencers and communication experts spread across 14 northern ‘high risk’ Nigerian states. With the support of donor and partners including the Bill and Melinda Gates Foundation, CDC, Dangote Foundation, European Union, Rotary, GAVI, JICA, the World Bank and the Governments of Canada, Germany, Japan, and others, the mobilizers are a key part of UNICEF’s ongoing support to the Government of Nigeria’s immunization programme.
Despite their achievements, Zulaihatu and other mobilizers know that there is much is still left to be done in their communities. Tomorrow, Zulaihatu will continue her work, going from household to household to keep every child safe.
In eastern Afghanistan, one family is helping to vaccinate every last child in their community
Zahed, his daughter Sahar, and son Mohammad all work together. But they are not working for themselves, they are working to eradicate polio.
The family lives in an indigent village in eastern Afghanistan with a diverse community. It is close to the border with Pakistan and many residents are returnees from Pakistan, families displaced by insecurity and nomads passing through. With a population that is often on the move, it is a community with high risk of poliovirus transmission – making it extremely important to vaccinate every child.
Zahed’s family are well-known. Each month, they knock on doors giving free vaccinations and educating their community about the virus.
Although sometimes they don’t have doors to knock – only tents. Known in Afghanistan as Kuchis, nomads are particularly vulnerable to polio, because they move seasonally and often miss vaccination campaigns. Historically underrepresented and often neglected, they are also isolated from health services.
Nomads at risk
Laden with water jugs, cooking equipment and clothes, the Kuchi travel with their livestock and move between provinces depending on the climate. Their goats, sheep and camels are often exchanged or sold for grain, tents and other essential items. There are an estimated two million nomads in Afghanistan.
Over 120 nomad families with 194 children under the age of five recently arrived in Zahed’s village from shelters along the Kabul River. They come in the winter because it offers warmer, more fertile ground for their animals to graze. They return to Kabul and Bamiyan during the spring, when the land is more arable.
To eradicate polio in Afghanistan, every child must be vaccinated – including the nomads. And this is exactly what Zahed’s family are doing. They go to each tent, and ensure every child is protected against polio. Last week, Zahed’s 20-year-old son Mohammad vaccinated 719 children, including nomads. “My community are happy with my service. I’m young, and it is a privilege to make a difference,’’ says Mohammad.
The family is not only protecting children, they are also contributing to community cohesion and bridging divides between nomads and residents. The challenge, however, is continuing to vaccinate nomads when they are on the move.
The motivation of Zahed’s family is impressive, but it is not always easy. A handful of people in the village reject the vaccine because they think that it is unsafe or not halal – permissible in traditional Islamic law. But watching an entire family working to eradicate polio helps break misconceptions. At the start of each vaccination campaign, Mohammad gives one of his own children the vaccine to prove that it is safe.
Becoming advocates
Zahed’s family have turned almost all the families who were refusing the polio vaccine into advocates for vaccination. Mohammad was already a prominent member of the community and was previously given a ‘Turban’ – headwear used to recognize a person who makes decisions on behalf of their community and country – to honour his relentless work to improve water, sanitation and development in his village. Now his role as a polio eradication ambassador is developing trust and increasing acceptance of the vaccine.
In 2017, three polio cases and 14 positive environmental samples were reported in eastern Afghanistan. A positive sample indicates that the polio virus is present, and that children with low immunity are at risk of contracting the disease. The first polio case of 2018 was also reported in eastern Afghanistan, making it an urgent priority location for nationwide eradication.
In the village, polio has almost been eradicated. But this is not enough for Zahed’s family. As they prepare for their next vaccination round, they are determined not to stop their work until everyone in their community – wherever they are from – is safe from polio.
With polio at the lowest levels in history in Pakistan, the country has launched a powerful and hopefully final assault on the disease in 2018. A crucial part of this is to further strengthen the ability of the polio programme to detect virus in stool samples, thereby giving clear indications of where and how the virus is moving in areas where populations remain under-immunized.
To support this effort, the Government of Japan announced today that it will provide US$3.2 million for the procurement of equipment to the Regional Reference Laboratory for polio eradication, located in the National Institute of Health in Islamabad.
The funds will help support the purchase of state-of-the-art molecular-biology equipment, allowing the laboratory to significantly enhance and speed up its ability to process and detect poliovirus in environmental and stool samples. This is critical work – in 2017, the Islamabad lab tested 30 000 stool samples and 950 environmental samples from both Pakistan and Afghanistan, helping the programme better identify where the virus is hiding.
The Japanese grant will also be used to replace aging stocks of cold chain materials and other essential equipment needed to be able to accurately identify poliovirus in samples.
Speaking at the ceremony for the signing of the grant, the Federal Minister of National Health Services, Regulations and Coordination in Pakistan, Saira Afzal Tarar said: “The steady support of the Government of Japan and other partners, and the strong partnership have been crucial elements of the programme’s tremendous progress over the past two years. The new grant will help strengthen polio surveillance through adaptation of new technology and contribute towards polio eradication in the country.”
“These funds come at a crucial time in Pakistan’s eradication effort, and are being used in a strategically important manner,” commented Michel Zaffran, Director for Polio Eradication at the World Health Organization. “The country is on the cusp of being polio-free. What we now need is to urgently root out any last remaining spot where the virus might be hiding, and these funds will help strengthen the ability to do just that. Only by finding polio’s last remaining hiding places will we be able to eradicate it once and for all.“
The Government of Japan is a longtime supporter of the Global Polio Eradication Initiative, with contributions to end polio in Pakistan of approximately ¥24 billion (approximately US$ 224 million) since 1996. With only eight cases recorded in the country in 2017 from just a handful of districts – compared to more than 30 000 all over the country just 20 years ago – these additional funds come at a critical time for the country programme as it launches into the final intensified effort to finish the disease once and for all.
The Global Polio Eradication Initiative partners would like to extend their profound gratitude to both the Government of Japan and Pakistan for their collaboration, and for their tremendous support and engagement in the effort to end polio globally.
A bold sign in the camp for internally displaced persons makes it clear where people can come to be vaccinated against yellow fever. WHO/NIGERIA
As he climbs out of his car and walks across to the entrance of Bakassi camp for internally displaced persons in Borno, northern Nigeria, Dr Terna Nomwhange is met by a familiar sight. Standing at the gates, greeting a tired, dusty family laden with possessions, is a team of polio vaccinators. As families arrive at this sea of shelters following a long, hard journey, these people offering polio vaccines are the first sign that they have reached a place of protection.
Not only are families in northern Nigeria facing insecurity, a humanitarian crisis and the threat of polio, but since September they have also been at risk from an outbreak of yellow fever. By early January 2018, a total of 358 suspected cases had been reported in 16 states, with 45 deaths recorded for 2017. In Borno, the ongoing conflict means that the health infrastructure on the ground to respond to the outbreak is limited to local government and the polio eradication infrastructure.
At the camp gates, the polio vaccinators give two drops of vaccine into the mouth of every child; but they also tell the parents where to go to get their yellow fever vaccination. As Dr Terna, who works for the WHO Nigeria polio eradication programme, walks further into the camp, he catches sight of the distinctive blue that signifies the uniform of a polio volunteer community mobilizer. As she emerges from the door of a shelter, he hears her reminding the family within to get their children vaccinated against polio, but also for the whole family to be vaccinated against yellow fever.
With weakened health system in parts of north eastern northern Nigeria, the infrastructure that is already on the ground to stop polio is providing the volunteers needed to support the yellow fever vaccination campaign. More than eight million people are being targeted with yellow fever vaccines in the states of Borno, Zamfara Kwara and Kogi states in 2018.
Vaccinating adults
By providing both polio and yellow fever vaccinations, the polio infrastructure protects everyone – the young children vulnerable to polio, as well as the whole population at risk of yellow fever. WHO/NIGERIA
Regular polio vaccination campaigns reach children under five years of age with polio vaccines, as this age group is the most vulnerable to the virus. But reaching everyone between nine months and 45 years to protect them against yellow fever takes creative thinking. People who would not usually be vaccinated have to be mobilised to come to health clinics where they can receive that one shot of yellow fever vaccine that infers life-long protection.
This is where the polio infrastructure comes in. To prepare for the launch of the yellow fever vaccination campaign that took place at the beginning of February, polio experts supported the preparations by developing detailed microplans, mapping each community so that every individual can be vaccinated. Volunteer community mobilisers, well versed in educating communities about the risks of infection, used their skills to warn populations of the high mortality rates associated with yellow fever.
Surveillance
Volunteer community mobilizers for the polio programme spread awareness of the importance of polio and yellow fever vaccinations. WHO/NIGERIA
The polio surveillance system in Borno is already on high alert to identify any case of polio, even in conflict affected areas. “Surveillance remains everyone’s number one priority,” says Dr Terna. “While the polio infrastructure is doing everything it can to find any trace of polio, it is killing two birds with one stone by keeping an eye out for yellow fever as well. This is a win-win situation to stop both diseases.”
While surveillance focal persons move house to house, they are also raising awareness about the symptoms of yellow fever. When a potential case is found, the polio infrastructure is being used to collect blood samples and transport them to the national laboratory down the reverse cold chain, keeping samples at the correct temperature for testing.
Collaboration
Volunteer community mobilizers for the polio programme spread awareness of the importance of polio and yellow fever vaccinations. WHO/NIGERIA
“What makes this campaign special is not just the fact that the strong polio infrastructure is helping to control other diseases, but also that it underscores what can be achieved with intersectoral collaboration and partnership,” said Dr Wondimagegnehu Alemu, WHO Country Representative to Nigeria. “Without the polio eradication infrastructure, a campaign of this scale would not have been able to take place.”
“Everyone is pulling in one direction – the government, partners and volunteers within communities – to protect any and every vulnerable person against polio and yellow fever,” says Dr Aliyu Shettima, Polio Incident Manager at the Emergency Operations Centre (EOC) in Maiduguri.
Support for immunization to the Federal Government of Nigeria through the World Health Organization is made possible by funding from the Bill & Melinda Gates Foundation (BMGF), Department for International Development (DFID), European Union (EU), Gavi, the Vaccine Alliance, Global Affairs Canada (GAC), Government of Germany through KfW Bank, Japan International Cooperation Agency (JICA), Korea Foundation for International Healthcare (KOFIH), Measles and Rubella Initiative (M&RI) through United Nations Foundation (UNF), Rotary International, United States Agency for International Development (USAID), United States Centers for Disease Control and Prevention (CDC) and World Bank.
Vaccinating every child, every time Haroon, 3, was vaccinated for the second time in two weeks. WHO / Tuuli Hongisto
In Afghanistan, frontline health workers explain to parents why the polio vaccine must be delivered multiple times
“It’s easy for the others, they are young and strong!” laughs Hamida. She has just climbed hundreds of steps to the top of a long and steep staircase on the side of one of Kabul’s many hills. Together with her colleagues Mohib and Khalid she works as a part of a polio team vaccinating children in their community. Today, the team started at 8 am, and they have now been walking up and down the hill for three hours. No wonder she is tired.
So far, the group has visited 50 families and vaccinated 110 children. They have 30 more to go today, and, in the next three days, they will visit a total of 233.
The team’s role is not only to vaccinate the children but to also to educate people about the life-saving polio vaccine and its importance. It is not always an easy job.
“Last time we visited was only two weeks ago, so some parents have been asking why we are visiting again. I have explained to everyone that the vaccine is beneficial for the children and that children need to be vaccinated every time we visit to be protected.”
It is the first day of a vaccination campaign, which aims to immunize over 6 million children against polio in Afghanistan.
Today, thankfully, all families have accepted the vaccine from this team.
Last push to eradicate polio in Afghanistan
Afghanistan is one of the last countries in the world where wild poliovirus still circulates, and has the highest number of children paralyzed by the virus.
In 2017, there were a total of 14 cases and, so far in 2018, there have been three confirmed cases. In recent months, the virus has been found circulating in southern and eastern regions.
WHO Afghanistan polio programme manager Dr Hemant Shukla is confident that with stepped-up efforts, the circulation can be stopped. “Afghanistan has stopped transmission in the past in all areas, but not at the same time. We are confident that by following correct strategies, focusing in the right areas and by coordinating our efforts with neighbouring Pakistan, we can stop the transmission”.
To answer to the challenge, the Polio Eradication Initiative has stepped up efforts to detect any viruses in the environment. The programme is taking special steps in the eastern and southern regions to reach all children with the vaccine every time the vaccinators pass by, as these are very high risk areas for polio transmission, with people moving in and out of neighbouring Pakistan. Special outreach tactics are concurrently aiming to reach and immunize ‘mobile populations’, such as nomadic people, who are at high risk of contracting polio.
The oral polio vaccine is effective as it not only protects children from contracting the virus, it also prevents them from carrying it in their intestines. Several doses – spaced apart – need to be given to build sufficient immunity, especially in areas where poor nutrition can weaken immune systems.
During the low transmission season, the Polio Eradication Initiative conducted two campaigns – in January and February – in order to vaccinate children in high risk and very high risk districts in quick succession so that the vaccine would have a maximum effect.
In March, 10 million children across the whole country will be vaccinated – that’s every single child under the age of five years.
In Kabul, one by one the team marks their tally sheet with numbers and ages of the children and takes note whether all the children of the household were present.
One of the children vaccinated today is three-year-old Haroon, who stands outside his family’s home. His mother Nadia peeks through the gate. She has six children, and Haroon is her youngest.
“Haroon was just vaccinated two weeks ago, but I know it is important to vaccinate children every time”.
The team marks this household vaccinated for today.
In four weeks, Nadia will open up her door when the vaccinators knock again.
The Afghanistan polio snapshot gives a monthly update on key information and activities of the polio eradication initiative in Afghanistan.
In January:
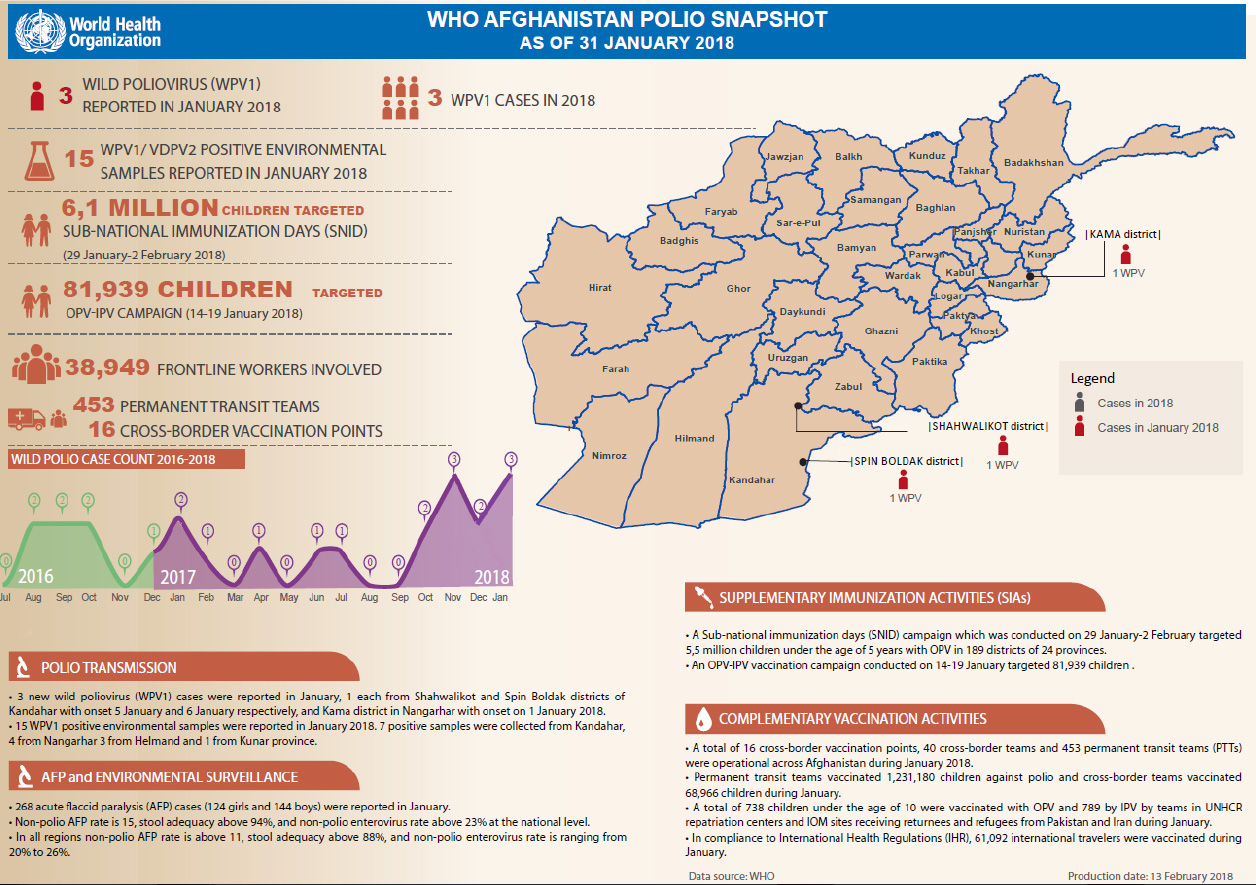
Three new cases of wild poliovirus (WPV1) were detected, two from Kandahar province, and one from Nangarhar province.
6.1 million children under five years of age were targeted during subnational immunization days across 24 provinces.
Permanent transit teams successfully vaccinated 1 231 180 children against polio, whilst cross-border teams vaccinated 68 966 children.