As Pakistan continues to struggle from the effects of the devastating floods affecting parts of the country, polio staff on the ground continue to assist emergency relief efforts.
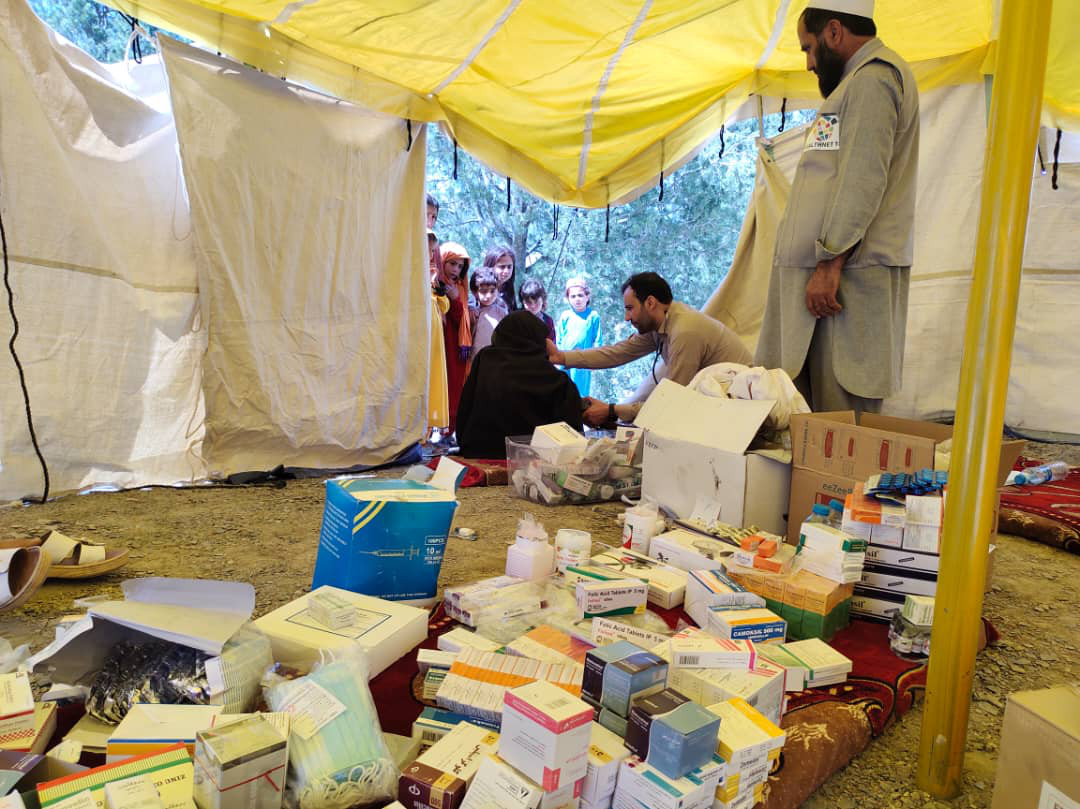
In flood-affected districts, the polio effort is supporting establishment of critical health camps, to provide basic clinical services, particularly ensuring treatment of water-borne and vector-borne diseases, and distributing water purification tablets. All routine immunization antigens are also provided to target children and pregnant women. Staff are actively conducting surveillance for communicable diseases, identifying nutrition needs of displaced populations, and collecting and analysing life-saving data to help target response strategies. Polio programmes around the world have a long history of supporting broader public health and humanitarian emergencies, as was the situation earlier this year in Afghanistan, following the devasting earthquake there.
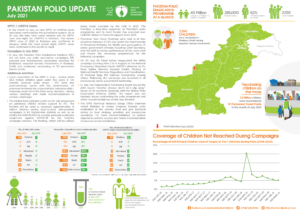
At the same time, the polio programme is adapting its operations, to ensure polio eradication efforts can continue unabated, even amid the tragedy. The programme is at a critical juncture – intensive response is ongoing to stop this year’s outbreak in southern Khyber Pakhtunkhwa. Virus linked to this outbreak was this month detected in an environmental sample from Karachi, in the south of the country. At the same time, the high transmission season for polio transmission is now starting and this transmission risks being particularly intense given the floods.
But despite these challenges, polio staff are working double-time: adapting polio approaches, while supporting life-saving flood relief efforts.
“I have been fortunate enough to be present when a number of countries successfully eradicated polio,” commented Dr Hamid Jafari, Director for Polio Eradication at the World Health Organization’s Regional Office for the Eastern Mediterranean. “Rarely have I seen such commitment and dedication than I have seen in Pakistan – from national political leaders, to health workers, right to the mother and father on the ground. To all who are involved, all I can say is: Thank you! You are making a huge difference to people’s lives, which goes far beyond the effort to eradicate polio.”
While detection of virus in Karachi is not unexpected, given the large-scale and frequent population movements between Karachi and the rest of the country, in particular Khyber Pakhtunkhwa. urgent efforts are underway, coordinated by the national and provincial Emergency Operations Centres (NEOC and PEOC), to continue surveillance efforts in greater Karachi and further boost immunity levels through health camps, to prevent polio from establishing a foothold in Pakistan’s largest city which has historically been a major polio reservoir.
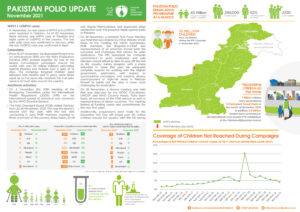
Despite the extraordinary climatic conditions and consequent operational challenges aggravated by the collapse of infrastructure, the programme continued with the August polio campaign – including across Karachi – and re-adjusted the schedule in all accessible areas. While the immunization campaign could not be conducted in Balochistan and parts of Sindh, the effort managed to reach nearly 32 million children in the country, with health workers wading through deep water to reach children with the life-saving vaccine.
At the same time, the programme has undertaken contingency planning to resume intensified vaccination activities in southern Khyber Pakhtunkhwa to stop the outbreak, as soon as the situation allows. The programme continues to innovate, adapt, and find opportunities to build children’s immunity through vaccination at health camps, at transit points, in settlements for displaced persons.
And, of course, national and subnational authorities are coordinating activities with neighbouring Afghanistan, particularly in border regions, given that both countries represent a single epidemiological block. Confirmation this month of Afghanistan’s second case this year, from Kunar province, confirms the risk any residual transmission on either side of the border continues to pose to children across this block.
Kunar, along with the rest of the country’s Eastern Region, is part of one of three, critical cross-border epidemiological corridors with Pakistan, the northern corridor specifically comprising of Eastern Region and central Khyber Pakhtunkhwa in Pakistan. Case response is currently being planned in the immediate area and the broader corridor. The other two cross-border epidemiological corridors are the southern corridor, comprising Quetta Block of Pakistan and Southern Region, Afghanistan; and, the central corridor, comprising southern Khyber Pakhtunkhwa and South-East Region in Afghanistan.
Districts along the border of Pakistan and Afghanistan in the three epidemiological corridors are at high-risk for poliovirus transmission, given the high proportion of zero-dose children and inconsistent quality of polio vaccination campaigns in some areas.
The Pakistan and Afghanistan polio programmes continue to coordinate on surveillance and vaccination activities through the Global Polio Eradication Initiative Support Hub, based in Amman, Jordan.