Elkoz Station (Wastewater station), Khartoum, Sudan. Jan 10, 2021: environmental surveillance collectors pouring wastewater for testing.
The Global Commission for the Certification of Poliomyelitis Eradication (GCC) met recently in Amman, Jordan, to review progress towards interrupting wild poliovirus type 1 (WPV1) transmission in polio-endemic Pakistan and Afghanistan, implementation of the Global Surveillance Action Plan, and to hear from the six regional certification commissions on current regional priorities and issues.
‘Deep-dive’ sessions on both endemic countries, focusing on epidemiology, virology, immunization coverage and surveillance, were valuable opportunities for the global body to be updated on current challenges being faced by Pakistan and Afghanistan country teams in achieving zero polio. The GCC commended the national programmes for their conduct of high-quality activities in the face of political instability, insecurity and other operational barriers, and concluded that 2023 presents a vital opportunity to finally stop transmission of WPV1.
On detection of poliovirus, the GCC noted the progress towards implementation of the GPEI Global Surveillance Action Plan (GPSAP) but raised concerns over shortcomings in surveillance performance, particularly the timeliness of detection and quality of environmental surveillance in some localities. The Commission reiterated the importance of environmental surveillance as a supplement to AFP surveillance, and while recognizing that its utility varies depending on ground realities, recommended that further analysis be conducted into ES system performance and for updates to be provided to the group on a biannual basis.
More broadly, the GCC stressed a need for greater confidence in surveillance systems worldwide, and particularly in the endemic countries, to detect transmission within areas and populations of greatest risk, such as those with substantial gaps in population immunity, high risk mobile groups and areas that have had silent transmission of poliovirus. The GCC called for greater granularity in GPEI reporting of progress in implementing the GPSAP and flagged a need for deeper understanding of all potential gaps, including region specific issues.
“It will be the quality of poliovirus surveillance that will allow the GCC to certify the eradication of WPV1 with the highest possible level of confidence,” said Professor David Salisbury, GCC Chair.
The GCC also recommended that immune-deficient vaccine-derived poliovirus (iVDPV) surveillance continue to be developed as an important aspect of the validation of the absence of VDPV.
Lastly, the GCC commended GPEI’s continued and intensive coordination and support of the endemic country programmes, to facilitate a smooth regional certification process when WPV1 is no longer detected and recommended that polio-free regions begin to prepare for global certification of WPV1, in line with the Eastern Mediterranean’s regional certification.
The full GCC report and recommendations will be made available in the coming weeks.
Following wide engagement of stakeholders – from lab workers to engineers to certification bodies responsible for signing off on the lockdown of poliovirus strains after certification of eradication – WHO’s chief guidance document for poliovirus containment has been given an overhaul. The update to the WHO Global Action Plan for Poliovirus Containment (GAP-IV, previously GAP-III) comes at the request of the WHO Containment Advisory Group (CAG) and streamlines the tool with other relevant WHO guidance and technical recommendations made by CAG. Its availability is expected to help accelerate containment implementation worldwide.
Containment involves biosafety and biosecurity requirements for laboratories and vaccine production sites, or any other place handling and storing eradicated polioviruses, to minimize the risk of these pathogens being released into communities. It also concerns risk mitigation measures associated with field use of some live oral polio vaccines. WHO urges facilities holding virus to move through its Containment Certification Scheme, and follow guidance contained in GAP-IV.
“Retention of poliovirus materials for what their governments deem to be critical functions is a risk and responsibility for all countries that choose to do so,” said Prof David Heymann, Chair of the CAG and professor of infectious disease epidemiology at the London School of Hygiene and Tropical Medicine. “GAP provides guidance that aims to minimize the risk of escape of the poliovirus from a retention facility, and we hope that the revised publication ̶ which stakeholders in polio eradication helped shape ̶ will ensure faster action by countries that decide to retain poliovirus materials,” he said.
“The revision of the guidance has been a long time in the making and comes with a lot of anticipation,” stated Dr Harpal Singh, WHO polio technical officer and CAG secretariat. “WHO and CAG have taken on board the numerous concerns and feedback from Member States with regards to carrying out the guidance, and a certain degree of flexibility based on local risk mitigation measures has been applied in some areas, whilst maintaining the rigor of evidence-based best practice,” he added. “We anticipate that this will result in a better implementation of the requirements for Member States opting to retain [poliovirus] materials, and having their facilities certified,” he added.
To date, two of three strains of wild poliovirus have been declared globally eradicated – type 2 and type 3. Countries around the world, however, continue to handle and store these viruses for functions including polio vaccine manufacture, diagnostics and research, among others. It is essential that any facility holding poliovirus types 2 and/or wild or VDPV type 3 stocks, regardless of purpose, either put in place the necessary biorisk management measures outlined in GAP or destroy their virus stocks.
“The world is on the precipice of eradication of wild poliovirus type 1 with the lowest ever case count recorded in 2021, and we got rid of WPV2 and WPV3 in 2015 and 2019, respectively. While some progress has been made, we’re actually quite behind schedule in ensuring those two eradicated serotypes are properly contained, and more needs to be done in this regard,” said Aidan O’Leary, head of WHO’s polio eradication programme.
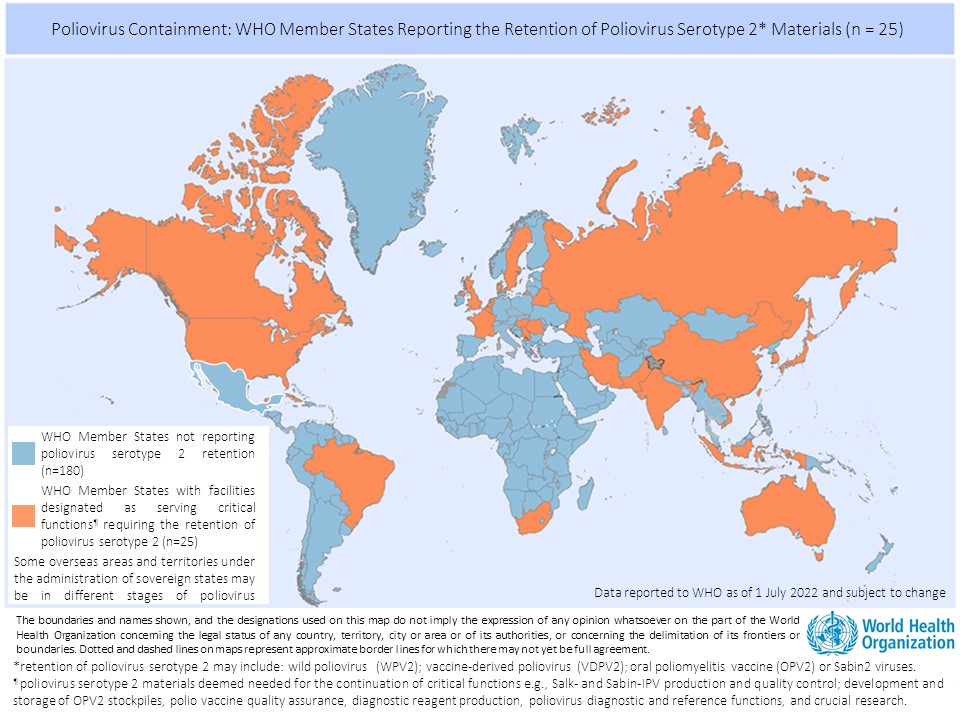
There are currently 25 countries hosting 65 facilities officially designated by their respective governments to retain poliovirus materials. The majority of countries have established a National Authority for Containment for domestic oversight over containment action, in line with commitments from the 2018 resolution, and work is underway to progress their facilities through the Containment Certification Scheme.
For now, containment measures apply to all type 2 and wild and vaccine-derived type 3 materials.
Q: Outbreaks of circulating Vaccine-Derived Poliovirus type 2 (cVDPV2) are popping up in a lot of countries. How do you explain this? Did the programme know this would happen after the oral polio vaccine ‘switch’?
There have been 47 cVDPV2 outbreaks in 20 countries since the switch in April 2016. Some of these outbreaks are spreading over more than one country. Taking the three years before the switch as a frame of reference, there were 8 cVDPV2 outbreaks in five countries altogether in 2013, 2014 and 2015.
Based on epidemiological modelling studies, we anticipated cVDPV2 outbreaks following the removal of the type 2 component from oral polio vaccine in 2016, via the trivalent to bivalent OPV “switch”. And we anticipated that VDPV cases would outnumber wild poliovirus cases in the endgame. However, what the modelling did not predict was the number and scale of these outbreaks, some of which have proven very difficult to stop.
The reason we are seeing a growing number of cVDPV2 outbreaks, particularly in Africa, is the result of a growing cohort of children without mucosal immunity to type 2 poliovirus, while at the same time the [polio] programme uses monovalent oral polio vaccine type 2 (mOPV2) to respond to existing cVDPV2 outbreaks.
The monovalent vaccine [mOPV2] is currently our only tool to interrupt transmission of cVDPV2 and it is very effective when there is sufficient vaccination coverage in the communities we are targeting to avoid an outbreak. However, when campaign quality is poor and not enough children are reached with the vaccine, we run a risk of seeding new viruses among under-immunized populations. There has been evidence of this happening in and outside of outbreak response zones. We are currently developing a new strategy for stopping cVDPV2 outbreaks, and at the same time preventing new outbreaks.
Q: With a limited global stockpile of mOPV2, is there sufficient vaccine to respond to these and future outbreaks?
No. Current mOPV2 stock is insufficient to cater for the number of outbreaks and the sizes of populations requiring it. The GPEI is working with vaccine manufacturers to boost production of mOPV2 and we expect to meet targeted quantities in 2020.
The vaccine will continue to be used for cVDPV2 outbreak response until a new and more genetically stable oral polio vaccine, known as novel oral polio vaccine type 2 (nOPV2), currently under clinical development, is available.
Q. What does increased production of mOPV2 mean for vaccine manufacturers in terms of containment? On one hand, the polio programme is asking for more live type 2-containing OPV. And on the other, it’s pushing for strict containment of all type 2 wild and Sabin polioviruses.
It’s a balance. The world needs enough mOPV2 stocks to help with the elimination of cVDPV2, and type 2 live attenuated poliovirus is needed to produce this vaccine. Yes, we are asking vaccine manufacturers to make more vaccine, but [vaccine] production and containment of type 2 virus are not mutually exclusive pursuits. Polio vaccine manufacture is costly, particularly when demand calls for rapid scale-up of outputs. Containment is also costly. But this is not a reason to put it on hold and stop efforts to ensure safe and secure handling and storage of virus. Quite the opposite: the impetus for putting in place adequate biorisk management systems should be greater, given the higher level of risk of human exposure to poliovirus in and around these facilities.
Q. What about manufacturers of inactivated polio vaccine (IPV)? Can they afford to relax?
IPV is made with killed, or inactivated strains of wild poliovirus types 1, 2 and 3, or their Sabin counterparts. Any facility manufacturing polio vaccines using the type 2 serotype – be it wild or Sabin ̶ and type 3 wild poliovirus since the declaration of its global eradication in October, is required to implement containment measures set out by WHO. This of course also applies to any other type of facilities holding the viruses, for example, research or diagnostic labs.
Holding on to these viruses is a risk and responsibility, and appropriate measures must be taken to protect communities from reintroduction and resurgence.
The world needs IPV and will continue to need it for the foreseeable future. We need vaccine production to continue in well-managed facilities that incorporate GAPIII approaches to biorisk management.
Q. of Sabin 2 remains a priority, while simultaneously, mOPV2 made up of Sabin 2 is being used in countries around the world. What gives?
First, we must be clear that use of mOPV2 is not a decision that is taken lightly. A thorough risk-benefit analysis is conducted before an advisory committee makes a recommendation and it is submitted to the Director-General of WHO for his approval.
It is never ideal to use mOPV2 and reintroduce Sabin 2, which should be under containment. However, as I mentioned earlier, mOPV2 is currently the only tool available to stop outbreaks of cVDPV2 and we must use it.
The reason we continue to push for containment of Sabin 2 viruses in countries not experiencing cVDPV2 outbreaks is precisely to prevent further emergences of VDPV2, which can cause outbreaks of cVDPV2 more easily now because of the very low population mucosal immunity to type 2 poliovirus.
Q. sounds like we are fighting fire with fire with mOPV2. Are we?
Many outbreaks have been stopped using mOPV2. However, in areas with low routine vaccination coverage, and thus low immunity, we are indeed reintroducing Sabin 2 in naïve populations and seeding new outbreaks. We are currently reviewing all aspects of our cVDPV2 approach and developing a new strategy that examines all options and tools ensuring we are using each for full impact. This includes improving our outbreak response so that it is appropriate in scope and effective, and accelerating the development and roll-out of a new vaccine that is less likely to seed outbreaks.
Q: When will nOPV2 be available?
Clinical trials are underway. There are numerous influencing factors but if all goes according to plan, our estimate is that approximately 100 million doses of the vaccine could be ready by mid-2020, with another 100 million by the end of the year. We are also working with the WHO prequalification team, which independently reviews all vaccine data to ensure a consistent quality in accordance with international standards to enable the vaccine to be used as quickly as possible by affected countries under an Emergency Use Listing (EUL), a risk-based procedure for assessing vaccines for use during public health emergencies—such as polio.
The vaccine is also being developed for types 1 and 3 polioviruses; however, this is further away in terms of production.
24 October 2019 – In a historic announcement on World Polio Day, an independent commission of experts concluded that wild poliovirus type 3 (WPV3) has been eradicated worldwide. Following the eradication of smallpox and wild poliovirus type 2, this news represents a historic achievement for humanity.
“The achievement of polio eradication will be a milestone for global health. Commitment from partners and countries, coupled with innovation, means of the three wild polio serotypes, only type one remains,” said Dr Tedros Adhanom Ghebreyesus, Director-General of the World Health Organization and Chair of the Global Polio Eradication Initiative (GPEI) Polio Oversight Board “We remain fully committed to ensuring that all necessary resources are made available to eradicate all poliovirus strains. We urge all our other stakeholders and partners to also stay the course until final success is achieved,” he added.
There are three individual and immunologically-distinct wild poliovirus strains: wild poliovirus type 1 (WPV1), wild poliovirus type 2 (WPV2) and wild poliovirus type 3 (WPV3). Symptomatically, all three strains are identical, in that they cause irreversible paralysis or even death. But there are genetic and virologic differences which make these three strains three separate viruses that must each be eradicated individually.
WPV3 is the second strain of the poliovirus to be wiped out, following the certification of the eradication of WPV2 in 2015. The last case of WPV3 was detected in northern Nigeria in 2012. Since then, the strength and reach of the eradication programme’s global surveillance system has been critical to verify that this strain is truly gone. Investments in skilled workers, innovative tools and a global network of laboratories have helped determine that no WPV3 exists anywhere in the world, apart from specimens locked in secure containment.
At a celebration event at the headquarters of the World Health Organization in Geneva, Switzerland, Professor David Salisbury, chair of the independent Global Commission for the Certification of Poliomyelitis Eradication, presented the official certificate of WPV3 eradication to Dr Adhanom Ghebreyesus. “Wild poliovirus type 3 is globally eradicated,” said Professor Salisbury. “This this is a significant achievement that should reinvigorate the eradication process and provides motivation for the final step – the eradication of wild poliovirus type 1. This virus remains in circulation in just two countries: Afghanistan and Pakistan. We cannot stop our efforts now: we must eradicate all remaining strains of all polioviruses. We do have good news from Africa: no wild poliovirus type 1 has been detected anywhere on the continent since 2016 in the face of ever improving surveillance. Although the region is affected by circulating vaccine-derived polioviruses, which must urgently be stopped, it does appear as if the continent is free of all wild polioviruses, a tremendous achievement.”
Eradicating WPV3 proves that a polio-free world is achievable. Key to success will be the ongoing commitment of the international development community. To this effect, as part of a Global Health Week in Abu Dhabi, United Arab Emirates, in November 2019, the Reaching the Last Mile Forum will focus international attention on eradication of the world’s deadliest diseases and provide an opportunity for world leaders and civil society organizations, notably Rotary International which is at the origin of this effort, to contribute to the last mile of polio eradication. The GPEI 2019–2023 Investment Case lays out the impact of investing in polio eradication. The polio eradication efforts have saved the world more than US$27 billion in health costs since 1988. A sustained polio-free world will generate further US$14 billion in savings by 2050, compared to the cost countries would incur for controlling the virus indefinitely.
On the long road to global polio eradication, the programme has achieved four important milestones, representing four out of six WHO regions that have been certified as having interrupted transmission of wild poliovirus (WPVs): Region of the Americas (1994), the Western Pacific Region (2000), the European Region (2002), and the South-East Asia Region (2014).
At present, only the Eastern Mediterranean and African regions— no WPV reported in Africa since 2016, the African region may be eligible for regional certification as early as late 2019—remain to be certified in the path towards global eradication and hence constitute a key priority.
But who decides that a region is free of WPV?
The Eastern Mediterranean Regional Commission for Certification of Poliomyelitis Eradication (ERCC) is an independent body appointed in 1995 by the WHO Regional Director for Eastern Mediterranean to oversee the certification and containment processes in the region. It is the only body with the power to certify the Region free from wild polio, which convenes annually. Here are the outcomes of the recent ERCC meeting:
Urgent need to address regional priorities
The Commission noted with concern the need to stop the ongoing wild poliovirus type 1 transmission in the only two remaining polio-endemic countries in the Region: Afghanistan and Pakistan. The RCC acknowledged the on-going eradication efforts but strongly recommended the full implementation of the respective national emergency polio programmes through complete political and programmatic support to tackle the WPV1 transmission in the common Pak-Afghan epidemiological corridor, which remains unabated. The Commission also expressed concern about the current circulating vaccine-derived poliovirus type 2 and 3 transmissions in Somalia.
Wild poliovirus type 3certification prospects
The Commission, however, marked the good progress made towards curbing wild poliovirus type 3 (WPV3). Extensive analyses of the stool and environmental surveillance samples provided evidence that no WPV3 is in transmission in the Region. Based on the epidemiology, EMRO – along with the rest of the world – may be up for global WPV3-free certification by the GCC, potentially certifying two of three poliovirus strains eradicated—WPV2 strain was certified as globally eradicated in 2015.
Stepping-up is the need of the hour
So far, sixty cases of WPV1 are reported from two countries (Pakistan and Afghanistan) in 2019. Given the existing WPV1 transmission in the two remaining endemic countries of the Region, the RCC asked that the Member States undertake a firm commitment necessary for reaching zero.
Eastern Mediterranean Regional Commission for Certification of Polio Eradication (ERCC)
The Thirty-third meeting of the EMRO RCC was held in Muscat, Oman, to discuss the Regional progress towards a polio-free certification. The meeting brought together members of the RCC, chairpersons of the National Certification Committees, polio programme representatives of 21 countries, and WHO staff from the headquarters, regional, and the endemic countries. Representatives from Rotary International and the Centers for Disease Control and Prevention were also in attendance.
Comprised of public health and scientific experts, the regional certification commissions are independent of the WHO and national polio programmes. Global certification will follow the successful certification of all six WHO regions and will be conducted by the Global Certification Committee (GCC).
Last month, we spoke with head of the Containment Advisory Group Professor David Heymann about some of the similarities and differences between poliovirus and smallpox containment, and work of the CAG. With decades of public health experience David has worked to manage and curb the spread of SARS, Ebola, Zika virus, HIV, malaria, and measles – and that’s in addition to polio and smallpox eradication efforts! He is currently a professor of Infectious Disease Epidemiology at the London School of Hygiene and Tropical Medicine and head of the Centre on Global Health Security at Chatham House, London.
As part of your extensive experience with infectious diseases you were involved in efforts to eradicate smallpox, a disease which caused the death of more than 300 million people in the 20th century alone. How did you get involved in the effort and what were some of the difficulties faced in reaching eradication?
David Heymann was the former Chair of Public Health England, Assistant Director-General for Health Security and Environment (WHO) and Representative of the Director-General for Polio Eradication (WHO).
For the smallpox programme I was recruited by WHO as a short-term consultant and I spent two years with the programme in the field, in Bihar state, India.
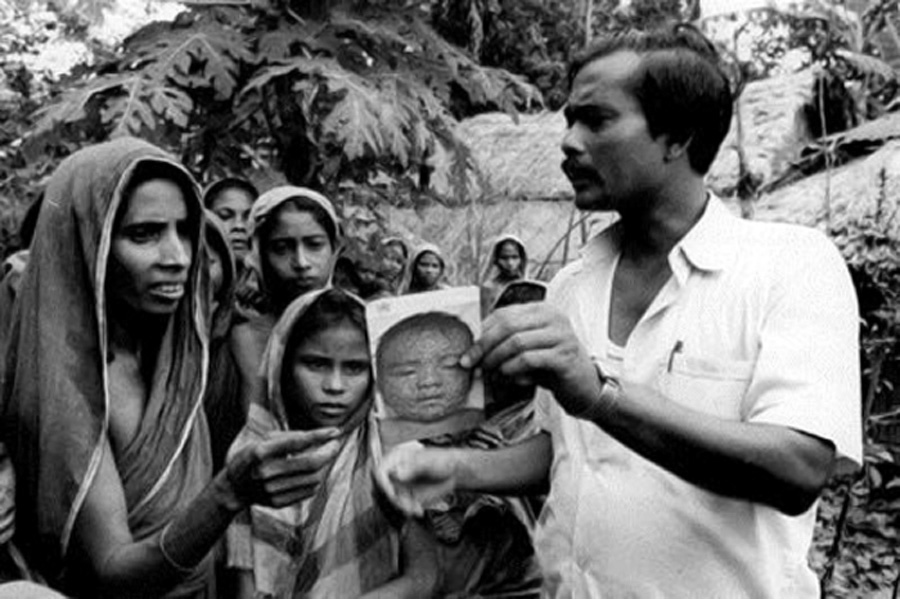
Smallpox eradication was actually very simple to deliver. It was straightforward with two basic strategies: search and contain. The search component involved looking for children or adults showing classical signs of smallpox, by going from house to house, to villages, communities, markets and religious festivals – wherever people congregated. We took with us pictures of what smallpox looked like so people knew what we were looking for and what to be on the lookout for. We explained that our work was to put an end to this disease and relieve pain and suffering, and communities were very receptive.
When a patient was identified, the address was taken and a house visit was made. If diagnosed as smallpox the patient was then isolated and there was a local vaccination activity – a ‘containment activity’ – with residents of 30 households around that patient vaccinated.
Would you say then that eradicating smallpox was/is easier than eradicating polio?
Yes. Compared to polio, smallpox was much easier to eradicate. A major reason being the nature of polio with only 1 out of approximately 200 cases being symptomatic. For smallpox, every infection resulted in the same clinical manifestation of the disease and this made patients easier to find and isolate. It also made following up on [case] contacts easier for monitoring and immediate isolation if they started to show signs of fever.
From a logistics point of view, far less vaccine was needed to stop smallpox transmission as the strategy was not mass immunization but ring vaccination – vaccinating people in households surrounding that of the patient and any other persons who were known to have contact with the patient. The vaccine was heat stable meaning it could be taken anywhere without cold chain. This is not the same for polio vaccine which needs to be kept cold.
Strict laboratory containment of variola virus which causes smallpox is vital to help make sure the disease does not come back. Was this something always known to the programme and was lab containment prioritized at the time of eradication?
The last case of smallpox in nature occurred in 1977 but the last human case actually occurred in 1978 through a laboratory accident in Birmingham, United Kingdom. The accident involved a medical photographer who was in a neighbouring office to the room storing variola virus. She became infected and then infected her family members. It was then realized that so long as the virus was going to be used in laboratories for research, it needed to be used under strict biosecurity conditions.
There was then a recommendation from WHO that countries destroy their variola stocks or transfer them to one of two major laboratories, one in Russia and the other in the US. Some countries destroyed but many asked for their viruses to be transferred and stored. The eradication programme anticipated that the two repository laboratories would eventually destroy virus stocks but that has not occurred because of continued research, which some scientists feel requires live variola virus, to discover new medications, new vaccines and new diagnostic tests for smallpox and other diseases. This research is being overseen by WHO.
It is thought by some that the variola virus may not be in just these two laboratories, but elsewhere around the world; to date it has not been possible to ascertain this with any certainty.
Which of the viruses is more infectious? And what are some of the differences in terms of containment?
The viruses are infectious by different means: variola is infectious via direct droplets, say for example when a patient sneezes, or through contamination by pus from the smallpox lesions. Polio is transmitted fecal-orally. It can get into water systems so it’s much easier to transmit than smallpox and has the potential to be much more widespread.
When we look at containment, things are much more complex for polio. One of the major differences is that the endgame for polio does not anticipate that the [polio] virus will be destroyed almost universally as it was for smallpox. There are 26 countries that want to continue to hold on to poliovirus for research and vaccine manufacture. We’re dealing with not only the wild poliovirus but also live Sabin virus strains found in oral polio vaccine. We’re dealing with infectious and potentially infectious materials. And in addition, the virus has been constructed de novo by a research laboratory. So it’s a very complicated endgame.
Smallpox containment was relatively easy to manage. There was a resolution by WHO to destroy or transfer materials, countries adopted this resolution, and things moved rather quickly.
From what you said, smallpox was completely eradicated before efforts began to securely contain it in labs. Are we not putting the horse before with poliovirus containment?
Type 2 poliovirus has already been eradicated and was certified as such in 2015. Countries need to urgently move on containing their type 2 materials. This is what the GCC, GPEI and CAG are advocating for, and what countries committed to through the World Health Assembly Resolution [on poliovirus containment] in 2018.
Containment for the remaining types 1 and 3 poliovirus will follow after their eradication is confirmed, and countries are urged to complete their inventories for their wild types 1 and 3 materials. It’s looking likely that type 3 will be declared eradicated by the GCC this or early next year and this will have containment implications. So surveys and inventories for wild type 3 materials should be done as soon as possible.
As Chair of the Containment Advisory Group, you advise WHO’s Director-General on poliovirus containment matters. Could you briefly explain how the CAG works and the make-up of the group?
CAG is made up of clinicians, epidemiologists, other public health experts, sanitation engineers and laboratory design experts. It’s made up of a varied group of people in order that they can interpret questions which might come from laboratories planning to retain the virus. Essentially, laboratories are interested in the most cost-beneficial ways of working with and storing the virus and sometimes question some of the recommendations made in WHO’s Global Action Plan III for the containment of polioviruses (GAPIII). CAG reviews and studies these questions and provides its interpretation to the Director-General.
At the time when global certification of eradication of all three types of poliovirus has occurred, there will be two major areas that will be important to scrutinize: 1., making sure country surveys and inventories of poliovirus materials and destruction of unneeded materials have been carried out, and 2., making sure appropriate containment measures have been put in place for facilities that will hold polioviruses. CAG can support this second function, however, the mechanisms would need to be determined by WHO and implemented by countries under a national system of regulation.
Has there been a containment issue that CAG has been unable to resolve?
Yes, an example is the laboratory ‘shower-out’. Showers are recommended for facilities maintaining polioviruses. These include industry that makes vaccine from the virus.
For many laboratories there’s a washing up process, where after you remove or doff your personal protective equipment, you take a shower because then if there are any remnants [of virus] on the skin, you wash it away. But there’s a lack of evidence to show whether that shower is effective, or even if it might be increasing risk [of exposure] by causing aerosolization of what might be virus on the body which could be inhaled. Further to a review of literature on this topic CAG has recommended that a study be done to determine effectiveness of the shower. This is being taken forward by WHO.
Presumably the CAG will continue to play a role after the global certification of eradication of polio, as containment is for the long-term. For how long will CAG be needed?
CAG functions will certainly be needed into the future. How that happens will be up to WHO. WHO will have to make sure that functions are covered by an appropriate technical group.
Finally, what would be your message to WHO Member States that have expressed they want to retain poliovirus but are undecided on if they will stick with this course of action and continue through the containment certification hoops?
My recommendation would be that they thoroughly study the issue and 1., decide why they want to retain the virus, and 2., justify that against the risk that it could escape from a laboratory and reinfect the world with polio, which would be a major public health crisis. They should conduct a risk-benefit analysis. If they believe they can safely keep the virus then they should follow what they believe. But if they cannot with all certainty say that they can keep the virus isolated and secure, they should reconsider.
It’s an issue of global responsibility to make sure that countries have the capacity to store the poliovirus safely if they decide to retain it after global eradication has been certified.
After concerted efforts spanning decades, polio eradication efforts are in the homestretch and experts are advising how to fast-track the last mile.
The SAGE convened in Geneva from 2-4 April 2019 to discuss all things related to vaccines and immunizations, including poliovirus and the global eradication efforts around it. SAGE reviewed the latest global polio epidemiology, the new Global Polio Eradication Endgame Strategy 2019-2023, and what the post-eradication world could look like.
Double down and escalate the fight to end wild poliovirus
While SAGE noted the achievements and the progress of the Global Polio Eradication Initiative—reducing the incidence of polio by 99%, absence of wild polio virus type 3 cases, and evidence of Nigeria being wild poliovirus free for over two years—the group displayed cautious optimism about meeting the timeline set out for global eradication of wild poliovirus.
The remaining challenges to fill vaccination coverage gaps—including restricted access, socio-political challenges, and large mobile populations—complicate the efforts to rid the world of poliovirus. However, the GPEI has developed a clear-cut five- year plan to secure a decisive win, the GPEI Polio Endgame Strategy 2019-2023, developed in broad consultation with stakeholders, including SAGE members.
Inactivated Polio Vaccine (IPV)—progress in roll-out continues
From the public health standpoint, Inactivated Polio Vaccine (IPV) can be used indefinitely even after polio eradication. As of April 2019, all 33 countries which had not yet introduced IPV into their routine immunization activities have now done so.
The projected IPV supply is thought to be sufficient enough for the introduction of a two-dose IPV schedule in all countries by 2022, and to catch-up all children missed due to earlier supply shortages, by 2020/2021.
Guidelines Endorsed
As per SAGE recommendations made in October 2016, GPEI developed guidelines for poliovirus surveillance among persons with primary immunodeficiency. After reviewing the guidelines, the SAGE endorsed the guidelines for implementation in high priority countries.
The meeting report will be published in the WHO Weekly Epidemiological Record by May 2019.
The Strategic Advisory Group of Experts (SAGE) on Immunization was established by the Director-General of the World Health Organization in 1999 to provide guidance on the work of WHO. SAGE is the principal advisory group to WHO for vaccines and immunization. It is charged with advising WHO on overall global policies and strategies, ranging from vaccines and technology, research and development, to delivery of immunization and its linkages with other health interventions. SAGE is concerned not just with childhood vaccines and immunization, but all vaccine-preventable diseases.
On 26-27 February 2019, the Global Commission for Certification of Poliomyelitis Eradication (GCC) met at the World Health Organization (WHO) headquarters in Geneva, Switzerland, to continue its intensified work on global certification criteria for poliomyelitis eradication and poliovirus containment. The work of the GCC is critical to verifying the achievement of a world free of all polioviruses.
The GCC reviewed the latest global epidemiology of all poliovirus transmission, examined remaining challenges such as subnational surveillance and immunity gaps, and evaluated current containment status.
The GCC expressed its concerns over the lack of progress in the interruption of transmission of wild poliovirus type 1 (WPV1) in Pakistan and Afghanistan and the spread of vaccine-derived polioviruses (VDPVs). As expressed in a recently-published letter from the four Chairs of the GPEI’s main global advisory bodies, it is essential that improvement is achieved in both routine immunization services and supplementary immunization activity (SIA) quality. Nevertheless, the GCC is continuing to accelerate its work, including taking into consideration circulating vaccine-derived polioviruses (cVDPVs), which continue to take on added significance as the time extends since the discontinuation of type 2 poliovirus in oral polio vaccine (OPV) with consequent loss of type 2 polio immunity. The GCC is also occupied with the urgent and increasing need for effective containment of polioviruses in laboratories and vaccine manufacturing facilities.
Noting that wild poliovirus type 3 (WPV3) has not been isolated anywhere since November 2012, the GCC re-affirmed its decision to undertake sequential certification of WPV eradication, meaning that WPV3 will be certified as eradicated prior to WPV1. The GCC has requested that the Director-General of WHO ask the Regional Directors of Africa and the Eastern Mediterranean respectively to confirm from their Member States that the last WPV3s in both Regions were identified more than six years ago. The GCC will review these data in conjunction with the final reports from the four Regions that have already been certified. This will permit the GCC to certify the eradication of WPV3.
The GCC noted progress in identifying the interruption of WPV1 transmission in the African Region, which will be eligible for regional certification when the African Regional Certification Commission is convinced of the evidence of absence of wild polioviruses that meets surveillance standards.
The outcomes and recommendations of the GCC will be presented to the WHO Director-General, and if accepted, incorporated into the Global Polio Eradication Initiative Strategic Plan 2019-2023. The full report from the GCC’s meeting will be made available at www.polioeradication.org.
Background:
The members of the GCC are independent of WHO and independent of involvement in national polio vaccination implementation or polio surveillance programmes. WHO Regions are eligible for certification following the absence of WPV from any country in that region from any population source in the presence of certification-standard surveillance. Regional certification is conducted by Regional Certification Commissions (RCCs). Global certification will follow the successful certification of all six WHO regions, and will be conducted by the GCC.
Four WHO regions have been certified as having interrupted transmission of WPVs: Region of the Americas (1994), the Western Pacific Region (2000), the European Region (2002), and the South-East Asia Region (2014).
WPV2 was certified as eradicated in 2015. WPV3 has not been isolated from any source since November 2012, making it eligible to be certified as eradicated. Thirty-three cases of WPV1 were reported from two countries (Pakistan and Afghanistan) in 2018 with 223 WPV1 isolates identified additionally through environmental surveillance. The verification of the elimination of VDPVs will occur after the global cessation of OPV use, which will happen after all remaining WPV strains have been certified as globally eradicated.
(Chair of Western Pacific RCC), Professor Yagoub Al-Mazrou (Chair of Eastern Mediterranean RCC), Professor Mahmudur Rahman (Chair of South-East Asian RCC), Professor David Salisbury (Chair of GCC and Chair of European RCC), Dr Arlene King (Chair of American RCC, and Chair of the GCC Containment Working Group); and, Professor Rose Leke (Chair of African RCC).
As part of its work to keep the world safe from poliovirus, WHO is seeking input on draft guidance for managing human exposure to live polioviruses from poliovirus-essential facilities such as labs and vaccine plants. Countries where polioviruses are kept require this guidance. The guidance document is open for public comment and WHO is particularly seeking feedback from national authorities for containment – the national bodies overseeing work in poliovirus containment – and from others working in public health.
The guidance is aimed primarily at public health workers in countries where there are facilities designated to handle and store polioviruses for vaccine production, diagnostics and key research (poliovirus-essential facilities), and outlines public health measures to be taken in the event of a spill or containment breach.
Could you please provide some background on your labs and the polio-related work carried out there?
SO: CDC’s polio and picornavirus lab is a global specialized laboratory in the WHO Global Polio Laboratory Network. It was set up in the mid-1950s and is US-government funded, with CDC being an agency under the Department of Health and Human Services. Our polio lab is one of the largest out there with approximately 55 staff dedicated to polio. We largely deal with the more complex side of polio diagnostics – sequencing, which is the molecular testing of poliovirus-positive samples to determine genetic connections to other known polioviruses.
We also act as a ‘lab of last resort’ when countries, for whatever reason, are unable to carry out preliminary diagnostic tests on their samples. We’re involved in the development of a new and even safer form of oral polio vaccine, and have a team which looks at population immunity through examining blood samples from communities (serosurveys). Importantly, we also develop and distribute reagent kits for testing samples for polio, to labs across the Network.
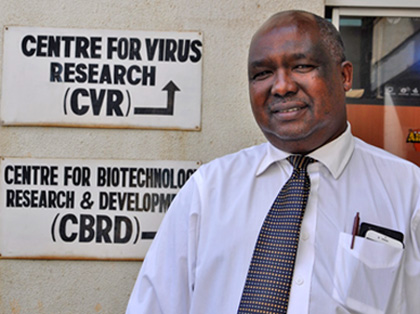
PB: The polio laboratory at KEMRI is combined with the measles and rubella laboratory and has been in operation since the 1980s under the general virology programme. The lab became formally accredited as one of the WHO Global Polio Laboratory Network labs in 2000. Our primary role in relation to polio is supporting surveillance through detection, i.e. isolation of poliovirus from samples we receive. We also conduct intratypic differentiation to identify strains of polioviruses isolated. KEMRI has 12 staff working on polio. WHO funds our routine diagnostic work and supplies and the Kenyan government funds our infrastructure, staff and recurrent costs such as electricity.
What’s the geographic scope of the support you provide?
SO: CDC’s polio lab provides sequencing support to countries around the world. Some examples of countries we are currently assisting include Nigeria, Yemen and those in the Horn of Africa. In terms of serosurveys, we’ve recently done work for Nigeria, DR Congo, Sri Lanka, Ukraine, Pakistan and Lebanon to name a few. We also assisted with testing of samples from Syria during recent polio outbreaks.
PB: We test samples collected from Kenya, Somalia, Djibouti, Eritrea and occasionally from Yemen, for poliovirus. In a year, we would process roughly 4,000 samples and we’ve tested about 200 from Yemen this year. In fact, around 800 samples from Yemen arrived just yesterday. We are in the process of shipping these on to CDC in Atlanta as currently we do not have the capacity to test this quantity. We assist when we can but need to be careful of our capacity so we don’t compromise our support to the other countries.
Type 2 poliovirus (PV2) has been eradicated and WHO has called for countries to destroy unneeded PV2 stocks. However, some will continue to keep PV2 to perform critical functions. Facilities keeping the virus will need to follow GAPIII guidance and pass through a rigorous certification process to prove they can safely and securely handle and store the virus. Their governments are also responsible for putting in place safeguards to minimize risk of containment failure. CDC has decided that it will continue to work with poliovirus but KEMRI has decided to destroy its infectious materials. How were these decisions made?
SO: To do the diagnostics and research work we do, it’s a basic requirement to have a large bank of samples of known identity – PV2 or otherwise. We also need samples to produce our kits, which we distribute to around 120/146 of the Network labs worldwide. CDC has been involved in containment for about 15 years and so understands the GAPIII requirements very well. Most of our facilities meet specifications although a few modifications are needed.
The bulk of the work ahead is related to work practices and documentation ‒ essentially making sure all our i’s are dotted and t’s are crossed. We’re bringing on a containment and safety manager to help with this and with monitoring and training. CDC is also looking closely at its risk assessment models and revising protocols for use in the event of a spill.
PB: Initially, we oriented ourselves to what it means to go through this process and become a poliovirus-essential facility (PEF). We looked at costs; actually the major determinant behind the decision was cost.
The costs of maintaining the infrastructure necessary to remain a poliovirus-essential facility are not tenable as the resource demands are above the government’s capacity. The decision was not from a lab safety aspect. We operate on biosafety level 2 and are a low-risk facility from our own assessments. However, the demands of GAPIII include certain other safeguards.
The primary safeguards that we have here we could easily manage, but the secondary and tertiary safeguards including immunization of the surrounding community and high levels of immunity, the requirement for an effluent system going out of our lab… these are things that made it [becoming a PEF] untenable for us as a country to maintain. In view of the implications of resources versus the benefits, the Kenyan government decided it was not worth KEMRI becoming a PEF.
What were the arguments, if any, for keeping samples at KEMRI?
PB: As any researcher would know, the material is valuable. That was the main argument for retaining. We refer to our stool sample collection as ‘golden stool’ ‒ golden because samples really generate information. When you have isolates, these are useful to share with other facilities on request for vaccine production.
For the unprocessed samples which contain poliovirus, as a research institution, this material is very useful to us for diagnosis of other agents. But when you look at it from the perspective of committing a whole country to putting a lot of resources in [to become a PEF], you say ‘OK, fine’. You let go.
What process did KEMRI follow to destroy its infectious material? And what happens to the new positive samples that come in?
PB: We had a local containment committee in-country who oversaw the destruction activities. We had an inventory and they set a date for us. We removed all our archived wild virus materials from storage and put them in an autoclave. So it was heat deactivation; we incinerated all the materials. KEMRI management and government officials witnessed the process. Because of the large amount of archived materials, it took one full week to prepare and actual destruction took three days. We didn’t want to come back and repeat the process for types 1 and 3 materials and so destroyed all types 1, 2 and 3 wild virus materials at the same time.
For new samples, we archive those positive for types 1 and 3. For type 2, all isolates are sent to CDC for sequencing and original stools are destroyed within 72 hours of the final genomic sequence result.
Having experience with containment, does CDC’s polio lab help others reduce risk of breaches?
SO: We help answer technical questions coming from other facilities in the US looking to contain the virus. Part of preparing to become a PEF is to have emergency plans in place in case there is a spill. We assist facilities in putting together their plans, and can help out with response if there is a spill.
A nation-wide immunization campaign helped in eradicating polio in India. WHO/2011
Eradicating polio in India was a feat of dedication, commitment and simply doubling down on immunization activities. Given India’s vast population, tropical climate in many parts of the country, and other environmental challenges, it would be easy to imagine that if polio couldn’t be stopped, India would be the place to fail.
Simply put: it was a challenge. After all, India constituted over 60% of all global polio cases as recently as 2009.
However, in 2014, India was officially declared polio-free, along with the rest of the South-East Asia Region. Thanks to the singular commitment of the Indian Government at all levels, partners of the Global Polio Eradication Initiative, notably WHO, Rotary International and UNICEF, polio was tackled head-on. India has not had a case single case of wild polio virus since 2011.
India had long been considered one of the most difficult geographical locations to eliminate the disease. Success in India really changed the game, and now serves as an example that eradication of polio is indeed possible when the world marshals political will and commits adequate resources to the cause that affects everybody worldwide.
Today, the world is close to making public health history when it comes to polio – as it was when in 1980 small pox was officially eradicated. The goal of reaching a polio-free world is well within reach.
Tune in to listen to the podcast as the UN Dispatch tells the story of how, against all odds, India wiped out polio, and some of the lessons learned along the way.
28 May 2018, Geneva, Switzerland: ‘Eradicate first’ was the mantra at last week’s World Health Assembly (WHA). While holding detailed discussions to plan for a polio-free world, delegates emphasized the need to finish the job of eradication.
With wild poliovirus transmission levels lower than ever before, Ministers of Health and delegates reviewed progress being achieved through national emergency action plans in the remaining endemic countries. As at May 2018, only eight cases due to wild poliovirus had been reported globally, from just two countries: Afghanistan and Pakistan.
To prepare for a polio-free world, Member States adopted a landmark resolution on poliovirus containment. A limited number of facilities will retain poliovirus after eradication, to serve critical national and international functions such as the production of polio vaccine or research. It is crucial that these poliovirus materials are appropriately contained under strict biosafety and biosecurity handling and storage conditions, to ensure that virus is not released into the environment, either accidentally or intentionally, to again cause outbreaks of the disease in susceptible populations.
WHO and countries that are currently funded by the Global Polio Eradication Initiative (GPEI) face significant financial, human resource, and programmatic risks as a result of the scaling down of the GPEI budget (2017-2019) and its eventual closure. Hence, Member States requested the Director-General to develop a strategic action plan on polio transition that will mitigate these risks, as well as strengthen country health systems. Delegates considered the resulting 5-year strategic action plan on polio transition, which has 3 key objectives: (i) sustaining a polio-free world after eradication of polio virus; (ii) strengthening immunization systems, including surveillance for vaccine-preventable diseases; and (iii) strengthening emergency preparedness, detection and response capacity in countries to ensure full implementation of the International Health Regulations. The strategic action plan outlines how essential polio functions like surveillance, laboratory networks, and some core infrastructure can support the implementation of the Post Certification Strategy to sustain a polio-free world, and can be integrated into the immunization or health emergencies’ programme, or mainstreamed into national health systems. The plan provides detailed costing for the integration of essential polio functions into WHO’s Thirteenth General Programme of Work, and some financing options. The three polio-endemic countries (Afghanistan, Pakistan and Nigeria) and a few high-risk countries battling outbreaks have been excluded from transition planning until eradication. All other GPEI-funded countries are expected to plan for polio transition.
Member States expressed overwhelming commitment to fully implement and finance all strategies to secure a lasting polio-free world in the very near term. Rotary International, speaking on behalf of the GPEI, which includes WHO, Rotary, CDC, UNICEF and the Bill & Melinda Gates Foundation, offered an impassioned plea to the global community to eradicate a human disease for only the second time in history, and ensure that no child will ever again be paralysed by any form of poliovirus anywhere.
A vaccine manufacturer in Stockholm has taken the first step towards becoming a certified Poliovirus Essential Facility (PEF), leading the charge in global efforts to safely and securely contain type-2 poliovirus. This facility has been awarded a Certificate of Participation co-signed by the National Authority for Containment (NAC) in Sweden and the Global Commission for the Certification of Poliomyelitis Eradication (GCC). The Certificate is the first of its kind to be issued, indicating formal engagement in the global containment certification process.
Wild poliovirus type-2 was declared eradicated by the GCC in September 2015, however, there is risk of the virus resurging. Following the removal of the type-2 component from oral polio vaccine (OPV) and the discontinuation of type-2 containing OPV from routine use in April 2016, countries around the world have been asked to safely and securely destroy their type-2 polio samples. As a further precaution, countries continue to immunize against type 2 polioviruses with inactivated polio vaccine. For facilities needing to retain the virus for vaccine production or for critical research, stringent containment measures need to be followed. The first step is getting a Certificate of Participation.
“We are pleased to see Sweden leading the way in demonstrating conforming with the processes to minimize the risk of releasing type-2 poliovirus into the environment. Participation in the Containment Certification Scheme shows that both the facility and the host country are serious about taking on and implementing the safeguard measures necessary to become a PEF,” said Prof. David Salisbury, Chair of the GCC and of the Commission’s European regional body.
“Handling and storing an eradicated pathogen is a risk and responsibility – a leak or breach could have devastating consequences,” said Michel Zaffran, Director of Polio Eradication at the World Health Organization. “We commend Sweden for its commitment towards ensuring safety standards are met and protocols are in place to help minimize risk, and for paving the road for the containment certification process,” he said.
“The issuance of a Certification of Participation formally engages a designated PEF in the containment process. Provided that the facility meets the requirements outlined in Global Action Plan III for the containment of polioviruses (GAPIII) within given time frames, it can then progress to achieving an Interim Certificate of Containment and finally, a full Certificate of Containment to become an accredited PEF,” said Prof. Salisbury. “Countries planning to retain type-2 poliovirus will need to establish their NACs as soon as possible, and by no later than the end of 2018. The GCC urges all countries that plan to have PEFs to get the ball rolling in this process,” he said.
Since April 2016, most facilities around the world have opted to destroy their type-2 poliovirus materials rather than contain them. Twenty-nine countries, however, plan to continue to handle and store their materials in 92 designated PEFs.
WHO will propose a resolution for consideration by the World Health Assembly in May to seek international consensus on accelerating containment efforts globally.
To supplement Global Action Plan III for the containment of polioviruses, WHO has published guidance for non-polio facilities to help them identify, destroy, or safely and securely handle and store sample collections potentially infectious for poliovirus.
Dr Mark Pallansch from CDC explains what the guidance means for facilities worldwide.
Poliovirus potentially infectious materials (PIM) include fecal, nasopharyngeal, or sewage samples collected in a time and place where wild polioviruses/vaccine-derived polioviruses (WPV/VDPV), or OPV-derived viruses were circulating or oral polio vaccines (OPV/Sabin) were in use. Non-polio research facilities with a high probability of storing such materials include those working with rotavirus or other enteric agents, hepatitis viruses, influenza/respiratory viruses, and measles virus. Other facilities could include those conducting nutrition research or environmental facilities.
Ondrej Mach of the WHO polio research team discusses why new inactivated polio vaccine solutions are needed for the post-eradication era. Why are we developing entirely new vaccines for a disease which will no longer exist?
The Global Certification Commission (GCC) for the eradication of polio, supported by the Containment Working Group, are now ready to review and endorse or reject applications for certificates of participation in the containment certification process, following approval by national aurhorities for containment.
The certificate of participation is the first stage of the containment certification process for laboratories and other facilities designated to retain poliovirus type 2.
Containment certification aims to ensure the safe and secure storage and handling of stocks of poliovirus around the world, minimizing the risk of the virus’ release back into the community after eradication. Containment is an important part of the poliovirus eradication process.
At the 70th World Health Assembly in Geneva, global health leaders have reiterated their commitment to polio eradication, discussing progress made and challenges ahead and emphasising the critical need for effective transition planning for the post-polio era.
Member States spoke of the continuing steady progress towards eradication, and the importance of supporting the remaining endemic countries in finishing the job. With only 37 cases in three countries in 2016, achieving eradication is closer than ever before.
Delegates from Afghanistan, Pakistan, and Nigeria, the last three endemic countries, outlined their key strategies for ending transmission as a matter of priority. The Pakistani delegate underscored the need for continued support from the global community: “Last miles are difficult, but we need to stay the course and reach a significant public health landmark of our time.”
Michel Zaffran, Director of Polio Eradication at WHO, spoke of the impressive decline in cases, achieved through the commitment of Member States, and stressed the critical need to continue to support the endemic countries in their efforts to stop the virus.
“We stand on the brink of making history, but progress is fragile… We cannot lower our guard. We must redouble our efforts to support Nigeria, Pakistan and Afghanistan to implement their national emergency action plans, and ensure they have the resources to do so.”
Member States also addressed the challenge of the scale down of the polio programme as eradication comes closer, including the potential impact on achieving and sustaining a polio-free world, on health programmes and systems currently supported by polio assets, and on WHO itself. They welcomed existing efforts to plan for the post-polio world, and stressed the importance of careful, considered, and strategic approaches to the transition of polio assets, requesting the WHO Director-General to prepare a detailed transition action plan.
Many delegates expressed concern about the ongoing shortage of inactivated polio vaccine, and noted the need to implement containment measures to ensure the safe and secure storage and handling of materials containing polioviruses, and destroy unneeded materials.
Rotary International reaffirmed the commitment of their 1.2 million volunteers to the global polio eradication effort, and expressed cautious optimism about the low levels of transmission in 2017. The Rotarian speaker called for the support of all countries to achieve eradication. “The support of every country is needed now more than ever. Passive support is not enough; we will not succeed without political and financial commitment… Let’s make history and end polio together.”
Photo: GPEI
As of this month, 176 countries and territories around the world have reported that they no longer have any wild or vaccine-derived poliovirus type 2.[1] Twenty-nine countries have reported that some facilities will likely retain the type 2 virus. These facilities and their host countries will need to work together closely to meet the containment requirements in GAPIII – the Global Action Plan for poliovirus containment.
In September 2015, the Global Commission for the Certification of Poliomyelitis Eradication (GCC) declared that wild poliovirus type 2 has been eradicated. While this virus is no longer found among people or in the environment, some laboratories or facilities around the world still use and store the virus for a variety of reasons, such as producing polio vaccines or conducting research.
If poliovirus is accidentally or intentionally released into the community from one of these facilities, polio could come back and cause paralysis and death. This can especially happen in areas where polio vaccination coverage is low. However, even in countries with high polio vaccination coverage, some people may not be vaccinated or protected against polio, putting them at risk of getting the disease if they are exposed.
To reduce the risk of any poliovirus type 2 being released into the community, countries are either destroying unneeded virus in some facilities, or designating certain facilities as poliovirus essential facilities that will safely and securely retain the virus.
Support for Containment
Of the 29 countries hosting these facilities, 18 have nominated national authorities to make sure poliovirus containment certification activities are appropriately conducted in their country, and to certify facilities on the biorisk management requirements in GAPIII.
WHO is providing key support for containment activities, including:
conducting workshops for countries on GAPIII, the auditing process, and certification
creating a list of auditors who can help countries audit facilities to assess if they meet the biorisk management requirements in GAPIII
The Global Polio Eradication Initiative has formed three groups to help strengthen poliovirus containment efforts in countries:
The Containment Working Group will support the GCC in its role of providing oversight for poliovirus containment activities worldwide. This group will review applications for certification received from the countries and make recommendations to the GCC.
The Containment Advisory Group will make recommendations to the Director-General of WHO on technical issues related to GAPIII.
The Containment Management Group will provide GPEI oversight, partner coordination, and management support for containment.
Containment of eradicated polioviruses is a key objective of the Polio Eradication and Endgame Strategic Plan, and is critical to ensuring that the world is kept free of polio after eradication.
This series of six short videos explain the important steps that are being taken to make sure that, once the poliovirus has been eradicated, it will never have the opportunity to return. We have never been closer to achieving our goal; but there is much still to be done to secure a polio-free world.
Once wild polio has been eradicated, the only risks of the virus returning would come from rare strains of circulating vaccine derived polioviruses, and from potential leaks of the virus from laboratories or vaccine manufacturers. This series of videos will explain the work being done to address these risks: from the vaccines that are being used to stop polio; to how the oral polio vaccine is being phased out from April 2016 to remove any risk of vaccine-derived polioviruses, starting with the switch from trivalent to bivalent oral polio vaccine in April 2016; and how securely containing polioviruses within laboratories and vaccine manufacturing sites will keep every last child protected, long into the future.
Two vaccines have brought us to the brink of a polio-free world: the oral polio vaccine and the inactivated polio vaccine. Learn how these vaccines work and the different, complementary roles they have to play in delivering a polio-free world.
In order to secure a polio-free world for all future generations, we must eradicate all strains of the virus. Learn about wild polioviruses and vaccine-derived polioviruses, and what needs to be done to stop both strains for good.
Learn about the switch from trivalent bivalent oral polio vaccine in April 2016 – the biggest, globally-synchronised project in the history of vaccines – and why gradually phasing out the oral polio vaccine is essential to prevent the emergence of circulating vaccine-derived polioviruses in the future.
Learn about the safety nets being put in place to make sure that the phased withdrawal of the oral polio vaccine will speed up our journey towards a polio-free world, such as the introduction of the inactivated polio vaccine into routine immunization programmes.
An important part of securing a polio-free world is making sure that laboratories and vaccine manufacturing facilities handle and store polioviruses safely and securely. Through this video, learn why poliovirus containment is now more important than ever in order to keep current and future generations safe from polio.
Poliovirus exists in laboratories and vaccine manufacturing facilities around the world WHO/Leilia Dore
In September 2015, the Global Commission for the Certification of Poliomyelitis Eradication (GCC) declared that wild poliovirus type 2 has been eradicated. However, the virus still exists in laboratories and vaccine manufacturing facilities around the world. The GCC explains the importance of containing poliovirus safely and securely in a recent article in Science magazine.
All countries should now destroy or safely and securely contain poliovirus type 2 so that it is not released to again cause paralysis or death. To do this, laboratories and vaccine manufacturing facilities need to implement the measures outlined in the WHO Global Action Plan (GAPIII) for poliovirus containment, endorsed by ministries of health in all 194 WHO Member States at the World Health Assembly in May 2015.
A lesson regarding the need for appropriate containment is the 1978 release of the then eradicated smallpox virus from a laboratory in the United Kingdom, resulting in a person dying from the disease. This triggered countries to further reduce the number of facilities retaining smallpox virus to the two official repositories that remain today.
The Global Polio Eradication Initiative is working with countries to limit the number of facilities retaining polioviruses to the minimum necessary to perform international functions, such as vaccine production and critical biomedical research.