The 72nd World Health Assembly, the governing body of the World Health Organization held by in Geneva, Switzerland is the biggest congregation of public health actors. Taking advantage of the critical mass of global leaders, the Global Polio Eradication Initiative hosted an event for polio eradicators, partners and stakeholders on 21 May 2019.
The event, To Succeed by 2023—Reaching Every Last Child, celebrated the GPEI’s new Polio Endgame Strategy 2019-2023. The five-year plan spells out the tactics and tools to wipe out the poliovirus from its last remaining reservoirs, including innovative strategies to vaccinate hard-to-reach children and expanded partnerships with the Expanded Programme on Immunization (EPI) community and health emergencies.
The informal event brought together a cross-section of stakeholders – partners, health actors, non-health actors, supporters, donors, Ministers of Health of endemic countries, WHO Regional Director for the Eastern Mediterranean, and Polio Oversight Board members – alluding to strengthened and systematic collaboration in areas of management, research and financing activities in the last mile.

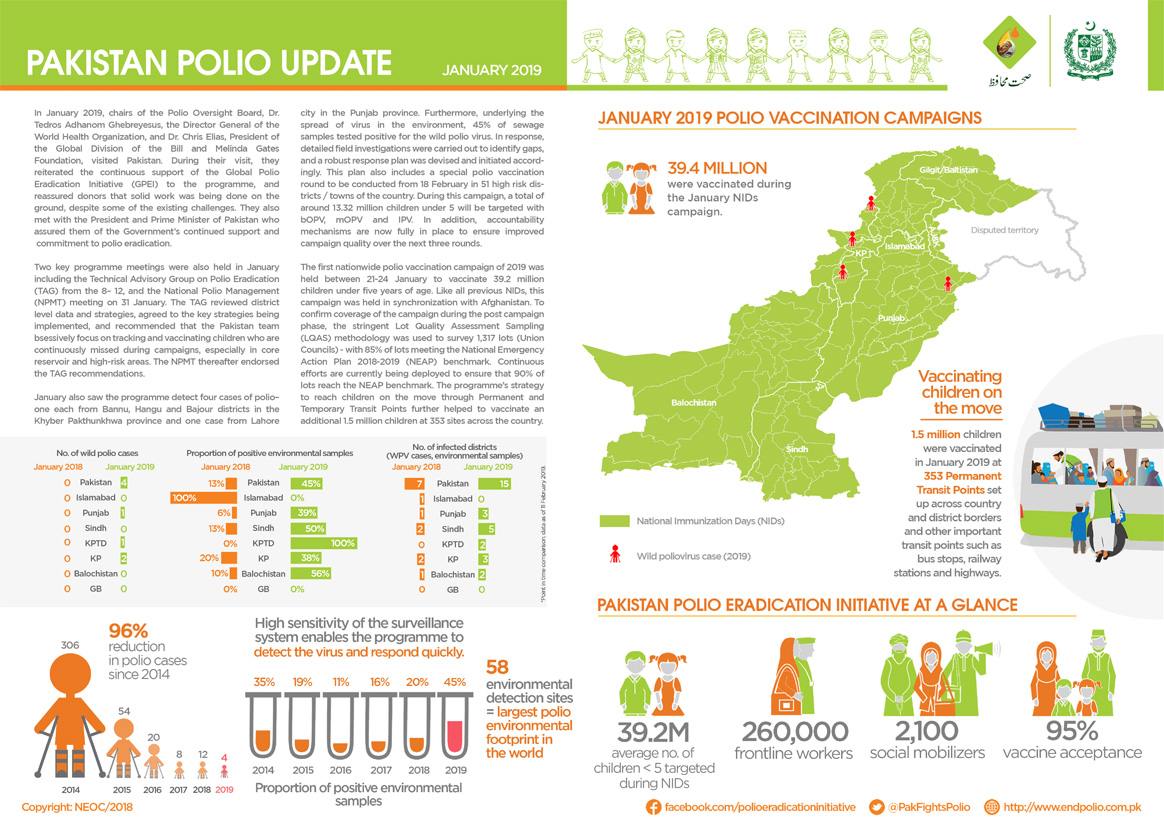
Dr Zafar Mirza, Pakistan’s Minister of State,Ministry of National Health Services, Regulations and Coordination, took the stage and gave insight into country-level polio eradication efforts and the need for coordinated action with Afghanistan: “20 years ago, 30 000 children were paralyzed by polio in Pakistan. This year, 15 cases have been reported. While we have done a lot, it is clearly not enough. We are resolute in this conviction. We, together with Afghanistan, must make sure we eradicate polio for the sake of our children. Our science is complete, only our efforts are lacking. Along with the polio programme, the donors and the Afghan government, we will get to the finish line.”
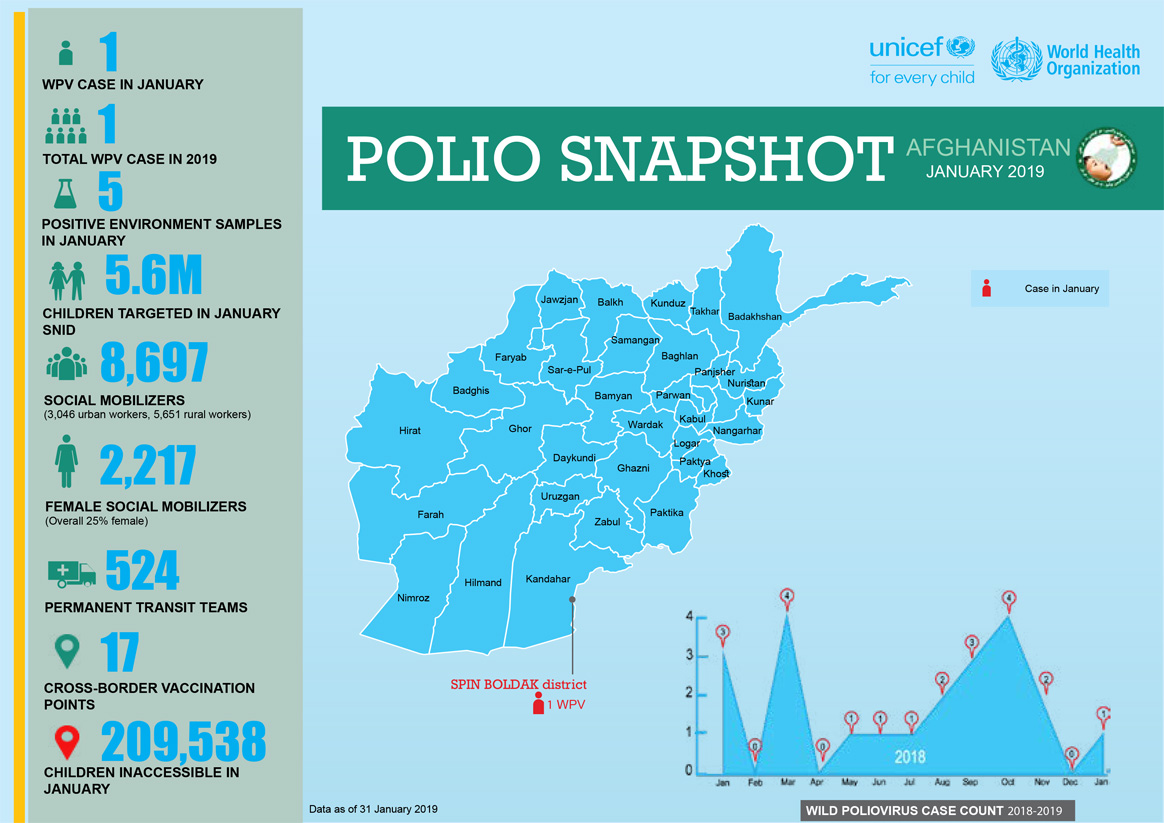
Echoing similar sentiments, Dr Ferozuddin Feroz, Minister of Public Health of Afghanistan, said, “I would like to start by expressing thanks to all the partners for their support. As you know, Afghanistan has a very challenging context due to inaccessibility, refusals, gaps in campaign quality, low routine immunization coverage, and extensive cross-border movement. But, Afghanistan has made progress—five out of seven regions continue to maintain immunization activities. We view polio as a neutral issue and have developed a robust National Emergency Action Plan 2019. We appreciate the Polio Endgame Strategy 2019-2023. We believe coordination with Pakistan will help us deliver a polio-free world. We look forward to your continued technical and financial support to achieve the goal of polio eradication.”

Recognizing the long-standing commitment of the United Arab Emirates, a video was played showing the on-ground efforts of the Emirates Polio Campaign, working with communities and families in Pakistan in collaboration with the Global Polio Eradication Initiative and partners, and the Government of Pakistan. Thanks to the Emirates Polio Campaign, 71 million Pakistani children have been reached with 410 million doses of polio vaccine.
Dr Abdullahi Garba, Director for Planning, Research and Statistics, National Primary Healthcare Development Agency spoke on behalf of Professor Isaac F Adewole, Federal Minister of Health of Nigeria. Dr Garba harked back to the past as the GPEI plans for the future: “Nigeria started actively working to eradicate polio in 1988, at a time when we used to have up to a thousand cases every year. With all our innovation and efforts, I am pleased to inform you today that no wild polio case has been detected for the past 33 months. This feat was achieved through continuous efforts between the government, GPEI and partners, having diligent incidence reporting, reaching inaccessible children, and improving the quality of the polio surveillance immunization activities through strong oversight mechanisms in Nigeria. I know I also speak on behalf of all countries across Africa – we will achieve success.”

Rounding off the evening, Dr Tedros Adhanom Ghebreyesus, the World Health Organization Director-General and Chair of the GPEI Polio Oversight Board, took the stage to recount his first visit of the year to the polio endemic countries of Afghanistan and Pakistan, the progress made over decades, and the need to re-commit to the cause of ending polio. “Together with Regional Director Ahmed Al-Mandhari and Chris Elias of the Gates Foundation, we travelled to Pakistan and Afghanistan. We saw first-hand the commitments by both public and civil society leaders, which gave us a lot of confidence. The other thing that gave us confidence was seeing our brave health workers trudging through deep snow. And of course, our partners: Rotary, United Arab Emirates, CDC, UNICEF, the Bill & Melinda Gates Foundation and Gavi. The last 30 years have brought us to the threshold of being polio-free…(which) lay out the roadmap that is the Polio Endgame Strategy 2019-2023. The Ministers of Afghanistan and Pakistan have also assured us that they will continue to work together in their shared corridor to finish polio once and for all.”

In 1988, the World Health Assembly passed a resolution to globally eradicate poliovirus, in what was meant to be “an appropriate gift…from the twentieth to the twenty-first century.”
As the GPEI plans for the future and its final push to ‘finish the job,’ it is clear that political and financial efforts need to ramp up in this increasingly steep last mile. As he concluded, Dr Tedros thanked committed partners like United Arab Emirates: “Global progress to end polio would not be possible without partners like the UAE. I would like to thank His Highness Sheikh Mohamed bin Zayed Al Nahyan, Crown Prince of Abu Dhabi, and the UAE – a long-time supporter of the polio programme – for agreeing to host the GPEI pledging event this November at the Reaching the Last Mile Forum, a gathering of leaders from across the global health space held once every two years…let us join together to end polio.”