Over the course of 2015, Pakistan has seen encouraging signs of progress against polio, with the programme tightening its grip on the last strongholds of the virus. The number of cases has declined sharply, with 39 reported to date in 2015, compared with 235 cases by the same point in 2014.
Not children reached, but children missed
One of the most important changes of the last year was a shift in focus from the number of children reached to the number missed during immunization campaigns. “How many missed, where and why?” became the determining question. The results of this shift are clear, with almost half a million children who were previously missed by vaccinators now being reached, due to gradual improvements in programme quality and access to previously unreachable areas since late 2014.
This week’s Morbidity and Mortality Weekly Report from the US Centers for Disease Control and Prevention attributes recent improvements to the establishment of a functioning Emergency Operations Centre (EOC), based on the model that contributed to success in Nigeria. A sign of the successful increase in political engagement at both regional and national levels, the EOC serves as a platform for increased government ownership of the polio programme, close collaboration among the partners of the Global Polio Eradication Initiative, and the implementation of new strategies outlined in the National Emergency Action Plan such as health camps, which have reached almost 350,000 people in high-risk areas with additional health services alongside polio vaccines this year.
As Pakistan zeroes in on continuously missed children, misconceptions about the polio vaccines and issues of inaccessibility in certain security challenged areas continue to pose challenges. An innovative approach to addressing these issues has been introduced through Continuous Community Protected Vaccination (CCPV), in which local, predominantly female community health workers are engaged to vaccinate the children of their own communities on a regular basis. With over 80% of polio cases occurring to children under two years old, there was a need to deploy vaccination teams who are in constant contact with children in the communities. CCPV was introduced in selected high-risk reservoir districts of Khyber Pakhtunkhwa and the Federally Administered Tribal Areas, using primarily female vaccinators who are more likely to gain access to households.
While cases have fallen, the virus is geographically widespread. Punjab, with no cases during 2014, has reported a case in 2015 and continues to show evidence of virus presence through environmental surveillance. Peshawar and its surrounding regions remain the heart of this reservoir of the virus, acting as a source of transmission to other parts of the country and into Afghanistan.
In order to stop the transmission of polio in Pakistan in 2016, a lot of work remains to be done. We must close immunity gaps by locating and vaccinating every last child and improving routine immunization coverage in high-risk areas. The Government of Pakistan must continue to demonstrate its leadership and to provide oversight and accountability through provincial and national EOCs. It will also be necessary to improve oversight and accountability for vaccinations delivered at transit points both inside Pakistan and at the borders with Afghanistan.
Health camps ensure that the most remote communities in high risk areas of Pakistan have access to life-saving vaccines and other health services. EOC Pakistan
In the shade of a tree in the remote village of Chandiya in Dera Ghazi Khan district of Punjab, a crowd of people wait their turn to receive medical treatment. Reaching children and their parents who all too often do not receive basic health care and water and sanitation services, these camps deliver polio vaccines to the children who most need them, alongside other important health services.
“This is a rare chance that a doctor is visiting our village to give us free check-up and medicines. It’s a blessing for us to services right at our neighbourhood,” said Sher Ali, a local standing in the crowd who had brought his child for vaccination.
This scene is not unique; across Pakistan, 1857 health camps have been set up by the Government of Pakistan with support from technical partners and donors. So far this year, 480 538 people have benefitted from the health services delivered at these camps, including 10 000 children under the age of five who have never previously received the oral polio vaccine. This has made health camps a vital tool in Pakistan’s push to identify and protect the children who have been missed by polio campaigns in recent years.
Dera Ghazi Khan borders several high risk areas for polio, including Balochistan, Sindh and Khyber Pakhtunkhwa. Therefore health camps like this one are essential for combatting the low immunization coverage, poor health services and misconceptions circulating among parents about oral polio vaccine, all of which leave many of the children of the district vulnerable to the virus.
Balochistan has the highest number of cases in any province of Pakistan, largely centred on the Quetta area. This drawing shows a vaccination centre, with community members informing each other about polio vaccination at the centre. A polio-affected child with crutches watches children playing and wishes he could join their play. Drawn by Fazeela, 6th grade
Drawn by an 8th grader from a local government school of Kharotabad, where three cases of polio have been confirmed in 2011, this picture shows a polio-affected child and other children. A mother of a polio survivor talks to a vaccinator, warning her to tell parents, "Never repeat the mistake I committed, my child is crippled. I request all the parents to vaccinate their children against polio.” Drawn by Fida Mohammad, 8th grade
Fifty students from ten schools of four high risk union councils participated in the drawing competition. Here, religious leaders and tribal members are marching, holding banners with slogans of a polio free Pakistan. The child shows in her art the active community participation from both religious and non-religious communities that is critical for polio to be eradicated. Drawn by Shakila Khan, 7th grade
Within the five high risk districts of Balochistan, 70 union councils in have been classified as high risk on the basis of persistent transmission, low quality campaigns, mobile population and hard to reach areas due to insecurity. Here, a polio affected child watches other children playing and thinks, “If only my parents had vaccinated me against polio I would have been playing like these children.” Drawn by Neelam Khan, 7th grade
Prime Minister’s Focal Person on Polio Eradication, Senator Ayesha Raza Farooq administers polio drops to a child in Islamabad during the first day of the nationwide immunization campaign.
Pakistan Polio Eradication Initiative
Pakistan launched a nationwide polio campaign yesterday to vaccinate more than 35 million children in 163 districts of the country. Approximately 200,000 polio workers are participating in the polio campaign, during which Vitamin A will also be distributed.
The Prime Minister’s Focal Person on Polio Eradication, Senator Ayesha Raza Farooq, monitored the campaign in various areas of Islamabad including urban and rural slums, reminding administrators that there would be zero tolerance for negligence. “Our priority is to reach out each and every child so that no child remains unvaccinated during this nationwide polio drive”, said Senator Farooq during her visit. “Nine campaigns are planned during September 2015 to May 2016 and every campaign is critically important to stop polio virus transmission.”
Pakistan currently accounts for most of the children paralyzed by wild poliovirus this year (30), followed by Afghanistan (9). These are the only two countries in the world with wild poliovirus cases in 2015: the lowest number of countries in history. Pakistan country is well-positioned to take advantage of the the current ‘low season’ for poliovirus transmission; it has prepared emergency operations centres at federal and provincial level and is improving its ability to hold every level of the administration accountable for delivering vaccine to children. The quality of these campaigns – whether missed children are given the opportunity to be vaccinated – will determine how swiftly Pakistan can eradicate polio.
Pakistan has become the second polio-endemic country to introduce the inactivated polio vaccine into the country’s routine immunization schedule, a move which will benefit more than four million children per year across the country. With more than half of the global birth cohort now receiving IPV due to the largest globally synchronised vaccine introduction in history, the addition of Pakistan’s children to this number will help to speed Pakistan towards stopping the virus for good.
Pakistan is one of only three countries in the world where polio remains endemic. Nigeria, which recently marked one year without a case of wild polio, introduced the vaccine in February of this year, and Afghanistan is due to begin using IPV in the coming weeks. While every country in the world is set to introduce IPV, endemic countries will greatly benefit from the boost in immunity that new evidence has clearly demonstrated that adding one dose of IPV to OPV offers to children as they fight to end transmission of the virus. Aziz Memon from Rotary International emphasized that “… adding at least one dose of IPV to the routine immunisation schedule is the best possible way to protect your children from life-long polio paralysis, while the disease is being eradicated from the remaining endemic hotspots.”
The universal introduction of IPV is part of the Polio Eradication and Endgame Strategic Plan 2013-2018. It helps to build a solid base-layer of immunity against polio, and will help to secure the gains made against the disease by contributing to stronger immunisation systems, so that every child in every country has access to vaccines. “The introduction of IPV is a major landmark as it would strengthen our efforts to fight polio and eventually eradicate it from our country and the world. We are confident that this introduction will give a boost to routine immunization in the country,” said Mrs Saira Afzal Tarar, Minister of State, Ministry of National Health Services Regulation and Coordination.
Pakistan has made significant progress in the fight against polio with a 75% reduction in the number of cases of wild poliovirus compared to the same period last year (from 115 cases to 29 cases). This decline shows that, despite major challenges and remaining hurdles in some provinces, Pakistan is getting closer to polio eradication. However, the country still accounts for more than 80% of cases worldwide so far this year, and many children in high-risk areas of the country remain un- or under-immunised.
As well as its use in routine immunization, the ability of IPV to boost immunity when used alongside OPV is being utilized in polio campaigns. In critical areas of the Federally Administered Tribal Areas such as South Waziristan and Khyber Agency, which were which were not consistently reached due to insecurity over the last few years, IPV campaigns are ongoing targeting children between 4 and 24 months. The children of families returning to North Waziristan, South Waziristan and Khyber Agency following displacement are also given IPV to increase their immunity as they are a particularly vulnerable group. While OPV is still the only vaccine that can end transmission of the virus, IPV can provide a boost to speed up the development of immunity to all types of poliovirus.
“The introduction of IPV is a result of significant progress for our country in term of strengthening routine immunization,” said Dr. Syed Saqlain Ahmad Gilani, National Program Manager, EPI. “We are another step closer to ridding the world of the terrible disease of polio, and it is a result of our efforts to improve the current state of routine immunization in the country.”
Read more about the global status of IPV introductions here.
The Bill & Melinda Gates Foundation, Norway, and the United Kingdom are generously supporting the introduction of IPV in routine immunisation schedules in 72 Gavi-supported countries, while Canada is supporting its introduction in other lower-middle income countries. The top ten government donors to GPEI include the USA, the UK, Japan, Germany, Canada, the Netherlands, Norway and Australia.
The Global Polio Eradication Initiative (GPEI) is led by national governments and spearheaded by the World Health Organization (WHO), Rotary International, the US Centers for Disease Control and Prevention (CDC), and the United Nations Children’s Fund (UNICEF), with the support of the Bill & Melinda Gates Foundation.
Since its launch at the World Health Assembly in 1988, the GPEI has reduced the global incidence of polio by more than 99%. The GPEI receives financial support from governments of countries affected by polio; private sector foundations, donor governments, multilateral organizations, private individuals, humanitarian and nongovernmental organizations and corporate partners.
A child in Nigeria is given a dose of the inactivated polio vaccine, helping to protect them against all strains of poliovirus. Nigeria introduced the vaccine in February 2015, the first of the polio-endemic countries to do so. UNICEF
The Global Polio Eradication Initiative (GPEI) is midway through the most ambitious, largest and fastest globally synchronised vaccine introduction in history as part of its drive towards a polio-free world.
How far have we come?
As part of the Endgame strategy for polio eradication, the inactivated polio vaccine (IPV) is being introduced into the routine immunization systems of every country that currently uses the oral polio vaccine (OPV). Half way into 2015, exciting progress is being made towards this goal, which will help to boost immunity against all types of poliovirus, giving children higher protection against paralytic polio.
51% of the global birth cohort is now receiving at least one-dose of IPV
The introduction of IPV has already made great strides, with 20 countries adding the vaccine to their immunization schedules between January and July this year alone, bringing the number of countries using the vaccine to 97. This means that 51% of the global birth cohort is now receiving at least one-dose of IPV. A surge of introductions in the coming months will lead to over 75% of countries having at least one dose of IPV in their routine immunization systems by the end of October. By the end of the year, all countries with the highest risk of wild poliovirus or the emergence of vaccine-derived polioviruses- the highest priority categories for IPV introduction- will have completed the introduction. This will ensure that the most vulnerable children are given the best possible protection against polio.
Two vaccines for polio
The polio eradication programme has two vaccines with which it protects children against the virus: IPV and the OPV. The use of the oral polio vaccine (OPV) has led to wild poliovirus being stopped in nearly every country in the world, and to no cases of wild poliovirus type 2 (WPV2) since 1999. Currently, 156 countries and territories use trivalent OPV (tOPV), which protects children against all three types of wild poliovirus, to vaccinate children against polio in their routine immunization programmes. While OPV is the only vaccine that is effective in stopping the transmission of poliovirus during outbreaks, the introduction of IPV in these countries will increasingly play an important role in keeping those countries polio-free in the long term.
The weakened type 2 strain of attenuated poliovirus in tOPV is no longer needed to protect children from wild polio, as no case of type 2 has been seen since 1999. In addition, the type 2 component of OPV causes more than 90% of all vaccine derived polioviruses (VDPVs), which occur when a very rare change in the attenuated virus in the vaccine mutates into a form that may cause paralysis. This can only occur where vaccination coverage is very low. To protect children from this very rare risk, OPV will be removed in a phased manner over the next few years. The first step is to replace tOPV with bivalent OPV (bOPV), which doesn’t contain the type 2 component, thereby removing the risk of type 2 VDPVs.
Why introduce IPV?
1. Giving IPV alongside OPV has been shown to be the most effective way of rapidly building immunity against all types of poliovirus. The introduction of IPV prepares children’s bodies for a rapid build-up of immunity in case an outbreak after the switch would need fast campaigns to protect children against the virus.
2. IPV will build up some level of population immunity against the type 2 polioviruses. When the type 2 component of OPV is withdrawn, children will no longer be protected against wild poliovirus type 2. While no wild poliovirus type 2 has been seen since 1999, maintaining some immunity through IPV will be important to mitigate the risks.
3. IPV will boost immunity against poliovirus types 1 and 3 in children who had previously received OPV, bringing us closer to a world in which every child is fully protected and stopping the virus for good.
The wider impact
Strengthening routine immunization systems is a core pillar of the strategy of the Global Polio Eradication Initiative. As IPV is an injectable vaccine it needs to be delivered by a trained health worker, unlike OPV, making the urgency of strengthening routine immunization has become even more apparent. In many countries, such as Bangladesh, the introduction of a new vaccine such as IPV provides an opportunity to strengthen the entire system through the expansion of cold chains, training health workers, and renewed community outreach. By using the lessons learned through the eradication of polio to strengthen routine immunization, the GPEI is ensuring that the legacy of polio eradication stretches into the future in more ways than providing a polio-free world.
The Bill & Melinda Gates Foundation, Norway, and the United Kingdom are generously supporting the introduction of IPV in routine immunisation schedules in 72 Gavi-supported countries. In addition, Canada is providing critical catalytic one-year support to help 19 lower middle income countries, enabling them to introduce IPV.
By increasing immunity against all strains of poliovirus, filling the immunity gap against type 2 and helping to enable the removal of type 2 OPV, this global vaccine introduction is helping to secure a lasting, polio-free world for everyone.
Read more about the global introduction of inactivated polio vaccine and the switch here or see find more information on the WHO website.
The Global Polio Eradication Initiative (GPEI) receives financial support from governments of countries affected by polio; private sector foundations, donor governments, multilateral organizations, private individuals, humanitarian and nongovernmental organizations and corporate partners-. A full list of all contributors is available here.
Status of IPV use in routine immunization systems in January 2013:
1
2
Reaching missed children is now the main focus of the polio eradication programme in Pakistan, which has led to a drop in polio cases this year. WHO
The world has never been in a better position to eradicate polio, yet Pakistan and Afghanistan face a daily battle to protect children against the virus. Pakistan, the single greatest challenge to global eradication, is getting back on track to stop transmission of polio in 2015, concluded the Technical Advisory Group (TAG) at their meeting in Islamabad on 4 and 5 June.
In 2014, Pakistan reported 85 % of the world’s polio cases. This year has seen 26 children paralysed by polio, 72% less than we had seen by this time in 2014. This drop in cases is evidence that, despite major challenges and remaining hurdles in greater Peshawar, Khyber Agency, the Federally Administered Tribal Areas (FATA), and the central Pakistan block, Pakistan is taking steps forward towards a polio-free future.
Every missed child
Key to improvements over the last few months has been the shift in focus to finding and vaccinating every missed child – rather than focusing on the numbers of children reached and vaccinated. The TAG was encouraged by the fact that the number of persistently missed children had significantly declined in all major areas including South Waziristan, parts of Peshawar and Karachi. Similarly, the exodus from North Waziristan due to military campaigns in 2014 was grabbed as an opportunity to vaccinate longstanding un-reached and unvaccinated populations. Ongoing innovations specific to each area and enhanced community engagement are the key tools being used to bring those numbers of missed children down to zero.
Pieces of the puzzle
Since the most recent consultation in February, the TAG recognised that significant progress has been made, especially through the adoption of innovations such as the use of the inactivated polio vaccine (IPV) in supplementary immunization activities, measures to protect the safety of health workers, and the health camps to reach children with vaccines alongside other health measures.
Pakistan has all the tools it requires to stop transmission of polio. It remains crucial that these tools are utilised to ensure that the final pieces of the puzzle come together in practice to see concrete change over the current high season for transmission. These essential aspects are an accountable government at all levels, community trust and health worker safety, engaged community leaders, the continued use of innovative solutions and ensuring that the programme are using the right vaccines in the right places, such as the inactivated polio vaccine (IPV) in campaigns in hard to reach areas to build immunity more rapidly.
Insecurity in certain areas remains the biggest obstacle to polio eradication in Pakistan, resulting in delayed or missed campaigns. Combatting this is where non-traditional tools, such as female community volunteers and health camps, have proved most valuable. “We cannot allow conflict and politics to get in our way because at the end of the chain, behind that door, stands a mother or a father who wants to protect their child,” argued Dr Hamid Jafari, Director of Polio Operations and Research at WHO.
The National Emergency Action Plan for Pakistan has outlined an action plan to stop transmission as soon as possible by detecting, containing and eliminating the virus, maintaining and increasing immunity, and strengthening routine immunization to help sustain protection once transmission is stopped. The plan aims at reaching every child with multiple doses of the vaccine between September 2015 and May 2016. The programme is strengthening and preparing to stand absolutely ready for high quality implementation by mid-August. The programme will also have to ensure it continues to coordinate with Afghanistan, following spread of viruses across the border in both directions. Along the 2450 km border, temporary vaccination points are in place to coincide with movement of seasonal workers, pilgrims and those forced to leave their homes due to extreme weather conditions.
“The recent progress in Pakistan is very promising. We may be looking at months- months, not years- before we eradicate polio in this country,” stated Dr Jafari. If all elements of the polio programme are accountable for reaching and immunizing every child in polio vaccination campaigns, Pakistan can take the world over the finishing line for polio eradication.
Key to improvements over the last few months has been the shift in focus to finding and vaccinating every missed child – rather than focusing on the numbers of children reached and vaccinated. The TAG was encouraged by the fact that the number of persistently missed children had significantly declined in all major areas including South Waziristan, parts of Peshawar and Karachi. Similarly, the exodus from North Waziristan due to military campaigns in 2014 was grabbed as an opportunity to vaccinate longstanding un-reached and unvaccinated populations. Ongoing innovations specific to each area and enhanced community engagement are the key tools being used to bring those numbers of missed children down to zero.
Since the most recent consultation in February, the TAG recognised that significant progress has been made, especially through the adoption of innovations such as the use of the inactivated polio vaccine (IPV) in supplementary immunization activities, measures to protect the safety of health workers, and the health camps to reach children with vaccines alongside other health measures.
Pakistan has all the tools it requires to stop transmission of polio. It remains crucial that these tools are utilised to ensure that the final pieces of the puzzle come together in practice to see concrete change over the current high season for transmission. These essential aspects are an accountable government at all levels, community trust and health worker safety, engaged community leaders, the continued use of innovative solutions and ensuring that the programme are using the right vaccines in the right places, such as the inactivated polio vaccine (IPV) in campaigns in hard to reach areas to build immunity more rapidly.
Insecurity in certain areas remains the biggest obstacle to polio eradication in Pakistan, resulting in delayed or missed campaigns. Combatting this is where non-traditional tools, such as female community volunteers and health camps, have proved most valuable. “We cannot allow conflict and politics to get in our way because at the end of the chain, behind that door, stands a mother or a father who wants to protect their child,” argued Dr Hamid Jafari, Director of Polio Operations and Research at WHO.
The National Emergency Action Plan for Pakistan has outlined an action plan to stop transmission as soon as possible by detecting, containing and eliminating the virus, maintaining and increasing immunity, and strengthening routine immunization to help sustain protection once transmission is stopped. The plan aims at reaching every child with multiple doses of the vaccine between September 2015 and May 2016. The programme is strengthening and preparing to stand absolutely ready for high quality implementation by mid-August. The programme will also have to ensure it continues to coordinate with Afghanistan, following spread of viruses across the border in both directions. Along the 2450 km border, temporary vaccination points are in place to coincide with movement of seasonal workers, pilgrims and those forced to leave their homes due to extreme weather conditions.
“The recent progress in Pakistan is very promising. We may be looking at months- months, not years- before we eradicate polio in this country,” stated Dr Jafari. If all elements of the polio programme are accountable for reaching and immunizing every child in polio vaccination campaigns, Pakistan can take the world over the finishing line for polio eradication.
With the introduction of two new vaccines, Bangladesh’s Extended Program on Immunization now protects children against 10 diseases. GAVI
On 21 March, the Extended Program on Immunization (EPI) in Bangladesh launched both the Inactivated Polio Vaccine (IPV) and the Pneumococcal Conjugate Vaccine into their Routine Immunization programme. With polio stopped in 2000 and 94% routine coverage by 2 years of age, Bangladesh has many lessons to share with other countries on how to provide strong protection against vaccine preventable diseases.
IPV Introduction in a Strong Routine Immunization System
EPI in Bangladesh is remarkable for the ownership felt for the program at all levels, from the Government to health workers to parents who actively seek out vaccines. This commitment is evident in the dual introduction for IPV and PCV, which enabled streamlining on training, logistics and the health workforce.
Movement around the country has been limited since January, due to road blockades for political reasons, giving the introduction a challenging backdrop. Innovative transportation techniques, the incredible commitment of staff and the power of the yellow EPI banner which shines out from every vehicle and denotes every EPI clinic made it possible to get the new vaccines to healthcare centres, despite the challenges.
Before any vaccine introduction, a cascade of improvements for the entire EPI system takes place. To accommodate two new vaccines into the system, international partners helped government to assess cold chain capacity, secure vaccine stocks, train all health workers and engage influential leaders. Dr Abdur Rahim, Program Manager of EPI at the Ministry of Public Health, explained: “Every time we introduced a new vaccine in the past few years, we saw an increase in overall coverage.” He hopes that this dual introduction will provide the necessary push to bring coverage to 90%.
With the addition of IPV and PCV, Bangladesh is now protecting children against 10 diseases. “This makes Bangladesh one of the model countries in South Asia, with many lessons to share with the rest of the world,” said Dr Jayantha Liyanage from WHO at the launch on March 21.
Polio’s Contribution to Bangladesh’s EPI System
Bangladesh’s historic success in stopping polio in 2000 set the foundation that enabled this introduction. The capacity of staff, lessons learned over many years of National Immunization Days (NIDs) and high community engagement all contributed to the strength of the system today, which is remarkable in a low income country with such a high birth cohort and many other public health challenges.
Bangladesh is an example of a country where routine immunization and polio eradication have worked in synergy for so long that the former now carries the latter. This process of synergy gained its strength from the way in which partnerships grew between the government, organizations such as WHO, UNICEF and Rotary International, and civil society organisations. The longstanding history of the program means that all stakeholders know their roles well, explains Dr N. Paranietharan, Head of WHO Country Office in Bangladesh. “There may be new challenges; however the public health approaches to respond to them remains the same.”
Bangladesh is an example of a country where routine immunization and polio eradication have worked in synergy for so long that the former now carries the latter.
Years of NIDs established and strengthened channels of communication, building all-important trust between the people and the EPI system. NIDs became festive occasions across the country, with Rotary and UNICEF doing everything they could to engage parents in the campaigns, with elephants, balloons, and music in the streets. “Just a generation or two ago, vaccine preventable diseases caused so many deaths, and now so few. This is incredible, visible change. When people saw vaccinated children staying healthy, it motivated the whole country,” describes Dr Abdur Rahim. “All walks of life have contributed to this program, so they all are committed to ensuring it remains strong and continues to improve.”
Bangladesh now faces the challenge of addressing inequity in coverage. Urban areas prove a particular challenge, where population movements, low levels of sanitation in slums and a less structured infrastructure need to be addressed.
Working for a Stronger Future
While polio has not been seen in the country since the end of the outbreak in 2006, the programme continues to play a role in helping to address the challenges of the entire system. “We are keeping our commitment to polio eradication strong, despite not having seen the disease for so many years. It is important for us to avoid the risk: as long as neighbouring countries are vulnerable to polio, awareness of the threat needs to be maintained,” explains Dr Paranietharan. “But the efforts aren’t just for polio. Polio eradication is so integrated that all the efforts are towards strengthening systems for routine immunization.”
The first child in the Federal Capital Territory receives the inactivated polio vaccine WHO/AFRO
This February, Nigeria became the first polio endemic country to introduce the inactivated polio vaccine (IPV) into its routine immunization system. The Minister of Health, Dr Alhassan Khaliru, described this as “… a quantum-leap opportunity for Nigeria in the polio eradication endgame strategy”.
The introduction of IPV into routine immunization systems is part of one of the four major objectives of the Global Polio Eradication Initiative (GPEI). In May 2012, the World Health Assembly called on all countries which were using only the oral polio vaccine (OPV) to introduce at least one dose of IPV into routine immunization schedules by the end of 2015. This is the largest globally coordinated vaccine introduction project in history.
The launch in Nigeria was supported by the partners of the GPEI, including the Nigerian Government, the World Health Organization, UNICEF, Rotary International, the Centers for Disease Control and Prevention and the Gavi Alliance. Speaking at the launch ceremony, the Minister stated that combining OPV and IPV had threefold benefits: acting as risk mitigation in the global plan to phase out the use of OPVs in 2016, boosting immunity against type 1 and 3 wild poliovirus (WPV) and also tackling the risk of circulating vaccine-derived poliovirus (cVDPV).
While OPV is extremely safe and has led the world to the threshold of being polio-free, on very rare occasions its use can lead to vaccine-associated cases. For this reason, the global eradication of polio requires the cessation of all OPV use, once polio has been eradicated. IPV will then be the only option for countries to maintain immunity levels.
IPV will be introduced in phases. This first phase has introduced IPV in 2 northern endemic States, Bauchi and Jigawa, while the second phase will see the vaccine introduced in the remaining states by 16 March 2015.
Nigeria remains one of the last three countries with endemic WPV transmission, and is also struggling with an outbreak of cVDPV. Significant progress has been made in the past year against WPV, with increased government ownership of the programme and innovative approaches in recent years leading to no cases having been reported for seven months. Yet the World Health Organization Country Representative, Dr Rui Gama Vaz, cautioned against complacency in finishing polio in the country as there are still risks of circulation and re-infection.
Eradicating polio depends on reaching every child with vaccines, whether through campaigns or routine immunization systems. Nigeria introduced IPV in mass polio campaigns in 2014 with more than 3 million doses administered to children 14 weeks to 59 months of age in high risk areas. There are significant positive trends in improving routine immunization coverage with the reported OPV3 coverage of 67% in 2013 compared with 54% in 2010. However, this is still well below the goal of reaching at least 80% of children with reliable routine immunization systems.
While the programme has made significant progress against polio in Nigeria, continuing to strengthen routine immunization and health systems will be crucial to maintain and magnify the gains of recent years.
2015 marks the year of one of the largest globally-coordinated vaccine introduction projects in history. Inactivated polio vaccine (IPV) will be introduced into more than 120 countries currently using only oral polio vaccine (OPV), in advance of the phased removal of OPVs in 2016. While OPV is extremely safe and has led the world to the threshold of being polio-free, on very rare occasions, its use can lead to vaccine-associated cases. For this reason, the global eradication of polio requires the cessation of all OPV use, once polio has been eradicated. IPV will at that time be the only option for countries to maintain immunity levels.
The global IPV introduction effort got underway in late 2014 – the Philippines, Vietnam and Tunisia just some of the countries introducing IPV, with countries across Asia-Pacific scheduled to follow in the first few months of 2015. The world is closely watching the experiences of introducing this vaccine in the Western Pacific, as this Region has a long history of leadership on polio eradication. The successful strategies first developed, trialled and taken to scale here are helping inform the eradication strategies in the remaining polio-affected countries of the world.
Now, the Region is again showing its leadership, and lessons learned here will help inform countries’ introduction plans elsewhere. The aim is to ensure that all children – no matter where they live – can be protected from lifelong polio paralysis. Because introducing a new vaccine into the routine immunization programme is no easy feat, it’s also about getting vaccines to the right place, at the right time, in the right condition.
The successful introduction of IPV in countries such as Nepal, Philippines and Vietnam, supported by WHO and UNICEF, shows that high level political commitment is a critical factor, filtering through to bolster many aspects of the programme. In all three countries, cold-chain capacity was reviewed and expanded ahead of the introductions, health workers were trained and equipped with updated data collection tools, and communities mobilized.
The introduction of IPV is also being used as an opportunity to evaluate broader routine immunization services in targeted countries, and to identify potential operational gaps which can now be addressed. For example, countries are taking advantage of the focus on IPV introduction to adapt community awareness materials, to update registers and forms comprehensively, and to expand health worker trainings. Such system strengthening efforts are helping to ensure that all children are not only protected by IPV against polio, but indeed will be even more comprehensively reached with all vaccine-preventable diseases.
All of this is part of the comprehensive Polio Endgame Plan, designed to secure a lasting polio-free world by 2018. Implementation of the Endgame Plan would not be possible without the critical and ongoing support of the international development community, including Australia, Japan, Norway, the United Kingdom, the Bill & Melinda Gates Foundation and Rotary International. Without these vital contributions, activities outlined in the Polio Endgame Plan could not be financed, and could not be implemented. It will ensure that no child will ever again be paralysed by polio, and that the world can reap savings upwards of US$50 billion over the next 20 years (mostly in developing countries).
It is a perfect example of aid dollars in action – helping secure a lasting polio-free world, that will be a gift for all future generations to come.
The Convention of the Rights of the Child, which marks its 25th anniversary on the 20th November, defines the right of each child to survive and develop to their full potential.
Polio is a virus that causes irreversible paralysis, mostly to children. Before the first vaccine was developed in the 1950s, hundreds of thousands of children around the world were left unable to walk every year. With no cure, the threat of polio was a well-known source of fear for parents everywhere.
In 2014, polio has been dramatically reduced, but still circulates in geographically restricted areas of the world where insecurity prevents health workers to reach children with the vaccine. It has become an indicator of poverty, circulating where health systems are weak and where insecurity leaves children vulnerable, unprotected by the services they have the right to be provided with. That children anywhere in the world continue to be paralysed by this easily preventable virus is an inexcusable violation of the right of children to survive and develop to their full potential.
In North Waziristan, Pakistan, bans on immunization have meant that children have gone without access to polio vaccines since July 2012. North Waziristan is one of the final reservoirs of the virus. “The militants banned vaccination in their strongholds and would punish anyone in public if they were found vaccinating children,” said Salman Shah, a boy in his teens, whose studies in Political Science were interrupted by the unrest.
This summer, military campaigns in North Waziristan caused over a million people from North Waziristan to leave the area to protect their families. As unvaccinated people moved out of the area, the fear grew that this would offer the virus a chance to regain hold in other areas of the country. However, the government of Pakistan and the partners of the Global Polio Eradication Initiative, including WHO, have taken steps to seize the opportunity to reach displaced families at permanent vaccination points as they leave North Waziristan, and in the host communities in which they settle.
In Karak district, where many displaced families are settling, the provincial government is seizing the opportunity to protect every child with the crucial drops of oral polio vaccine. Doctors are going from door to door as part of health teams to vaccinate children free of cost. Noor Wali, a father who was displaced with his 7 children, expressed his gratitude that the government was finally able to reach his family with essential services. He said, “It is so important for us to shield our children from polio and other diseases.” His two youngest children, Noorul Amin and Robina, are finally protected against a disease that has been a severe threat to them since health workers stopped being able to reach their village 4 years ago.
The World Health Organisation has been crucial in ensuring that the displacement of families from North Waziristan was seized as an opportunity. Dr Margaret Chan, the Director-General of WHO, championed the importance of WHO’s role in the field of human rights: “The world needs a global health guardian, a custodian of values, a protector and defender of health, including the right to health.” By working for the past months to reach every family leaving North Waziristan, WHO has helped to ensure that over half a million children have been vaccinated against polio. In supporting governments to do everything they can to prevent life threatening diseases such as polio, WHO plays a crucial role in enabling children to survive and develop to their full potential.
Habib Ur Rehman, the father of 5 children who have now been protected with the vaccine, said: “In Darpakhel, vaccination activities took place under a cloud of fear. But the situation was worse in adjoining areas where vaccination activities were suspended. People have had to suffer a lot. I believe vaccination is the only way to prevent these life threatening diseases.”
17 July 2014 – The displacement of more than 900,000 people from North Waziristan in Pakistan’s Federally Administered Tribal Areas (FATA) increases the risk that polio will spread, as the virus travels with people as they move out to other parts of the country. Due to a ban on polio vaccination since June 2012, the area has suffered 55 of the country’s 94 cases in 2014.
However, this displacement also creates an important opportunity. For the first time in more than two years, vaccinators can reach large numbers of children who could not previously get vaccine.
Between 21 May and 15 July, 406,051 doses of oral polio vaccine were administered at vaccination points set up along major transit routes on the way out of North Waziristan. Emergency vaccination campaigns have also been held in surrounding areas, including weekly activities in parts of Khyber Pakhtunkhwa and FATA. This week’s campaign was reported to have reached almost 550,000 children.
Afghanistan is also doing its part to protect both the displaced and host communities against polio. More than 35,000 displaced children under the age of 10 are reported to have received a dose of oral polio vaccine as they entered the Afghan provinces of Paktyka and Khost
More than 42,000 children were vaccinated by the FATA Administration during a two-day campaign with the financial support of the United Arab Emirates and the protection of security forces. It was for the first time since 2009 that a comprehensive campaign could be conducted here, due to military operations and insecurity.
There were no security incidents during the campaign and according to preliminary reports, the demand from the community and the acceptance of vaccine was very high with excellent overall coverage. This opportunity allowed health officials to assess other critical health needs of the population, and to respond to the Leishmaniasis outbreak.
During the next three weeks, three more similar campaigns will be conducted on a weekly basis.
The World Health Organization (WHO) is taking immediate steps to assess the public health benefits of tightening the application of polio vaccination recommendations for travellers from polio-infected areas. These steps are being taken in response to a request by WHO Member States convening at the organization’s Executive Board (EB) in January 2014.
This request of Member States reflects growing concern about the substantial international spread of polio from key infected areas in 2013. Last year, poliovirus originating from polio-endemic countries resulted in major outbreaks in the Horn of Africa and the Middle East. Some WHO Member States, including the Kingdom of Saudi Arabia, already require that travellers from polio-affected areas show proof of vaccination before they are issued entry visas.
As an immediate first step, WHO convened the independent Polio Working Group of the Strategic Advisory Group of Experts on immunization (SAGE) on 5-6 February 2014 to review existing definitions for polio-infected areas, update WHO’s polio vaccination recommendations for travellers from infected areas based on new information and evidence, and identify potential operational and other considerations that would need to be evaluated in tightening the international application of such recommendations. These updated policy recommendations are summarized in the new ‘Polio vaccines: WHO position paper, January 2014’, published in the WHO Weekly Epidemiologic Record on 28 February 2014 and will be published in full in the 2014 edition of WHO’s International Travel and Health in April 2014.
The deliberations and recommendations of the SAGE Polio Working Group will be discussed by SAGE in April 2014 and inform deliberations under the International Health Regulations concerning potential measures for reducing the international spread of polioviruses.
Courageous Pakistani mothers, like polio survivor Saima, are key to ending polio’s paralysing effects on children for good – not just in Pakistan, but all over the world.
Polio survivor Saimal Liaqat UNICEF Pakistan
This is not the first time Saima Liaqat has shown her courage.
Stricken by polio at age two, Saima was partially paralysed. Yet already, as a girl, she refused to let the disease get the best of her. She limped down the long dusty road to school so often, and studied so hard, that she became the first woman in her family to go to college.
Saima’s native Pakistan is one of only three countries on earth where polio is still endemic; Afghanistan and Nigeria are the others. Polio, as Saima knows all too well, attacks children with devastating, paralyzing results. The disease can be prevented by swallowing two drops of polio vaccine. Yet in small pockets of Pakistan, some parents have refused to allow their children to take the vaccine. And the recent polio outbreak in Syria is a reminder that, whenever children anywhere go unvaccinated, every child is at risk.
It will take courage – and the efforts of unstoppable women like Saima – to rid Pakistan, and the world, of polio once and for all.
In this TV spot, which has reached nearly 70 million viewers across Pakistan, Saima stands up, once again, to the disease that left her partially paralyzed. Now a wife and mother of three herself, she shares her story as a polio survivor and urges parents to accept the vaccine:
“I think parents become their child’s worst enemy when they don’t vaccinate them. You will regret it, if something happens to your child.”
As a mother, Saima has always refused to let polio hold her back.
“When my children were young, we would go to the park. I would play all sorts of games with them… badminton, cricket. I would take care of them all by myself,” says Saima. “I wanted to prove to people that I was still my own person.” Her courageous example has not been lost on Saima’s own children.
“I wanted to become a doctor so I could treat my mother,” says her daughter, Hamna. “Now I know this disease has no cure.”
Saima has taught her daughter to focus on what can be changed, rather than on regrets from the past. Still, even as Hamna speaks of the polio vaccine that can free children all over the world from this tragic disease, her voice is wistful. It’s hard not to wonder how different her mother’s life might have been – if only she had swallowed those two tiny drops of vaccine. Says Hamna:
“I wish my grandparents had given my mother polio drops, so she would not be in so much pain today.”
Qari Aqeel, Teacher at a Madrassa in Karachi UNICEF Pakistan
“I kneel before Allah. But I am unable to stand on my feet before any man.”
In Pakistan, Qari Aqeel teaches children the fundamentals of Islam and the Holy Quran. He also tells them, from his own painful experience, what it is like to live with polio.
A teacher at a Madrassa in one of Karachi’s poorest areas, Aqeel talks to parents and children about the importance of vaccination from an Islamic perspective. In this moving video, Aqeel takes the spotlight away from the politics and misunderstandings that can too often muddy the dialogue about polio vaccination. He brings the focus firmly back to what most matters: the heart-wrenching effects that polio can have on a young life – and the imperative to end this tragic and preventable disease, once and for all.
As a child, Aqeel so longed for an education and a connection to God that he braved pushing, shoving and being spit at by other children as he made his way on crutches through the streets of Karachi to learn at the local seminary.
Today, as a grown man, Aqeel might be speaking of his newly-acquired wheelchair, when he says:
“Now, when they push me, I just go faster.”
Or he might be speaking of the struggle to end polio itself.
Grand Imam of Al-Azhar receiving Muslim Scholars to discuss children rights to be protected by vaccination WHO/EMRO
Cairo, 7 March 2013 – The Grand Imam of Al-Azhar, Doctor Ahmad Al Tayyeb, today called for the protection of Muslim children against poliovirus transmission by ensuring they receive the required polio vaccine. He stressed the importance of increasing the awareness of the correct Islamic teachings on the subject to combat all deformed and false beliefs, and confirmed that Al-Azhar is ready to continue to exert all efforts to enlighten Muslim individuals and communities about the rights of children to be protected against polio and all other diseases and the obligation of all muslims to ensure that their children are protected. “Crippled children lead to a crippled Muslim Ummah” Dr Al-Tayyeb warned.
This was announced today at a meeting held at Al-Azhar during which the Grand Imam met with Muslim scholars from several countries. The scholars expressed their solidarity with the children of the Islamic world and reaffirmed their resolve to support the people, health workers and governments of the three countries where polio is not yet eradicated, namely Afghanistan, Nigeria and Pakistan.
The Global Polio Eradication Initiative, launched in 1988 by the health ministers of the Member States of the World Health Organization, has been successful in stopping the transmission of this crippling disease in all but these three countries of the world. Except for in Afghanistan, Nigeria and Pakistan, Muslim communities and countries everywhere have eradicated polio, including 54 out of 57 member states of the Organization of Islamic Cooperation (OIC) that have successfully interrupted transmission of wild poliovirus. This has been achieved through the application of proven eradication strategies, the administration of the safe oral polio vaccine and with financial and political support from the Islamic world.
Recognizing with grave concern the ongoing transmission of wild poliovirus in parts of Afghanistan, Nigeria and Pakistan, and the remaining political, cultural, societal and security challenges preventing all children in these areas from being vaccinated against polio, and in particular the tragic and deadly attacks against frontline health workers in parts of Pakistan and Nigeria in the past three months, Islamic scholars from several countries are meeting for two days in Cairo from 6–7 March to discuss the major obstacles preventing these countries from stopping polio transmission and trying to reach a consensus on how the Islamic leadership can help Muslim communities to overcome these barriers and ensure protection for all Muslim children.
11 February 2013 – In Egypt, wild poliovirus type 1 (WPV1) was isolated from sewage samples collected on 2 and 6 December 2012 in two areas of greater Cairo. Virus has been detected in sewage only; no case of paralytic polio has been reported. Genetic sequencing shows that the virus strains are closely related to virus from northern Sindh, Pakistan. Pakistan is one of three countries worldwide affected by ongoing indigenous transmission of WPV (together with Nigeria and Afghanistan). The isolates were detected through routine environmental surveillance in Egypt that involves regular testing of sewage water from multiple sites.
Following detection of these isolates, the Government of Egypt is implementing a comprehensive response in line with international outbreak response guidelines issued by the World Health Assembly (WHA) in Resolution WHA59.1. On 2-6 February, supplementary immunization activities (SIAs) were conducted in the two areas of Cairo from where the environmental samples had been collected, reaching more than 155,000 children with trivalent oral polio vaccine (OPV). In early March, SIAs are planned across Cairo to reach three million children with monovalent OPV type 1, to be followed in April by nationwide SIAs targeting 12 million children with trivalent OPV. A joint national and international team of epidemiologists and public health experts is assisting in the investigations, helping plan response activities and supporting active searches for any potential cases of paralytic polio.
This event confirms ongoing international spread of a pathogen (WPV) slated for eradication. In May 2012, the completion of polio eradication was declared a programmatic emergency for global public health by the WHA in Resolution WHA65.5. Based on the history of previous importations to Egypt and the ongoing response, the World Health Organization (WHO) assesses the risk of further international spread of these virus strains from Egypt as moderate; and, of further international spread of WPV from Pakistan as high. In 2011, WPV from Pakistan spread internationally to China, causing an outbreak in the country’s western Xinjiang province, resulting in 21 cases.
It is important that all countries, in particular those with frequent travel and contacts with polio-infected countries, strengthen surveillance for cases of acute flaccid paralysis (AFP), in order to rapidly detect any new poliovirus importations and facilitate a rapid response. Countries should also analyze routine immunization coverage data to identify any subnational gaps in population immunity to guide catch-up immunization activities and thereby minimize the consequences of any new virus introduction. Priority should be given to areas at high-risk of importations and where OPV3/DPT3 coverage is <80%.
Egypt stopped transmission of indigenous WPV, with its last case in May 2004. The environmental samples which yielded these positive results were collected in December 2012. Previous to this, the last environmental sample which had tested positive for WPV was related to virus from the Sudan, in December 2010.
GENEVA/NEW YORK, 19 December 2012 – The World Health Organization (WHO) and UNICEF join the Government of Pakistan and the provinces of Sindh and Khyber Pakhtunkhwa in condemning the multiple attacks that have killed nine health workers this week.
The attacks took place in several locations in Pakistan – Gadap, Landi, Baldia and Orangi towns of Karachi city, Sindh Province and Peshawar, Khyber Pakhtunkhwa Province. Those killed were among thousands who work selflessly across Pakistan to eradicate polio.
The Government of Pakistan and the affected provinces have temporarily suspended the vaccination campaigns due to concerns over safety of health workers.
Such attacks deprive Pakistan’s most vulnerable populations – especially children – of basic life-saving health interventions. We call on the leaders of the affected communities and everyone concerned to do their utmost to protect health workers and create a secure environment so that we can meet the health needs of the children of Pakistan.
WHO, UNICEF and all their partners in Pakistan and globally express their deepest sympathy to the families of the health workers. We remain committed to supporting the Government of Pakistan and the people of Pakistan in their efforts to rid the country of polio and other diseases.
17 December 2012 – Last week, Chad passed six months without a single case of wild poliovirus (WPV). But while this would normally be cause for cheer, there are signs – including the presence of circulating vaccine-derived polioviruses – that children are continuing to miss out on the vaccine.
Much has been written lately about the outbreaks of circulating vaccine-derived polioviruses (cVDPVs) currently affecting Chad, Nigeria, the Somalia/Kenya border and Pakistan, and their implications for the global polio eradication effort. But what exactly is a circulating VDPV? How do they occur? And how can they be prevented?
Eventually use of OPV must stop
A circulating VDPV is an extremely rare strain of polio genetically changed from its original, weakened strain contained in oral polio vaccine (OPV). Read More
Circulating VDPVs must be responded to in the same manner as WPV outbreaks. But once wild polioviruses have been successfully eradicated, OPV must be phased out, as the public health benefits of OPV will no longer outweigh the very small risk of its continued use.
Trivalent oral polio vaccine (tOPV) has long been the vaccine of choice for routine immunization in many parts of the world – it was the vaccine that eradicated wild poliovirus type 2, after all. But while wild type 2 is gone, 90% of circulating vaccine-derived poliovirus cases are of type 2.
The bivalent oral polio vaccine (bOPV) – which does not contain type 2 – is more effective against the two remaining wild poliovirus types. So the world’s guiding body for vaccination policy, the SAGE or Strategic Advisory Group of Experts on immunization has called for a globally synchronized withdrawal of type 2-containing OPV – necessitating a switch from tOPV to bOPV in routine immunization programs. In its landmark decision, the SAGE also recommended that all countries introduce at least a single dose of inactivated polio vaccine to mitigate the risks associated with this switch. This switch is an integral part of the new Polio Eradication and Endgame Strategy currently under development.
How poliovirus behaves
To understand how cVDPVs occur, one should look first at how a wild poliovirus (WPV) behaves.
When a child is infected by a WPV, the virus replicates in the child’s intestine, and then enters the bloodstream through cells lining the intestine, where it can spread to the spinal cord and cause paralysis. The virus is also excreted during this period, spreading to other children in the community, particularly in areas with poor sanitation. If a sufficient number of children are fully immunized against polio, this WPV is unable to find susceptible children to infect, and dies out.
Immunization with OPV occurs in much the same manner. When a child is immunized with OPV, the weakened vaccine-virus also replicates in the intestine (developing immunity by building up antibodies in the intestine) before entering the child’s bloodstream through cells lining the intestine (further developing immunity by building up antibodies in the blood stream). Like WPVs, the vaccine-virus is also excreted during this period. Importantly, as it is excreted, this vaccine-virus is no longer the same as the vaccine-virus originally contained in the OPV dose, as it genetically alters from its original form as it replicates. This vaccine-virus can spread in the immediate community – this is beneficial, as this way it ‘passively’ immunizes other children. Once it no longer finds unimmunized children, this vaccine-virus rapidly dies out.
Circulating VDPVs: Causing cases in areas where populations are under-immunized
On very rare occasions, if a population is seriously under-immunized, an excreted vaccine-virus can find susceptible children and begin to circulate beyond the immediate household into the broader community, for an extended period of time. The longer it is allowed to survive this way, the more genetic changes it undergoes as it replicates, and eventually it can revert to the point that it can cause paralysis. Circulating VDPVs are viruses that have gone through this process.
This takes a long time. Generally, the strain will have been allowed to circulate in an un- or under-immunized population for a period of at least 12 months. Circulating VDPVs occur when routine or supplementary immunization activities (SIAs) are poorly conducted and a population is left susceptible to poliovirus, whether from VDPVs or WPVs. Hence, the problem is not with the vaccine itself, but with low vaccination coverage.
If a population is fully immunized, they will be protected against both VDPVs and WPVs.
Circulating VDPV events are extremely rare. Over the past 10 years, more than 10 billion doses of OPV have been administered to more than 2.5 billion children, preventing more than 650,000 polio cases every single year. In that same period, only 21 cVDPV episodes are known to have occurred, resulting in 622 cases.
President Karzai of Afghanistan, President Zardari of Pakistan, B. Gates, Gates Foundation, polio survivor R. Ferris, President Jonathan of Nigeria, W.J. Wilkinson, chair Rotary Foundation Trustees, and Dr M.Chan, Girector-General of WHOStuart Ramson/Insider Images
UNITED NATIONS, 27 September 2012 – In a display of solidarity, leaders from around the world today vowed to capitalize on progress achieved this year and to step up the fight to eradicate polio. Heads of state from Afghanistan, Nigeria and Pakistan stood alongside donor government officials and new donors from the public and private sector to outline what is needed to stamp out this disease forever: long-term commitment of resources, applying innovative best practices, and continued leadership and accountability at all levels of government in the endemic countries.
“This decisive moment is a matter of health and justice. Every child should have the right to start life with equal protection from this disease. That’s why I have made eradicating polio a top priority for my second term as Secretary-General,” said UN Secretary-General Ban Ki-moon.
Polio is a vaccine-preventable disease that is more than 99 percent eliminated from the world. Today, there are the fewest number of polio cases in the fewest districts in the fewest countries than at any time in history. In 1988, when the global fight against polio began, there were 125 countries where polio raged. Today, there are only three: Nigeria, Pakistan and Afghanistan. India, long-regarded as the nation facing the greatest challenges to eradication, has been polio-free for more than 18 months.
“The evidence is clear: if we all do our part, we can and will end this disease. But we must act quickly and give ourselves the very best chance to succeed,” said Bill Gates, co-chair of the Bill & Melinda Gates Foundation, one of the leading donors to the Global Polio Eradication Initiative (GPEI). “When we defeat polio, it will motivate us to aim for other great health and development milestones.”
Earlier this year, at the World Health Assembly, 194 member states declared the completion of polio eradication to be a “programmatic emergency for global public health.” In order to look beyond short-term challenges, however, GPEI is developing a long-term roadmap for ending polio. The strategy also will ensure that the legacy of investments in polio supports other vaccine-preventable disease goals.
“Failure to eradicate polio is unforgiveable, forever. Failure is not an option. No single one of us can bring this long, hard drive over the last hurdle. But together we can,” said Dr. Margaret Chan, Director-General of the World Health Organization.
Ending polio is an important early milestone in the Decade of Vaccines, a global vision and commitment to reach all children with the vaccines they need. A polio-free world also will lay the foundation for a better public health system that provides critical health services for children in the poorest and most inaccessible places.
“Together we can make history by eradicating polio – thanks mostly to the heroes in the field who risk their lives, every day, to deliver vaccines to children in some of the most dangerous parts of the world,” said Anthony Lake, UNICEF Executive Director.
The high-level event, “Our Commitment to the Next Generation: The Legacy of a Polio-free World,” featured opening remarks from UN Secretary-General Ban Ki-moon and was moderated by Senator Timothy E. Wirth, president of the UN Foundation.
Speakers included leaders of the three polio-endemic countries: President Hamid Karzai, Islamic Republic of Afghanistan; President Goodluck Jonathan, Federal Republic of Nigeria; and President Asif Ali Zardari, Islamic Republic of Pakistan. Earlier this year, these leaders launched national emergency plans to stop transmission of polio in their countries.
“Governments need to step up and honor their commitments to polio eradication if we are to achieve a polio-free world,” said Wilfrid J. Wilkinson, Chair of Rotary Foundation Trustees. “We must seize the advantage by acting immediately, or risk breaking our pledge to the world’s children.” Rotary International, which already has contributed US$1.2 billion to polio eradication, announced additional funding of $75 million over three years to GPEI.
Australian Prime Minister Julia Gillard reinforced Australia’s commitment and called on the Commonwealth to do its part. Last October, Australia committed $50M during the Commonwealth Heads of Government Meeting. Also speaking was Kathleen Sebelius, Secretary of Health and Human Services for the United States. The United States has been the leading donor to the GPEI and provides technical support through the US Centers for Disease Control & Prevention (CDC).
“We have been given the unique opportunity to end polio and provide a lasting legacy for the world’s children,” said Dr. Thomas Frieden, Director of the CDC. “Together we must strive to achieve this important global milestone.”
The Islamic Development Bank, a new donor to the polio eradication effort, announced a three-year $227 million financing package to Pakistan which will cover the majority of the country’s polio vaccination campaign costs. It also announced a $3 million grant for polio eradication activities in Afghanistan.
Additional leaders pledged new and continued commitment to polio eradication. These included:
H.E. Julian Fantino, Minister, International Cooperation, Canada, who announced an initiative to engage civil society to match funds to GPEI;
Rt. Hon. Alan Duncan, Minister of State, International Development, United Kingdom, whose government committed an additional £25M to polio eradication in 2012;
Mr. Sandro Rosell, President, Football Club Barcelona (FCB) and FCB Foundation, who announced the club’s engagement on the polio issue in collaboration with the Gates Foundation and Etisalat, the largest telecomm operator in the Middle East;
Ms. Aseefa Bhutto Zardari, Pakistan’s Goodwill Ambassador on Polio Eradication.
On 29 September, the Global Poverty Project, a campaign group aimed at ending extreme poverty, will host the Global Citizen Festival, a concert bringing together more than 60,000 people in New York’s Central Park with the aim of inspiring a global movement to voice support for eradicating polio and ending extreme poverty.
The Global Polio Eradication Initiative (GPEI), launched in 1988, is spearheaded by national governments, the World Health Organization (WHO), Rotary International, the US Centers for Disease Control and Prevention (CDC) and UNICEF, and supported by key partners including the Bill & Melinda Gates Foundation.
Since its launch, the incidence of polio has been reduced by more than 99 percent. In 1988, more than 350,000 children were paralyzed each year in more than 125 endemic countries. In 2012, 145 new cases have been reported, and only three countries remain endemic: Nigeria, Pakistan and Afghanistan.
Bill & Melinda Gates Foundation: media@gatesfoundation.org, +1 206 709 3400
Rotary International: Petina Dixon-Jenkins. petina.dixon@rotary.org, +1 847 866 3054
UNICEF: Christian Moen. cmoen@unicef.org, +1 212 326 7516 or mobile +1 917 299 1041
US CDC: Alan Janssen. axj3@cdc.gov, +1 404 639 8517
WHO: Oliver Rosenbauer, Communications Officer, WHO, rosenbauero@who.int; +41 22 791 3832
Shahid Afridi meets the two brothers Najibullah and Naqeebullah, both of whom have polio. Rotary Pakistan
19 September – With such a focus on vaccinating the last one per cent of the world’s children, it is easy to forget the work that is being done to help those children who have survived the incurably crippling poliovirus. For Najeebullah (18) and Naqeebullah (15), two brothers living in the polio sanctuary of Gadap Town, however, the Rotary Club of Karachi has been instrumental in enabling them to best overcome the virus and meet Pakistan’s cricketing legend, Shahid Afridi.
The two brothers, originally from Mazhar-e-Shareef in Northern Afghanistan, were afflicted with polio when they were 14 and 11 years of age respectively. The third child in the family has been vaccinated against the virus to ensure he does not suffer the same fate as his brothers.
After receiving treatment and therapy for 40 days at a rehabilitation hospital in Saddar Town, Karachi, the older brothers regained some mobility in their hands and legs. At Rotary Club of Karachi’s artificial Limb Project Community Centre, they were both fitted with prosthetic limbs free of charge thanks to the donations of Pakistani Rotarians.
The 5000 artificial limbs and calipers the centre provides free of cost every year to polio victims and amputees is not the only service offered by Rotary’s Community Centre. There is also a permanent limbs workshop at the centre, a gym, an eye clinic, a permanent immunization centre for the surrounding population, and activities such as computer classes.
At the end of July, the brothers were invited to a Polio workshop in Karachi, organized to inform Presidents of Rotary Clubs in Karachi of the current polio status in Pakistan. Here, they shook hands with Pakistan hero, Shahid Afridi. According to ESPN, ‘cricket never has and never will see another’ like Afridi. Indeed, ‘Boom Boom’ Afridi has already vaccinated children personally as part of the promotional campaign, which has seen the cricketer’s face displayed on the side of hundreds of rickshaws which roam all areas of Karachi.
Enlisting the support of religious leaders increases the success of vaccination campaigns. WHO/JM Giboux
28 August 2012 – On the weekend of 31 August, prominent religious leaders from seven major sects in Pakistan who are supportive of polio eradication will travel to Saudi Arabia to attend a Conference on Children and Islam. These leaders represent religious leaders across Pakistan who are working to mobilise the community in support of polio vaccination and overcome widespread rumours that polio vaccination is anti-Islamic.
Refusals, and religious refusals in particular, are rare in Pakistan, with an average of only two per cent of the population refusing the vaccination during each campaign. However, in order to reach every last child, this is too high a figure, and one which polio staff and religious leaders are working hard to bring down.
When volunteers visit households on their vaccination rounds, they can find some families who persistently refuse to have their child vaccinated even when they are re-visited several times during the campaign. When parents cite religious reasons for refusing the oral polio vaccine (OPV), it is often due to a perception instilled by the teachings of an influential religious figure who has expressed reservations about the safety of the vaccine, or even the motives of the polio programme in general.
In some areas, localised resistance has been mobilised around the belief that the polio programme is a western plot to sterilise Muslims, or that the contents of the vaccine are not halal.
It is critical not only to provide correct information about the importance of polio vaccination, but also to help mobilise religious leaders to become advocates for the cause. In the high-risk areas of Pakistan, 1,085 social mobilisers are working to transform community perceptions.
Social mobilisers explain and dispel persistent myths about the vaccine and use passages from the Qur’an and the Hadith to emphasize the importance of children’s health . Fatwas from highly respected Islamic clerics also help to demonstrate that polio vaccine is not anti-Islamic. Once on board, religious leaders have the influence to successfully convince their followers to vaccinate their children and can call families from their mosques to vaccination points.
One such religious leader is the uncle of two-year-old Mehrama, from Quetta in Balochistan, who was diagnosed with polio in June this year. In this case the turning point came when he was shown a pro-vaccine video of Maulana Rafi Usmani, an influential religious scholar from his own Deobandi sect. In the July campaign, this influential leader inaugurated the vaccination campaign in his Union Council by vaccinating his one-year-old son and convincing eight other families who had previously persistently refused to vaccinate their children.
In areas that don’t have access to television or radio, the inter-personal connection that social mobilizers are able to establish is crucial: with persistent and appropriate interventions, one-to-one communication can not only change beliefs, but also behaviour. Across the 33 high risk districts in Pakistan, 1 out of every 2 parents who initially refuse the vaccine are later convinced of the importance of vaccination, according to UNICEF’s communications data. Thanks to the work of religious leaders, and increased commitment from the whole country towards the eradication goal, the total number of polio cases in Balochistan in the first half of this year was 3 compared to 19 by the same point in 2011.
There remains a lot of work to do, however. Children in Quetta Block continue to be missed – 16 % in Pishin in the March 2012 immunisation campaign. With the help of religious leaders and civil society to establish polio vaccination as a universal social norm, however, more children will enjoy a polio-free future.
Melon growing family missed by vaccination campaigns highlights the necessity of improving micro plans. UNICEF / Pakistan
In the scenic Sanwan village, close to the Indus River in Thatta district, Sindh, melon growing is a common occupation for local farmers. Thirteen-month-old Sundar Lal’s family have been known for their melons for years. It takes three months to harvest the melons: “We have already gathered two crops and the final one will be ready in a month’s time,” Premi, Sundar Lal’s grandmother, explained. However, it is unlikely that Sundar will be able to play a role when he’s older in the harvesting of the melons: Sundar was diagnosed with polio in January of this year.
It is families such as Sundar’s that highlight the myriad logistical and operational challenges of nationwide vaccination campaigns.
The young boy got off to a difficult start in life, being born in an Internally Displaced Persons (IDP) camp after the 2010 floods in the Hyderabad district. Even so, his mother, Bhaga, was able to take Sundar for routine immunization at a nearby EPI centre. Polio drops, however, need to be administered at least four times and in places with poor sanitation, or a high incidence of malnutrition or diarrhoeal diseases, the vaccine can be less effective than elsewhere.
Because of this, supplementary immunization activities (SIAs) are used to boost the immunity of the population to as high a level as possible. However, an investigation into Sundar’s case showed that vaccination teams assigned to the area did not follow up after the child was registered as ‘not available’ during the campaign, citing fear of stray dogs loitering in the neighbourhood.
This was not the only flaw in the vaccination campaign which was supposed to reach Sundar. During the planning, three separate areas were reflected as one in the micro-plan and assigned to a single person, doubling the number of children for them to cover.
Although it is too late for Sundar, the Global Polio Eradication Initiative is moving faster to identify and solve these issues in order to ensure cases such as his do not happen again. For example, in West Africa, insecurity in Mali, the Sahel crisis and the upcoming rainy season have resulted in large scale population movements. Nevertheless, immunization campaigns continue to take place in refugee camps in countries bordering Mali, including in Mauritania and Burkina Faso, and in internally-displaced persons camps in Mali itself. Furthermore, population movements are actively tracked and mapped, with health posts set up at key border crossings, gathering sites and in hard-to reach areas.
Meanwhile in Pakistan, a WHO and UNICEF staff surge is actively reviewing vaccinator team performance and composition, improving micro-planning and fixing the ‘basics’ of good campaign operations. This new approach is already having an impact: there have only been two more cases of polio after Sundar in Sindh province for the first six months of this year, compared to 14 for the same period last year.
Mr. Muhammad Ishaq, during a SIA in Pakistan WHO Pakistan/Edda Salvatori
KARACHI/NEW YORK/GENEVA, 21 July 2012 – The World Health Organization (WHO) and UNICEF are deeply saddened by the killing of Mr. Muhammad Ishaq, a local community worker supported by WHO, who was part of the polio eradication initiative in Pakistan.
Mr. Ishaq was shot and killed in the Gadap town area of Karachi on Friday evening.
Polio immunization activities were suspended in this area of Karachi earlier this week after a shooting incident injured two WHO staff members who were supporting the implementation and monitoring of a vaccination campaign.
Until activities were suspended, Mr. Ishaq had worked with the national polio eradication effort as a Union Council Polio Worker for several months, helping to plan and implement vaccination campaigns to protect the most underserved and vulnerable children against this debilitating disease.
Because of the dedication of heroes like Mr. Ishaq, Pakistan is this year closer than ever to the eradication of polio. He was known for his dedication and diligence to immunize all children against polio.
Polio is a highly infectious disease caused by a virus that can cause permanent paralysis in a matter of hours. There is no cure, but there are safe and effective vaccines. Polio can be eradicated if every child is immunized until transmission stops worldwide.
Currently the disease remains endemic in only three countries: Pakistan, Afghanistan and Nigeria. Mr. Ishaq was one of the thousands of people across Pakistan who worked selflessly in the battle to eradicate polio.
WHO, UNICEF and all of the polio partners in Pakistan and globally express their deepest sympathy to his family for this tragic loss. The partners of the Global Polio Eradication Initiative remain committed to supporting the Government of Pakistan and the people of Pakistan in their efforts to eradicate this devastating disease.







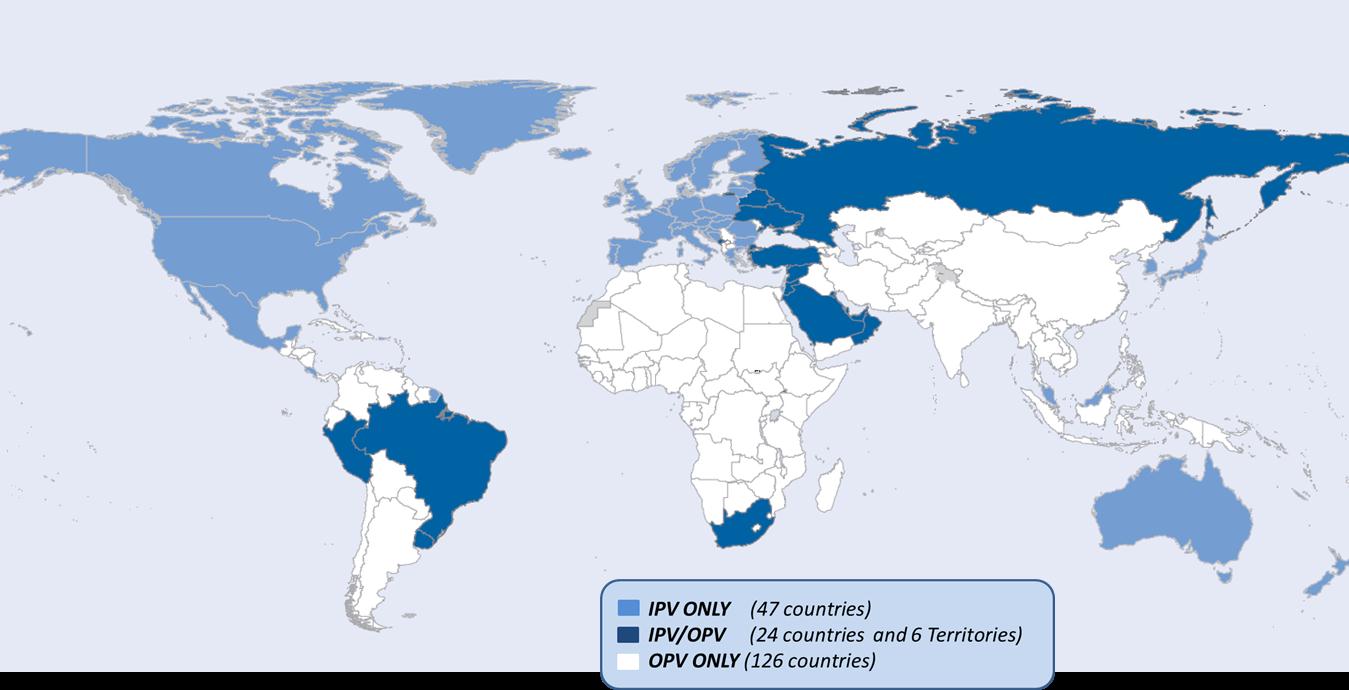
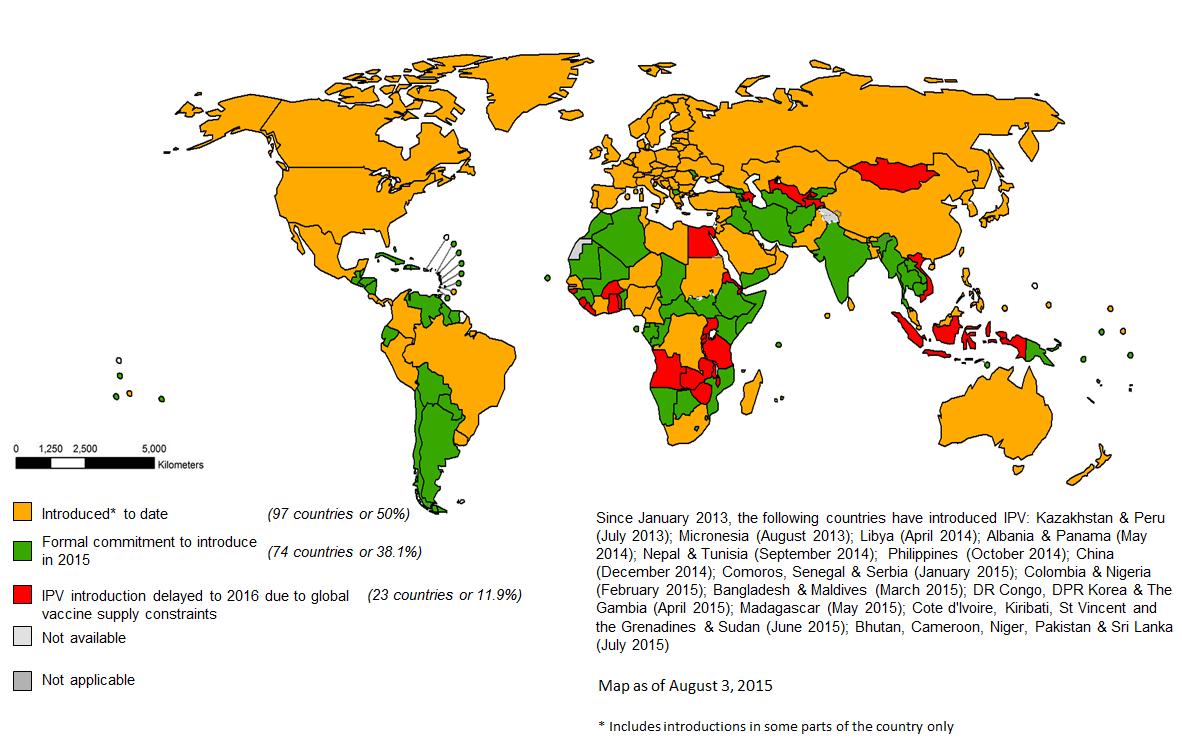












 Such attacks deprive Pakistan’s most vulnerable populations – especially children – of basic life-saving health interventions. We call on the leaders of the affected communities and everyone concerned to do their utmost to protect health workers and create a secure environment so that we can meet the health needs of the children of Pakistan.
Such attacks deprive Pakistan’s most vulnerable populations – especially children – of basic life-saving health interventions. We call on the leaders of the affected communities and everyone concerned to do their utmost to protect health workers and create a secure environment so that we can meet the health needs of the children of Pakistan.




