For Dr Tedros Adhanom Ghebreyesus, Director-General of WHO, the start to the new year was marked with a four-day visit to Afghanistan and Pakistan from 5-8 January. The visit came at the heels of his new role as the Chair of the Polio Oversight Board (POB) on 1 January, a committee which oversees and guides the Global Polio Eradication Initiative, signalling the Board’s utmost commitment towards eradication of polio for good.
Accompanied by WHO Regional Director for the Eastern Mediterranean Dr Ahmed Al-Mandhari, Dr Tedros’ well-knit, compact visit covered a lot of bases from field visits to high-level meetings with heads of state from both the countries, giving the POB an opportunity to see that while polio may still be in endemic in Afghanistan and Pakistan, but the process to achieve the goal of ending polio is not far from realization.
“We must all give our best on this last mile to eradicate polio once and for all. My wish for 2019 is for zero polio transmission. You have WHO’s full support to help reach every child and stop this virus for good,” Dr Tedros said.
During his first stop in Afghanistan on 5-6 January, Dr Tedros met with His Excellency President Dr Ashraf Ghani, His Excellency Chief Executive Dr Abdullah Abdullah, the Council of Ministers, representatives of key partners and nongovernmental organizations working in the field of public health. He also visited to the WHO-supported Trauma Care Hospital in Kabul.
In Pakistan on 7-8 January, Dr Tedros met with the Prime Mister Imran Khan, Federal Minister for National Health Regulations & Coordination Mr Aamer, Mehmood Kiani, Minister of Foreign Affairs and Federal Minister for Human Rights Dr Shireen Mazari.
Dr Tedros accompanied the President of Pakistan, Arif Alvi, to the launch of the first Pakistan Nursing and Midwifery Summit and the Nursing Now campaign. He also visited a basic health centre in Shah Allah Ditta where WHO signed an agreement with the Government of Pakistan to develop a model health care system for universal health coverage in Islamabad.
In the last mile of the polio eradication journey, Dr Tedros’ visit serves as a reminder that now more than ever we need to have social, political and global will to make polio the second human disease in history to be wiped from earth.
Front-line health workers and volunteers represent the backbone of the global polio eradication effort. As they work tirelessly to reach and vaccinate every last child against polio – often in remote, hard-to-reach or even dangerous areas – they are not only protecting children from the poliovirus, but also paving the way for other health programmes to reach the world’s most vulnerable children.
The Every Last Child project is a collection of over 30 stories and profiles from India, Pakistan and Afghanistan about the collective efforts of front-line health workers, governments and global health partners to protect children from the poliovirus in some of the world’s most challenging environments. These multimedia pieces illustrate the complexity and scale of polio eradication efforts in each of these key countries through in-depth narratives, compelling profiles and interactive visuals.
To end polio, the global polio programme must reach every last child and take bold steps to take the world across the finish line once and for all. Visit the Every Last Child project page to learn more about the history of these remarkable efforts, as well as stories of heroic front-line workers.
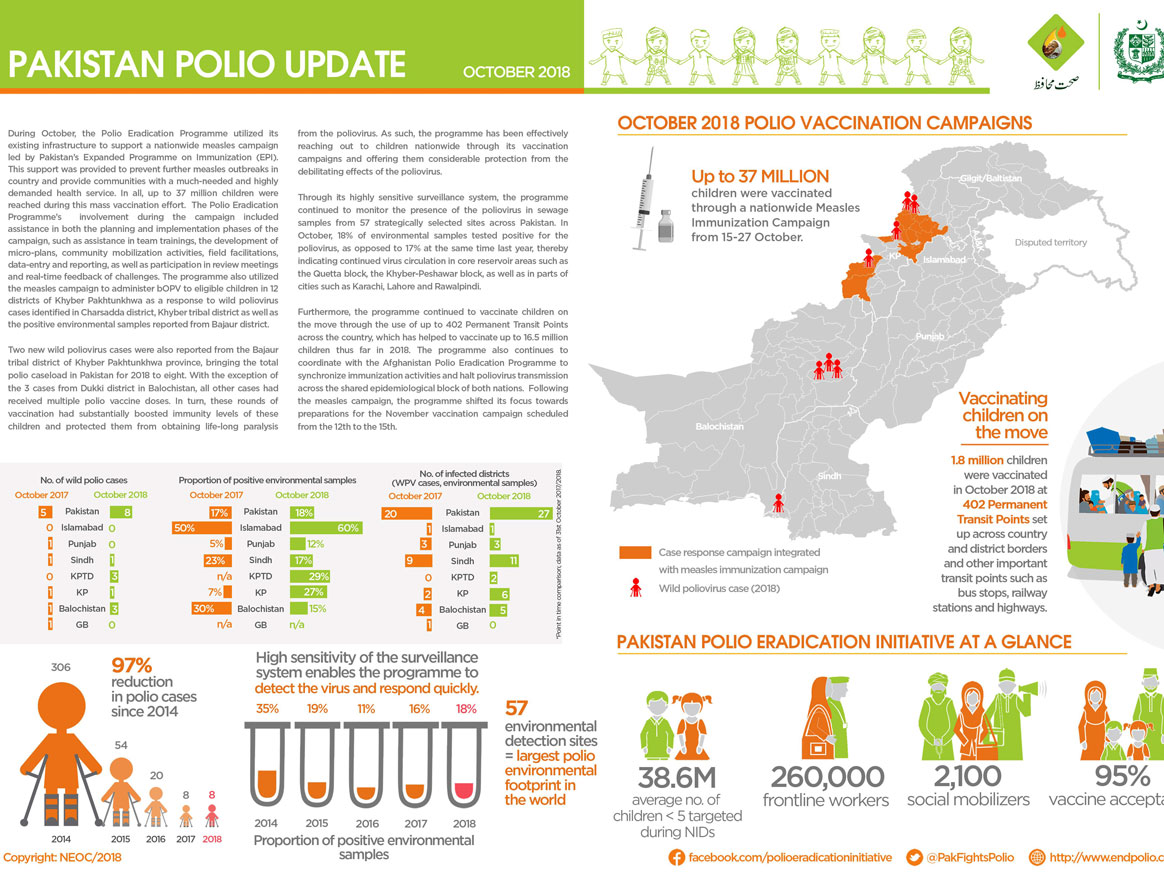
Pakistan’s routine immunization programme Expanded Programme on Immunization will carry out a nationwide measles vaccination campaign targeting around 31.8 million children aged 9-59 months from 15 to 27 October to respond to an ongoing measles outbreak in Pakistan. Over 30 000 measles cases have been reported this year, compared with around 24 000 cases in 2017.
Pakistan typically encounters a measles outbreak every 8 to 10 years, and the Federal Ministry of Health works proactively to stop these outbreaks with regular vaccination campaigns. Although the Polio Eradication Initiative and the Expanded Programme on Immunization are separate entities, they work together to improve immunization outcomes in Pakistan. Achieving strong essential immunization coverage is a critical step in bringing Pakistan closer to ending polio, and once this goal is reached, in maintaining polio-free status.
Many of the areas at highest risk for polio are also at high risk for measles. During the upcoming measles campaign, the polio programme will lend its human, physical and operational resources, knowledge and expertise to achieve the highest possible measles immunization coverage across the country.
Reaching more children through stronger collaboration
The collaboration between polio and routine immunization programmes has made a significant difference in vaccination efforts across dense urban environments as well as scattered rural settings. A key factor for success has been the polio programme’s highly-skilled workforce of community vaccinators, front-line health workers and social mobilizers.
During every round of country-wide polio vaccination campaigns, around 260 000 front-line health workers vaccinate more than 38 million children under the age of 5 across Pakistan. With vital on-the-ground experience in some of the most challenging settings, they are determined to ensure that the lessons learned in polio are transferred to other health interventions.
“Our front-line workers have built strong rapport in their respective communities,” said Dr. Rana Safdar, coordinator of the National Emergency Operation Centre (NEOC) for polio eradication and member of the National Measles Steering Committee.
“They understand the dynamics of the population, even as they relate to children, not only at the district level but also at the Union Council and village level. This indigenous knowledge coupled with community trust can definitely play an instrumental role for other health interventions.”
Unlike polio eradication activities, measles immunization is not carried out from door-to-door but at fixed centres at health facilities as well as through outreach sessions within communities. Children are mobilized to the vaccination sites where trained healthcare professionals administer the injectable measles vaccine. The deep local knowledge polio workers have developed and the trust they have built with their communities is vital in mobilizing caregivers to take their children for measles immunizations at nearby vaccination sites.
“The strong collaboration between the two programmes has helped us vaccinate more children. Our joint efforts are geared towards reaching every last child and they have shown significant progress so far. We hope that our synergized efforts during the upcoming measles campaign will lead us to reach every child in the target population with measles vaccine,” said Dr. Tahir Abbas Malik, from the Pakistan polio programme.
“For polio, these coordinated efforts have paved the way for increasing the coverage of persistently missed children, especially those who are on the move or reside in hard-to-reach areas. Similarly, integrated micro planning, monitoring and reporting of children who have not received essential immunization have been instrumental for achieving gains for routine immunization through enhanced coverage,” said Dr. Tahir Abbas Malik.
Pakistan polio eradication programme has achieved significant progress in recent years, thanks to renewed government commitment and revitalized community ownership. However, in cities like Karachi, poliovirus continues to be detected.
Working to overcome the virus once and for all, the polio programme an emergency action plan in January 2018. Since then, the geographical scope of the virus has been noticeably reduced. Much of this progress is thanks to religious leaders like Imam Qari Mehboob, who has spent years building trust and demand for polio vaccination in some of the most difficult areas of the city.
Gulshan-e-Buner is in the eastern corner of Karachi. The town includes some of the most impoverished and high-risk populations of the city. Playing in the streets, playgrounds and compounds that wind up and down the hilly landscape are around 2200 boys and girls under five years old. The places where they learn to crawl, walk, and run are perfect hiding spots for the paralysing poliovirus, but the last detection in the environment was in June 2016. No child in Gulshan-e-Buner has been paralysed by polio since 2014. In a community where vaccine refusal has sometimes caused problems, this represents a dramatic transformation.
Gulshan-e-Buner is one of the high-risk areas of Karachi where the polio programme first began community-based vaccination. Religious leaders helped to identify and recruit female vaccinators to reach every child with vaccines, and the area seemed well on the way to becoming polio-free. Then in 2012, an attack on health workers caused vaccination activities here to stop. In the years since, the commitment of religious leaders to ensure security, restore access, and build community trust has been crucial to defeat the virus.
Iman Qari Mehboob is 50 years old, a migrant from Khyber Pakhtunkhwa like most of his neighbours. He calls the community to prayer five times a day, and teaches many of the youngest children in the town. A father of four children, he is devoted to keeping them and all the other children in his community safe from the poliovirus. His support of the polio programme has helped increase vaccine trust, boost uptake of routine immunization services, and spark conversations about the vaccine.
During every polio vaccination campaign, Qari Mehboob goes from house to house with vaccination teams to check for any unvaccinated children. He speaks to parents who refuse the vaccine for their child, reassuring them that it is safe and effective. He conducts his work under the guidance of the National Islamic Advisory Group for Polio Eradication (NIAG), which educates religious leaders about polio eradication and the unique and important role they can play in protecting all Pakistan’s children from polio.
Under the guidance of NIAG, religious leaders are trained on the basics of social mobilization, communication, health, and hygiene. They also learn about the religious justifications for polio vaccination, including examining the arguments and fatwas of influential religious scholars.
Reflecting on his training, Qari Mehboob says, “The toughest job [for the NIAG trainers] is to convince religious clerics because their denial and doubt is deep rooted, but the collective Fatwa [scholarly verdict] of prominent scholars helps a lot”.
Since his training, Qari Mehboob has organised community engagement sessions to raise awareness about the dangers of the poliovirus. He often makes vaccination a central theme during his sermons at Friday and Eid prayers.
“I face less resistance because most of the people here know me personally and they rely on me because of my status as a religious cleric.” he says.
Qari Mehboob also uses the power and platform of his mosque to amplify his voice. He means this literally – sometimes he can be found using a loudspeaker. That’s so that mothers working inside compounds and homes can hear his messages, as well as the fathers who attend prayers. He doesn’t just speak about polio eradication, but also educates his community about personal hygiene, routine immunization and importance of education in Islam.
To thank him for his work, the provincial polio eradication programme team gave Qari Mehboob a clock during a Mosque promotional activity a few years ago. Below the time lies a message emphasising the importance of vaccination. Now displayed prominently on the wall of the mosque, the gift reminds parents why the polio vaccine is one of the best gifts that they can give to their children.
Back out in the streets of his town, Qari Mehboob laughs with local children as he checks their finger marking to make sure that they are vaccinated.
Discussing his motivation, he says, “These children are my own children. So I must protect them from any harmful disease - especially from a crippling disease like polio.”
At the end of the day’s campaign, Qari Mehboob offers tea and cookies to members of the provincial polio eradication programme team.
Since he joined the programme, vaccine refusals in Gulshan-e-Buner have dropped by 50%, and far more children receive their full polio vaccine doses on time.
Reflecting on the impact of his work, Qari Mehboob returns to his desire to keep all children safe. “I feel an extreme level of contentment after I contribute my part in the programme,” he says.
Dr Nosheen Safdar works as a Divisional Polio Surveillance Officer in Pakistan’s capital, Islamabad. A medical doctor, Dr Safdar has worked with the polio eradication programme for the past eight years.
Surveillance officers like Dr Safdar work with one aim: to detect and stop polioviruses from circulating before they have a chance to paralyze a child.
8:00 AM: Sample collection
As the sun rises, a health worker carefully pulls on gloves, a protective coat, and rubber boots, and climbs into a shallow stream located next to a market on the outskirts of Islamabad. His job? To collect a sample of the slow-moving sewage water that flows through the city.
This is environmental disease surveillance – sampling sewage at select points in cities and towns to test for the presence of the poliovirus, and to measure the quality of polio immunization activities.
In Pakistan, there are currently 57 sampling sites spread over 31 cities. This is the largest environmental surveillance network of any country in the world.
The collected sewage is transferred to a small container, packaged carefully and placed in a cool-box. It will be sent to the Regional Reference Laboratory for Polio Eradication in Islamabad for testing.
Each year, the lab tests thousands of environmental and stool samples from Pakistan and Afghanistan. The vast majority of these samples come back negative for polio. However, the tiny fraction of positive results tells the programme where the virus may be hiding.
Every time a sample is collected at this site, Dr Safdar observes the process to make sure that a high quality sample is sent to the lab.
“Testing sewage water for the presence of poliovirus is very important as it gives us the information if children in a given area are at risk of polio,” she says.
By midday, Dr Safdar is visiting the Children’s Hospital at the Pakistan Institute of Medical Sciences.
At the hospital, Dr Safdar reviews records of every doctor’s appointment. She is looking for cases of acute flaccid paralysis (AFP) – the key sign of poliovirus infection.
Staff in all health facilities are asked to report every case of AFP in any child under 15 years of age. Every suspected case acts as a signal that polio might be circulating in the area, and triggers an investigation by the polio eradication programme.
As she looks through the records, Dr Safdar checks if the nurses know what the symptoms of polio are, and what they need to do if a child with AFP is brought in.
Before she leaves, Dr Safdar visits a 4-year old child suffering paralysis.
She speaks to the child’s mother, and makes detailed notes, noting immunization status, travel history, and the child’s previous illnesses. She performs a detailed neurological examination and checks reflexes to confirm if the child is suffering from polio.
Dr Safdar hands over stool collection kits to the nurses. They will ensure that adequate samples are collected to investigate the cause of the child’s paralysis in the laboratory.
“The poliovirus lives in intestines, where it multiplies, and is finally excreted. This is why only through testing stool samples from paralysed children we can find out if polio was the cause,” explains Dr Safdar.
After leaving the hospital, she visits a girl who developed partial facial paralysis a few weeks previously.
For every suspected polio case, a 60-day follow-up consultation is conducted by the polio programme to check for long term paralysis. This takes place whether the paralysis was caused by polio or not.
To her family’s joy, this girl has fully recovered from her facial paralysis – a happy ending for her, and a positive outcome for Dr Safdar.
Whilst the girl’s mother offers tea, Dr Safdar writes down her final observations, and closes the case.
7:00 PM: Meeting at the Islamabad Polio Control Room
As night falls, Dr Safdar makes her way back to the Islamabad Polio Control Room, to report back on her day at an all-staff meeting.
“It’s important that we meet daily to all be on the same page and discuss cases that need particular attention and what can be improved,” explains Dr Safdar.
The team also receives updates on planned supplementary immunization activities and routine immunization.
As she heads home, Dr Safdar knows that the work to eradicate polio is not over. Tomorrow she will continue to track down the virus, working hard to ensure that her two children grow up in a polio-free world.
Children clutch parents as the crowds gather. Overhead, clouds fill the sky, whilst below, noise rolls around the square where people stand. Shouts, music, and laughs all contribute to a growing sense of occasion.
The excitement lies at the heart of Karachi, Pakistan’s largest metropolis. Mazar-e-Quaid, the mausoleum of Pakistan’s founding father Muhammad Ali Jinnah, is a prominent symbol of Pakistani independence, and of the united people of Pakistan.
Each year, millions of people from across Pakistan and the world visit Mazar-e-Quaid. The number of visitors reaches its peak on 14 August, Pakistan’s Independence Day. As the sun rises, thousands arrive dressed in green, the national colour, carrying food and flags, ready to be first to enter once the site is opened up to the public.
For the Pakistan polio eradication programme, Independence Day is an important opportunity. From morning to night, they will take part in a herculean effort to vaccinate all children visiting the mausoleum against the poliovirus. In doing so, they are setting world records for the number of children vaccinated in one location.
Permanent Transit Points (PTPs) are vaccination sites established at important transit points such as country and district borders, bus terminals and railway stations, to make sure that children on the move are vaccinated against polio. Currently, there are 390 PTPs across Pakistan.
On an ordinary day, eight vaccinators work at a PTP at Mazar-e-Quaid. After a quick brief, they are ready to protect all visiting children from the virus with just two drops of the safe, effective oral polio vaccine.
Independence Day requires a different kind of operation. The teams know that they have to take the opportunity to vaccine young children who otherwise might miss out.
Twenty vaccinators volunteer, enthusiastic to meet the influx of parents with young children entering the site.
As the crowds surge into the mausoleum, vaccinators immunize a new child every few seconds at fixed points at the entrance and exit, whilst others mingle with the crowds, searching for any young child without a purple stained finger – the sign used to indicate that they have been vaccinated.
This year, 11 409 children were vaccinated at Mazar-e-Quaid over the course of Independence Day. With such a small team, this is an impressive achievement.
Mehwish Sheikh is a vaccination supervisor at Mazar-e-Quaid and is considered to be one of the most dynamic polio eradicators to have ever worked there.
Talking about her passion for polio eradication, and what drives her to protect Pakistan’s children, she says,
“Working against polio is in my blood. My mother started as polio worker in 1992 with the start of the polio eradication drive. Following her, I have worked for more than a decade now.”
“My mother vaccinated the current Chairman of Pakistan People’s Party Mr. Bilawal Bhutto Zardari, and she was featured on television and newspapers. My sister is also a vaccination worker so vaccination and work against polio is our passion.”
“Will you believe that I took only 3 days off on my wedding and then rejoined the team here?”, she laughs.
So what is it like vaccinating on Independence Day?
Mehwish isn’t afraid to acknowledge the challenges that the teams face on 14 August each year.
“This is really a tough day for all of us because the number of people is so overwhelming. Peoples’ connection with their leader is especially strong on Independence Day.”
With a wry smile, she continues, “Of course, our real independence will be our independence from polio virus.”
The parents
Whilst vaccination in this context might seem unexpected, parents visiting the Mausolem are enthusiastic. This is thanks to the efforts of the Pakistan polio programme and the government to educate the population about the vaccine.
One father notes, “As parents, it’s our duty to protect our children from going into harm’s way and administering all sorts of vaccines is one way of doing this.”
A nearby mother concurs, “The vaccinators are here to save the lives of our children and we must cooperate with them.”
The eradication of polio in Pakistan will be a success for thousands of people involved in the programme, and a source of national pride.
Speeding past to vaccinate more children, one vaccinator calls out, “We want to see our names among those who are fighting the final battle against polio in Pakistan”.
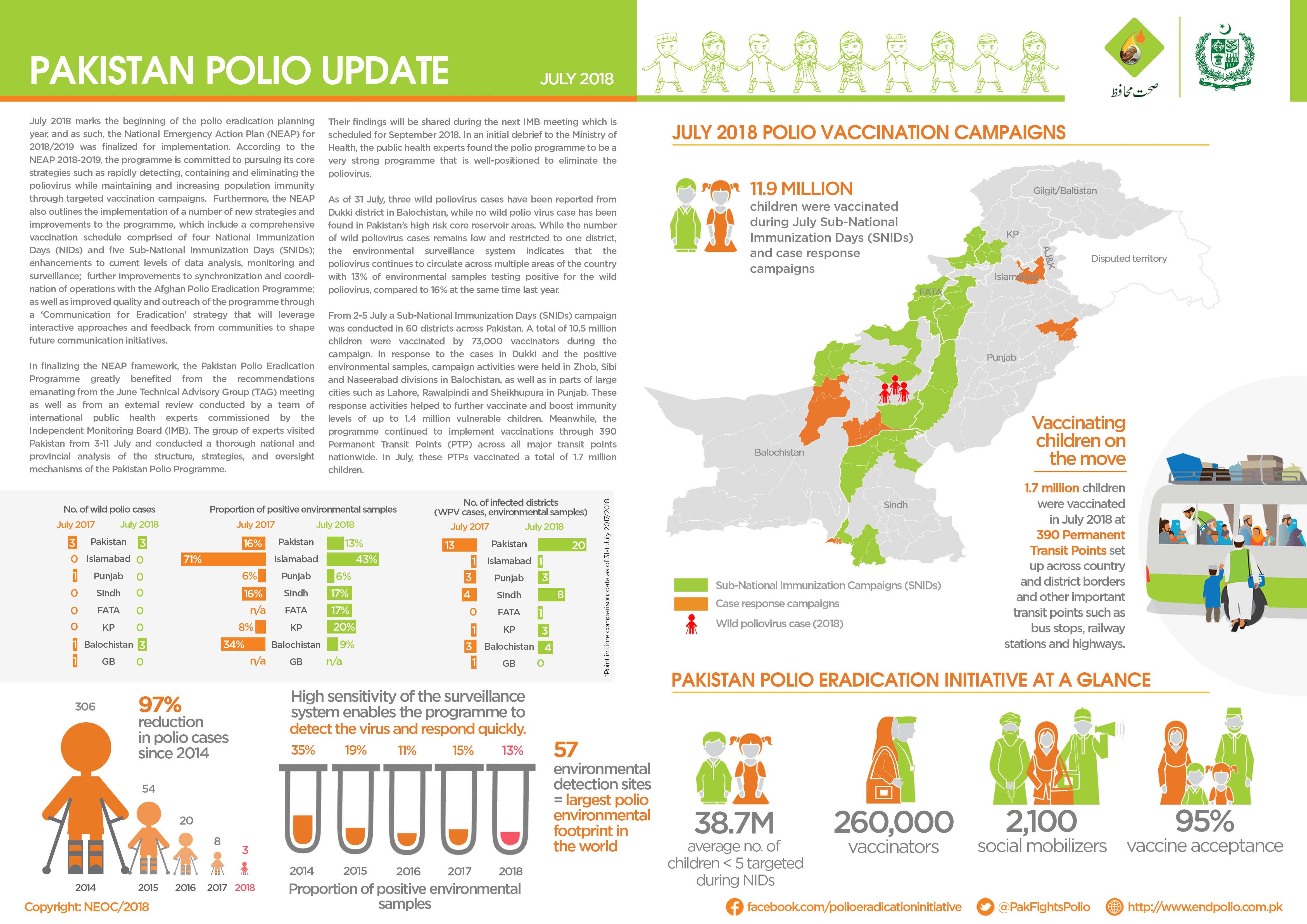
In July:
There were no new cases of wild poliovirus (WPV1) reported.
10.5 million children were vaccinated against poliovirus during case response campaigns by more than 73 000 dedicated frontline workers.
Teams at transit points and borders successfully vaccinated 1.7 million children.
Molvi Hameedullah Hameedi is a prominent religious scholar in a mountainous rural area of Killa Abdullah district, one of the poorest districts in Balochistan province, Pakistan. With a close connection to his community, who are mostly Pashtuns, he delivers the sermon each week during Friday prayers, and runs a religious seminary.
He is also a determined supporter of routine vaccination for all children, and an advocate for better health.
This might come as a surprise if you met Molvi Hameedullah just a year or two ago. For most of his life, he did not believe in the safety and effectiveness of the oral polio vaccine, the key tool of polio eradication.
“I was a religious scholar who was very sceptical of non-governmental organizations and the polio vaccine,” he reflects.
“After reading anti-vaccine books and papers, I began following the work of anti-vaccine campaigners. Soon, I came to consider it my religious duty to spread awareness against the polio vaccine.”
“But it all changed when I was invited to a two-day International Ulema conference in Islamabad where religious scholars from all over Pakistan and other Islamic countries were invited to debate polio vaccination.”
The conference Molvi Hameedullah attended was hosted by the Islamic Advisory Group for Polio Eradication (IAG). The IAG was launched in 2014 by leading Islamic institutions including Al-Azhar University, the International Islamic Fiqh Academy (IIFA), the Islamic Development Bank (IsDB) and the Organization of Islamic Cooperation (OIC).
For Molvi Hameedullah, attending the conference marked the beginning of a change in perspective. “At the conference, I was given an opportunity to discuss my apprehensions towards polio vaccine. The talks I had motivated me to further research the pro-polio vaccine stance, and I started meeting with religious scholars in Karachi to debate polio vaccination.”
“Through talking to these people, I was getting a completely different picture to what I had believed earlier.”
By educating religious leaders and scholars about the poliovirus, and explaining religious justifications for vaccine acceptance, the IAG and its national equivalent equip people like Molvi Hameedullah with the tools to act as health advocates. The same skills that help scholars engage with parents about the polio vaccine are applicable for wider health, including improving routine immunization, hygiene practices, and maternal and child health.
After the conference Molvi Hameedullah was offered support by other vaccine-promoting scholars.
“I received a book from a religious support person working for polio vaccination in my area. Included were dozens of fatwas from highly esteemed madrassahs and religious teachers. I was initially sceptical, so I telephoned the madrassahs who had written them. To my surprise, all the fatwas were genuinely issued by them, and they also urged me to support vaccination wherever I called.”
Today, Molvi Hameedullah teaches similar fatwas as a member of the Provincial Scholar Task Force under the National Islamic Advisory Group. Most Task Force members have an honorary position, and are not paid a salary. Instead, the local government facilitates their transport and communication needs during immunization campaigns. Of his new role Molvi Hameedullah says, “I was faced with a different problem. I had been working against polio vaccination for many years, and now felt that I had done a great damage to the children and parents of my community. I felt it was now my absolute religious duty to negate all that I had taught before. I decided to step forth, and started working in the community voluntarily to promote vaccination.”
Religious refusals in Molvi Hameedullah’s area have declined. He has begun supporting other ways of ensuring that every child receives a vaccine, including by recruiting women vaccinators.
He acknowledges that the work he does now is not easy. He and his fellow scholars sometimes face challenges from those accusing them of having a political agenda, and changing beliefs informed by years of cultural and religious tradition takes time and patience. But he vows to continue his new mission until eradication.
There have been no cases of polio in the area of the district that Molvi Hameedullah covers since he joined the Provincial Scholars Task Force. Looking ahead, he is determined not to stop until all of Pakistan is polio-free.
A pale blue sky stretches from east to west. The ground is dusty, the journeys of thousands of people compacting it into a hard dirt track. Ahead stands a structure known as the Friendship Gate – with people laden with bags and boxes weaving paths beneath it. This isn’t an ordinary street, but a border crossing between Afghanistan and Pakistan, where people, goods, livestock, and sometimes, the poliovirus, pass from one country to the other.
Porous borders, which enable the continuous movement of people between countries, are a contributing factor to poliovirus transmission in Afghanistan and Pakistan. Along with Nigeria, these are the only wild poliovirus endemic countries in the world. Look at a map of poliovirus cases and positive sewage samples over time, and transmission ‘corridors’ can be clearly seen, evidence of the virus passing consistently between the countries. Every year for decades, the virus has made it over the border through key entry and exit points, hiding in children.
Spin Boldak in southern Afghanistan and Chaman in western Pakistan are both important border crossing points centrally positioned in what is known by epidemiologists as the ‘southern corridor’. Today, thanks to collaboration between the governments of Afghanistan and Pakistan, and the efforts of hundreds of thousands of individuals working to fight the virus, this important crossing is attended by polio vaccinators, seven days a week, 24 hours a day. With two drops of safe, effective vaccine, they ensure that every one of the thousands of children under the age of ten entering the other country each month leaves the poliovirus behind.
To defeat the virus, polio eradicators seek to understand the push and pull factors of people crossing the border. Many are traders, some seek medical treatment in Pakistan, others visit relatives on both sides of the border. Many have sought refuge in Pakistan, or are forced returnees. Many come from areas where health systems are weak, and some children have never been vaccinated before.
To defeat the virus, Afghanistan and Pakistan have built strong relationships. Studded along the border – which weaves from north to south, through mountainous areas, deserts, and between busy cities– are 15 WHO and UNICEF supported vaccination posts, hosting 42 vaccination teams. Each month, they vaccinate tens of thousands of children for free, no matter what their nationality or reason for being at the border.
Dressed in Rotary ‘End Polio Now’ hats, and surrounded by bright banners, the cross-border health workers also watch out for children travelling across the border presenting signs of acute flaccid paralysis, an indicator of potential polio infection. Vaccinators also speak to parents, educating them about the importance of vaccines, and the other immunization services that they can get free-of-charge in the country they are crossing to. For many without free professional health-care, this is a crucial service. Most arrive unaware of the benefits they can gain to protect their children’s health, and this information is not always easy to come by.
The polio programme also works with other humanitarian organizations near the border. As the situation changes, with refugee numbers fluctuating accordingly, the vaccination teams work to ensure children can be reached at or near the border, with few missed. In April, 2289 children under the age of ten, mostly from Pakistan and Iran, were vaccinated near the border with oral polio vaccine by teams receiving them into UN Refugee Agency (UNHCR) repatriation centers and sites run by the International Organization for Migration (IOM).
Polio vaccination at the border prevents the reintroduction of the virus into areas of Afghanistan and Pakistan where no cases or environmental positive samples have been seen for some time, and reduces incidence of the virus in areas where it is still circulating. Our team gives every child a strong start in life – whether they are a refugee or a returnee, and irrespective of their place of origin. As the team in Spin Boldak and Chaman finishes its shift for the day, the next team continues their task: to protect all children at the border, and help end polio.
In April:
No new cases of poliovirus (WPV1) were reported.
38.9 million children were vaccinated against poliovirus by a team of 260 000 dedicated frontline workers.
Teams at transit points and borders successfully vaccinated 1.5 million children.
Almost everyone in the Killa Saifullah district of Balochistan, Pakistan, knows and respects 35-year-old Taj Muhammad. A dedicated and passionate doctor by profession, Dr Taj spends his days working as a Union Council Medical Officer in his local public health facility, and his evenings running a free medical clinic for local residents.
In his capacity as Medical Officer, he coordinates polio eradication efforts at the Union Council level, which is the smallest administrative unit in Pakistan.
His role includes coordinating microplanning, training frontline health workers, and supervising polio vaccination campaign activities. Since the start of his medical career in 2007, he has supervised more than 100 polio vaccination campaigns.
Dr Taj says he became a doctor to fill the existing health care gap in his area. “During my childhood, my mother was seriously ill and she died because of the absence of medical facilities in our area. She often used to tell me that I must become a doctor to help poor people with their health. She died afterwards but her words are still in my heart,” he explains.
His hometown, Killa Saifullah, is located 135 kilometers away from Balochistan’s provincial capital Quetta. Economic and social deprivation is widespread, and the district lacks basic health facilities, particularly for women and children. “There is only one hospital, serving only 150 people per day in the district, whereas the current population is more than 200,000. In these conditions, working as a medical officer is quite challenging,” Dr Taj says.
His job is tiring, and the demands are huge, but Dr Taj perseveres. As well as supporting polio vaccination activities, and endorsing vaccination, each day he tends to the large crowd of people who gather outside his evening clinic, often desperately needing health care.
His work to serve his community is particularly important because Killa Saifullah lies close to Dukki, where the only case of polio in Pakistan so far in 2018 was reported. Nawabzada Dara Khan, who chairs the Killa Saifullah’s Municipal Committee, notes that the community feels “vulnerable” knowing that the virus is close by.
Since the first polio case of 2018 was detected, polio vaccination campaigns have been conducted in response in all neighboring districts, including Killa Saifullah. But whilst this has increased immunity to the virus, it has also caused vaccine hesitancy amongst some parents, who question the need for multiple vaccination campaigns.
“We are trying hard to vaccinate each and every child; however, repeated campaigns and misconceptions are posing a big challenge for us,” Dara Khan says.
Luckily, the efforts of dedicated doctors like Dr Taj are helping to remove misconceptions and doubt. With the immense trust and respect he enjoys from his community, he has been able to use his free evening clinic as a local platform to advocate for polio eradication and the safety of the vaccine, extending his critical role in the polio programme.
Dara Khan adds, “The contribution of Dr Taj in polio eradication is commendable. His goodwill is playing a very positive role within our community to remove these misconceptions.”
His impact is also wide ranging, reaching multiple different families.
The proof? In April, thanks to the intensive efforts of Dr Taj and others, no parents or caregivers in Killa Saifullah refused vaccination.
That’s 70,690 children who now have lifelong protection from polio.
Karachi, the capital of Sindh province, is Pakistan’s largest city, with an estimated population of more than 16 million people. It is also by far the most challenging place in Pakistan to eradicate polio. Difficulties include the large and frequent movement of people, poor water and sanitation conditions, and pockets of community resistance to vaccination.
In 2017, two of Pakistan’s eight total cases of polio were located in Karachi, and multiple environmental samples continue to test positive for the virus.
In the northwestern part of the city lies Orangi Town. The fifth largest slum in the world today, it is a tough place to live for the children who run around and play games in the streets outside their homes.
One of their most pressing needs is a supply of clean, drinkable water. In Orangi Town, the sewage system is basic, and poorly maintained. At many points, human waste mixes with drinking water lines. The quality of potable water is low and filled with pathogens including bacteria and viruses, and it is the main cause of many water-borne illnesses in adults and children, including hepatitis A, acute watery diarrhea and typhoid. Polio can also be spread through drinking water contaminated with the stools of an infected person.
Health workers for the polio eradication programme work tirelessly to immunize every child. But there are other ways to reduce the spread of the virus – and provision of uncontaminated drinking water is one of them.
Thanks to the efforts of Rotarians, who raised 50% of funds, 55 000 residents of Orangi now have access to a new water filtration plant. By ensuing that there are no viruses or bacteria present in the water, the plant will protect children from water-borne illness. As the plant runs using solar energy, it will work consistently through the regular power outages that affect the city, and won’t require expensive oil or electricity to run, placing fresh water within the reach of all.
Speaking on 8 May at the opening of the plant, Mr Aziz Memon, Chairman of Pakistan’s National Rotary PolioPlus Committee said: “This is the 15th water filtration plant installed in Pakistan, and the sixth in Karachi, and we will do all that we can with our partners to help raise the community’s standard of living including health.”
Dr Shafiq, a representative of Orangi Town, thanked Rotary International for its continuous support of polio eradication in the area. Combined with vaccination activities, children drinking the clean water provided by the new plant will now have an improved chance to grow up polio-free.
National Chair Aziz Memon said: “Orangi Town is one of the most underprivileged urban slums in Karachi and the supply of safe drinking water will improve health issues of the community and save children from water borne diseases.”
He added that “Rotary is making intensified efforts in this impoverished area and has established a Resource Center in Bijli Nagar Orangi Town.”
These extra steps towards ensuring that children are safe from disease also help to gain community trust, and form part of Rotary’s work to raise awareness of polio, and overcome vaccine hesitancy. In 2016, Rotary International contributed over US$ 106 million to polio eradication worldwide, and in Pakistan, Rotarians are at the forefront of the fight against the virus.
By chance, the opening ceremony of the plant coincided with the second day of this month’s subnational immunization days, when over 20 million children across different parts of the country were targeted with oral polio drops. Emphasizing the link between safer water, and polio eradication, children were given polio vaccine by high profile individuals attending the event.
Kicking off a safer future for some of Orangi’s children, Mr Memon and Rotary District Governor Ovais Kohari pushed a button at the plant to allow clear, safe water to flow from the taps. They then had a drink of water to test the quality and taste.
Simultaneously, polio vaccinators were going from house to house all over the city. For some families, Rotary was providing two life changing interventions in just one day – an effective vaccine, and water that they could finally trust.
On top of the US$ 120 million committed in 2013, last year, HH Sheikh Mohamed bin Zayed pledged an additional US$ 30 million towards polio eradication, and the UAE is active on the ground in Pakistan through the UAE-Pakistan Assistance Program
UAE support also funded more than 5000 committed full-time vaccinators in highest-risk districts of Pakistan
Last year saw the lowest number of wild poliovirus cases in history (22 worldwide); Pakistan reported a 97 percent decline in cases between 2014 and 2017
GENEVA (16 April 2018) – The Global Polio Eradication Initiative (GPEI) announced today that the UAE has completed the US$ 120 million commitment made by His Highness Sheikh Mohamed bin Zayed Al Nahyan at the 2013 Global Vaccine Summit in Abu Dhabi.
“We thank the UAE for their long-term generous support and unwavering dedication to polio eradication, and particularly the personal commitment of His Highness Sheikh Mohamed bin Zayed Al Nahyan, Crown Prince of Abu Dhabi,” WHO Director General Dr Tedros Adhanom Ghebreyesus said. “This is the kind of support that will ensure we reach every last child to complete the job and to show the way to delivering health to all.”
Polio is a highly infectious disease that can cause lifelong paralysis, but it is entirely preventable with vaccines. Only three countries remain which have never stopped polio: Afghanistan, Pakistan and Nigeria. When the polio eradication effort was launched in 1988, 350 000 children were paralyzed by polio every year across 125 countries.
Polio eradication efforts have since made remarkable progress and there were only 22 cases in 2017 – the lowest ever recorded number. However, a number of key challenges remain. Reaching the most vulnerable children with the polio vaccine is hampered by a range of hurdles including difficult terrain, insecurity, and large-scale population movements.
Following the Global Vaccine Summit, the UAE expanded its role through the UAE Pakistan Assistance Program (UAE-PAP) to ensure that further gains would be made where it was needed the most. Through the “Emirates Polio Campaign” initiative, the UAE has helped drive on-the-ground eradication efforts within the most vulnerable communities in Pakistan.
Speaking about the UAE’s work, His Excellency Mohamed Mazrouei, Undersecretary of the Crown Prince Court of Abu Dhabi said: “The UAE’s pivotal role in eradicating polio completely is not limited to being a donor only, but extends to include its capacity to convene key groups and provide on-ground support to deliver vaccines in the highest risk areas of Pakistan.
“The UAE’s support – both as a leading donor and passionate advocate – has been critical for getting as close as we’ve ever been to making history by eradicating polio,” UNICEF Director of Polio Eradication Akhil Iyer said. “This is a gift not only to the children of Pakistan but to all future generations of children, everywhere, who are so close to the goal of being able to be born and be raised in a polio-free world.”
Dr. Chris Elias, President of the Global Development Program, Bill & Melinda Gates Foundation, said: “The UAE and His Highness Sheikh Mohamed bin Zayed Al Nahyan have shown an unwavering commitment to end polio, and we are delighted to partner with them in this effort. Without their involvement, achieving a record low number of polio cases in 2017 would not have been possible.”
The UAE is a longtime supporter of the polio eradication program. In addition to the US$ 120 million that His Highness Sheikh Mohamed bin Zayed Al Nahyan pledged in 2013, he pledged a further US$ 30 million to polio eradication, announced by Bill Gates at the Rotary International Convention in Atlanta, USA in June 2017. With additional commitments in 2011 and 2014, in total, the UAE has contributed US$ 167.8 million since 2011 to help end polio, with direct support to Pakistan, Afghanistan, Somalia, Ethiopia, Kenya, and Sudan.
The Global Polio Eradication Initiative (GPEI) is led by national governments and spearheaded by the World Health Organization (WHO), Rotary International, the US Centers for Disease Control and Prevention (CDC), and the United Nations Children’s Fund (UNICEF), with the support of the Bill & Melinda Gates Foundation. Since its launch at the World Health Assembly in 1988, the GPEI has reduced the global incidence of polio by more than 99%.
The GPEI receives financial support from governments of countries affected by polio, private sector foundations, donor governments, multilateral organizations, private individuals, humanitarian and non-governmental organizations and corporate partners. A full list of all contributors is available on the GPEI website, https://www.archive.polioeradication.org/financing/donors/
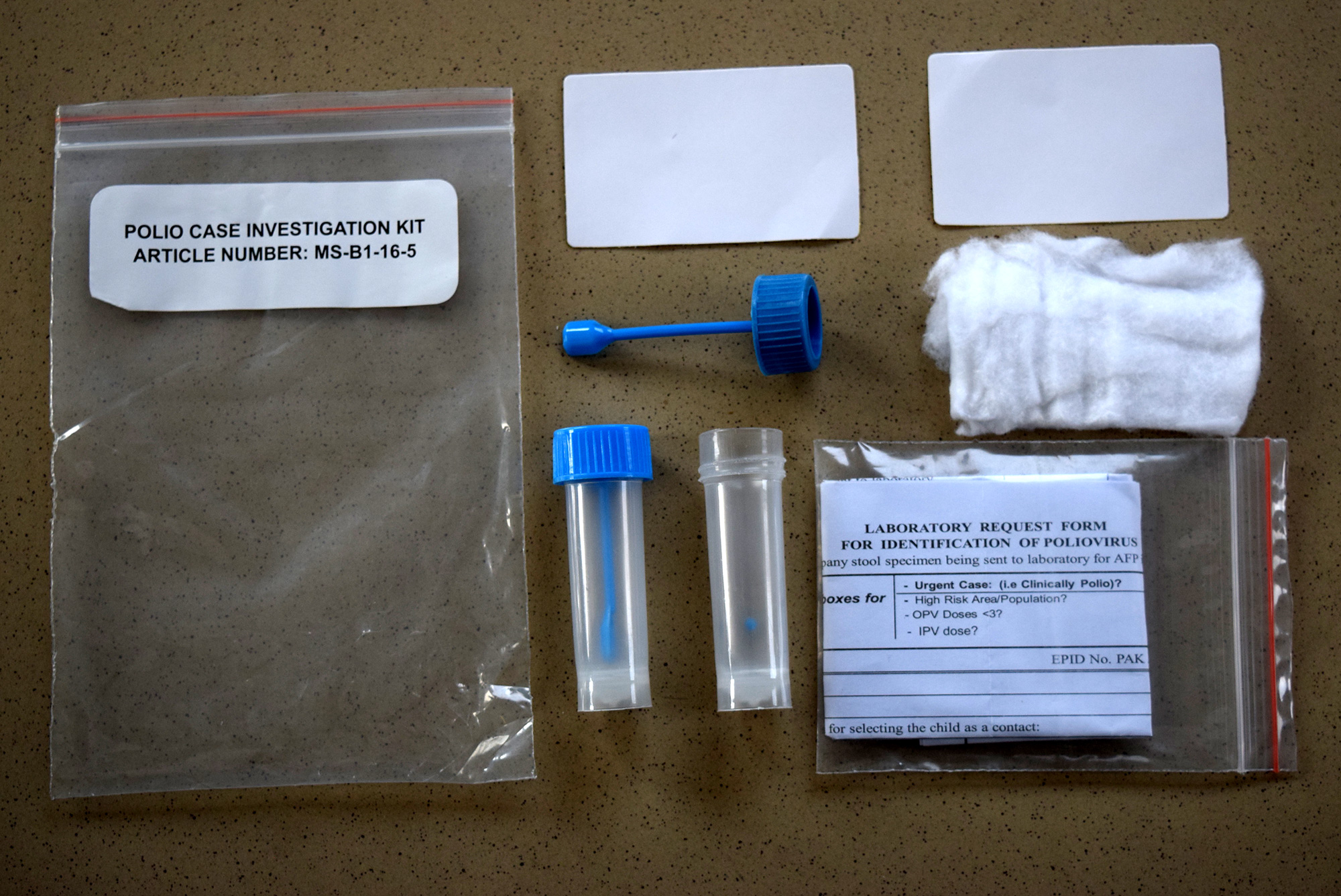
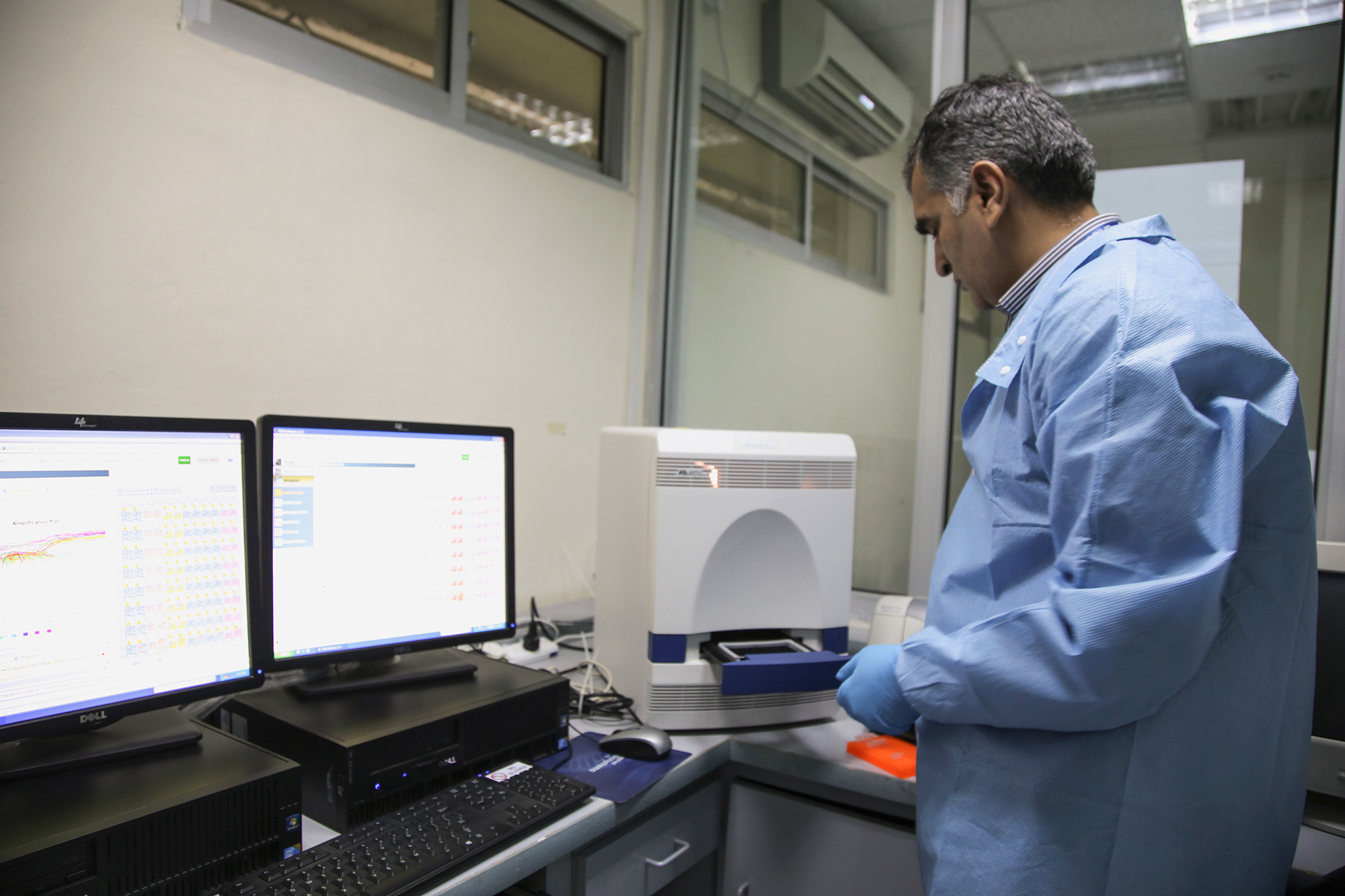
Surveillance is one of the main pillars of the polio eradication initiative. By testing stool samples collected from children suffering acute flaccid paralysis – the clearest symptom of the virus – as well as samples taken from sewage water, we are able to find the poliovirus wherever it is hiding.
Pakistan’s polio surveillance system is one of the largest ever established in the world. Click through these pictures to learn about the journey of a stool sample there: From a child with suspected polio to the laboratory.
In Pakistan, a wide network of health workers, teachers, and other community members vigilantly look out for signs of polio in children in their area. These volunteers detect and report to the polio surveillance system children showing possible symptoms of the virus, often floppy or weakened limbs with rapid onset of paralysis, known as acute flaccid paralysis. Every suspected case acts as a signal that polio might be circulating in the area, and triggers an investigation.
The poliovirus lives in children’s intestines, where it multiplies, and is finally excreted. When a child with acute flaccid paralysis is reported to the surveillance system, health workers collect the child’s stool samples and transport them to the lab in specially designed cool boxes. The boxes ensure a constant temperature of between 4 to 8 °C, so that the viruses in the samples remain high enough quality to test. Once collected, stool samples from all corners of the country must reach the Pakistan Regional Reference Laboratory for polio eradication, based in Islamabad, within 72 hours.
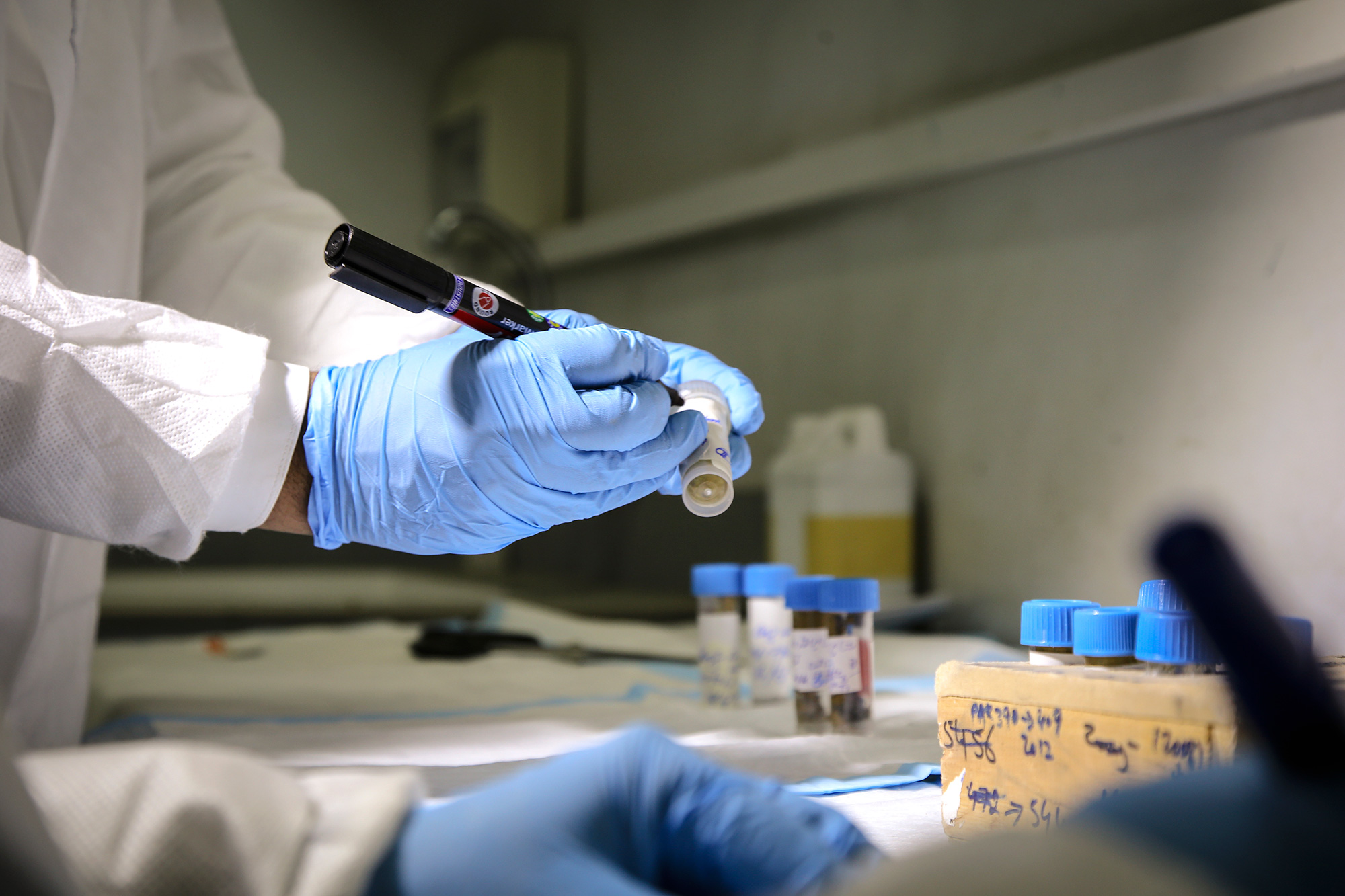
The Regional Reference Laboratory was established in 1991 and tests around 30 000 stool samples each year from both Pakistan and Afghanistan. More than 99% of these stool samples come back negative for polio. This is because most cases of acute flaccid paralysis are not caused by poliovirus. However, the tiny fraction of positive results tells the programme where the virus may be hiding.
Dr Salmaan Sharif is a Molecular Biologist, and the Coordinator of the Regional Reference Laboratory in Islamabad. He supervises a team of 34 lab staff, each responsible for a different component of surveillance sample testing. With an increase in reported acute flaccid paralysis cases, and environmental sampling sites, the workload of Dr. Sharif and his team is increasing. This is a sign that the polio surveillance system is working well, as a large number of reported acute flaccid paralysis cases and environmental samples gives us our best chance of finding the virus.
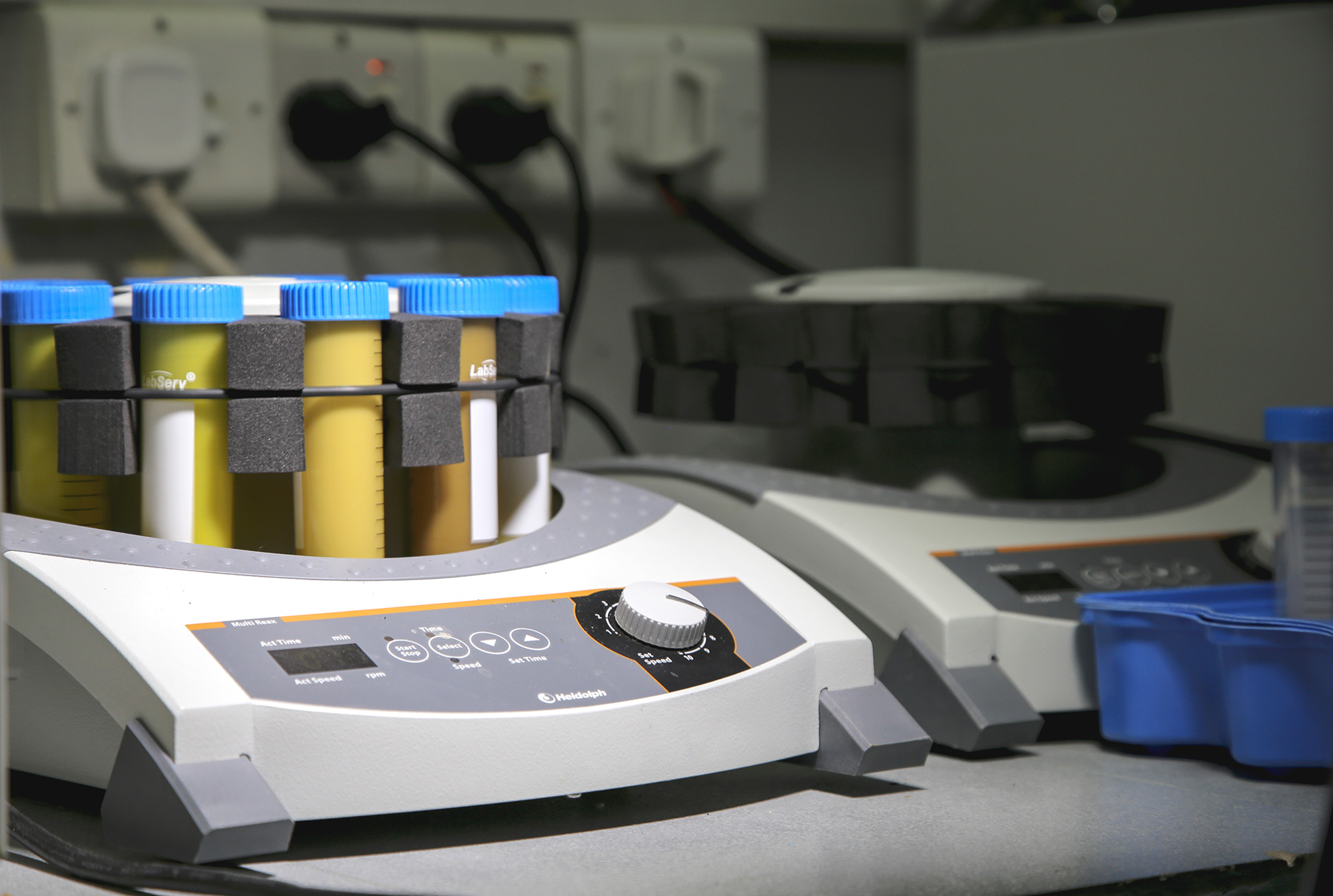
Each sample is then processed in a centrifuge, which separates the components of the sample. Solids will drop to the bottom and liquids will remain at the top. Any poliovirus will remain in the liquid component. Once separated, a scientist is ready to inoculate a healthy cell.
From the processing room onwards, extensive biosafety measures are taken to ensure that all virus is kept in the controlled environment, that contamination of other samples does not occur, and humans are not at risk of exposure. During the primary screening, healthy cells are mixed with the liquid component of the processed stool sample, and are then grown in an incubator at 36 °C for up to ten days. An incubator mimics the natural environment of the virus, creating the ideal conditions for the virus to grow. If the virus is present in the processed stool sample, it will infect the healthy cells.
A daily microscopic examination is performed to determine whether poliovirus is present in the processed stool sample. Infected cells are visibly broken in pieces, while healthy cells are seen as long strands.
If poliovirus is isolated in a stool sample, further tests are carried out to determine what type of virus this is and where the strain may have originated. A Polymerase Chain Reaction (PCR) machine is used to determine the kind of poliovirus detected (known as the serotype), and to distinguish further between wild poliovirus and that related to the vaccine-derived.
The next step is genetic sequencing. By reading the genetic code of the virus, wild viruses can be compared to others and classified into genetic families. From this, the geographic origin of the virus can be determined. This helps to guide the programme when deciding the best immunization strategies to stop transmission, and to prevent further spread of the poliovirus.
The polio surveillance system stretches even further than stool sample testing. In carefully selected places where the virus could be hiding, surveillance officers collect sewage samples. These are also sent to the Regional Reference Laboratory for processing, using a method similar to the testing of the stool samples. Crucially, environmental surveillance can help find polio in the environment before it has a chance to paralyse a child.
In Pakistan, the programme has used environmental surveillance to test and detect the presence of poliovirus in the sewage in high-risk locations since 2009. The network has continued to expand over time with a wider coverage. Currently, there are 53 sampling sites in 33 districts and towns of the country, making it the largest environmental polio surveillance network ever established.
The sensitive polio surveillance system finds the poliovirus wherever it exists – from the most remote villages to huge cities. With the polio case count at the lowest level in the history of Pakistan, the country intends to make 2018 the year of poliovirus interruption, keeping current and future generations of children safe from this disease. Thanks to the generous support of the Government of Japan, the Islamabad laboratory is continuing to expand operations, now able to procure new state-of-the-art molecular biology equipment to help detect the last remaining reservoirs of the virus.
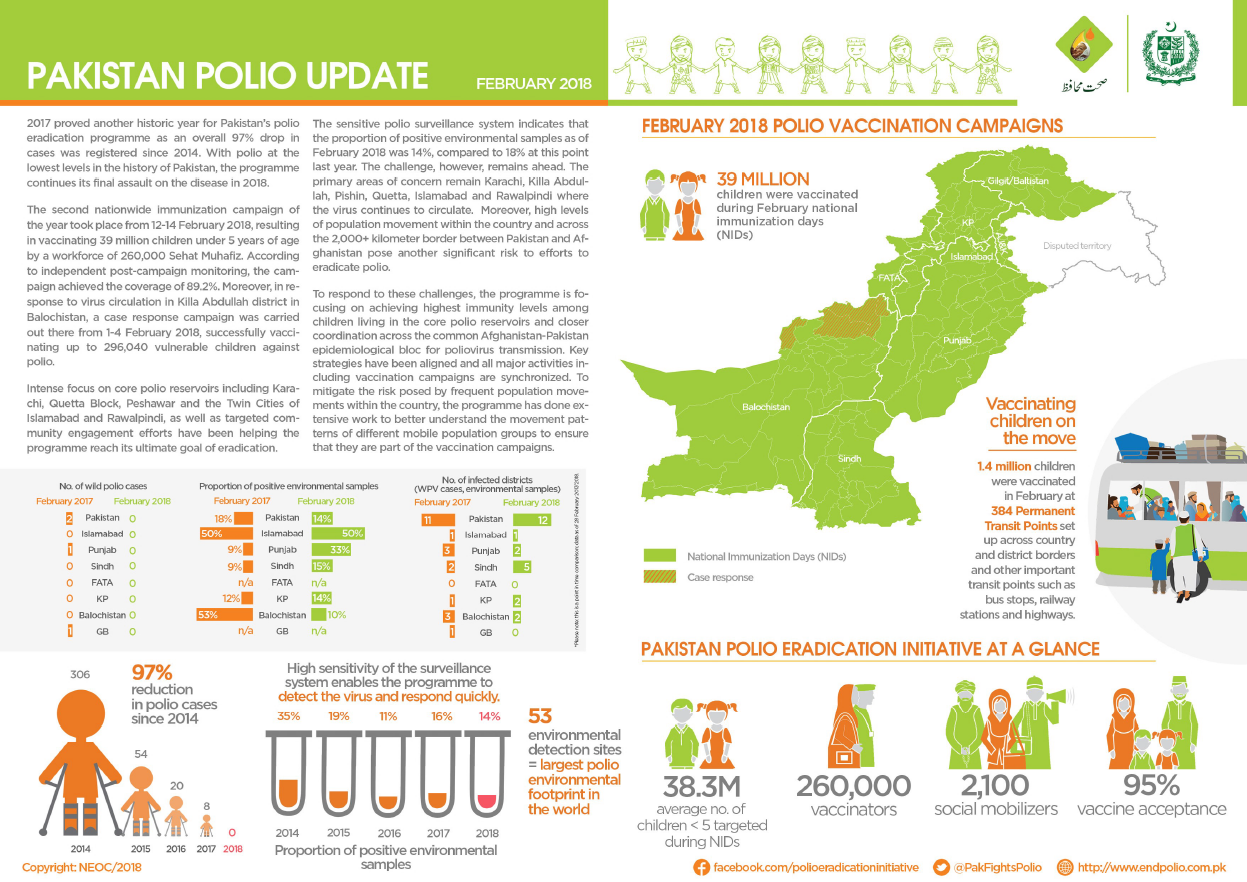
The Pakistan polio snapshot gives a monthly update on key information and activities of the polio eradication initiative in Pakistan.
In January:
No new cases of wild poliovirus (WPV1) were detected.
More than 39 million children were vaccinated against poliovirus by a team of almost 260 000 dedicated frontline workers.
Teams at transit points and borders successfully vaccinated 1.5 million children.
Vaccinating high risk mobile populations, like children of brick kiln workers, is essential to ensure polio is eradicated in Pakistan. UNICEF/R.Curtis
THE NOMADS
Faryad Rehman can’t read or write, and lives on a dirt floor in one of 18 dusty tents clustered together a stone’s throw from the main road to Lakki Marwat in southern Khyber Pakhtunkhwa (KP), where his two-month-old daughter Naina was born.
Naina will likely never go to school – no one in the camp has ever been to school – she has never seen a doctor, or received an immunization against any disease. Except for one: in her two months of life she’s already been immunized twice by the visiting two-person polio vaccination teams.
The Rehmans are economic nomads, based in Lakki Marwat but moving seasonally to East Punjab, Sindh or D.I. Khan to follow the harvest, work in a brick kiln, labor on a construction site, or attend a relative’s wedding or funeral. They make bangles, sell plastic toys and work as beggars, the women and infant children cloistering at red lights and intersections seeking small change.
Once from Balochistan, these nomads speak Saraiki, can barely understand the native Pashto tongue of KP, and converse with their vaccinators in the common Urdu. Faryad says his only use for a local newspaper is “to wrap the bangles in”.
For Pakistan’s polio programme, these High-Risk Mobile Populations, or HRMPs – nomads, Internally Displaced Persons, Afghans, brick kiln workers and visiting “guest children” – are critical. With just a handful of polio cases reported in the country this year, these most vulnerable children, who often live outside the traditional health system, could be the key to stopping the virus from moving inside Pakistan or across the border to Afghanistan – and ultimately stopping it altogether.
In the district of Lakki Marwat, 742 polio vaccination teams go door to door to protect 173 545 children under the age of five against polio. But District Health Officer Dr Taouse Khan says it is the 5562 HRMP children the programme worries about the most: “HRMPs are not an afterthought, they’re our principal focus – on the first day of each campaign we cover these HRMPs. In this settlement there are 18 tents here and 27 children under the age of five, and each and every child of this camp has been identified and recorded.”
Faryad says his nomadic group have called Lakki Marwat home, on and off, for 15 years: “It’s good here. We’ll stay here until the landowner tells us to go, then we’ll go.”
THE VACCINATORS
In a small, windowless room off a laneway in Lakki Marwat City, 40 Lady Health Workers wrapped in colourful shawls are conducting a polio refresher training. Here they learn facts about polio and acute flaccid paralysis, and the inter-personal communication skills they need to speak with mothers about the importance of the polio vaccine. In recent months, they’ve been trained repeatedly to not only provide life-saving messaging inside the walled
household compounds, but to specifically seek out visiting guest children for vaccination.
“We are well aware of HRMPs and guest children,” says vaccinator Tabassum Rana, “as well as vaccinating all the children on the streets and on the move, in the backs of trucks or rickshaws or carts. We know how to search for every child and we do search for every child. If I even see a child on the back of a motorbike passing through my area, I stop them to give the vaccination.”
Vaccinators do not only go house-to-house. Across Khyber-Pakhtunkhwa province, there are also 89 Permanent Transit Points (PTPs) vaccinating children on the move. In Lakki Marwat, there are 5 PTPs and an additional 5 temporary points to enable vaccination of children during the current seasonal high movement in the region.
THE AFGHANS
Mohammad Sayed is in his 50s, and has lived in Pakistan for more than 40 years. Once from Gardez, Afghanistan, he’s spent his working life stoking furnaces in brick kilns and doing petty jobs. His family and countryfolk have moved in around him, and now the houses of hundreds of Afghan settlers spread out through the fields.
In all, there are 56 Afghan Refugee settlements across KP province – four of them in Lakki Marwat, with a total target population of 1,834 children under five. With polio moving freely between Pakistan and Afghanistan – mostly in the bellies of Afghan children passing back and forth across the border, these populations are a key focus for the programme. In Mohamad’s settlement, 373 children under five are documented to be vaccinated in every campaign.
Mohammad fears the once-easy movement across the border to Afghanistan is now a thing of the past. “Just two years back it was no problem going and coming back but not now. Now if we go back with our Afghan passports we can’t come back. Now we break our houses down and take the door frames and the windows and we go there and build again.”
Now his trips are limited to “Faisalabad and Peshawar, for business. We’ve been 40 years in Pakistan, doing business.”
THE SOCIAL MOBILIZERS
COMNet social mobilizer Kalim Ullah has tracked every HRMP in his area, but maintains there is no room to rest. “I visit all the brick kilns and nomadic settlements each month, investigate if there are new tents, new arrivals, ask if there are any pregnant women or newborn babies. This field validation is part of our duty. But it is hard to track every tent, every brick kiln.”
“We go there and we gather their elders and we speak about the importance of the campaign. The settlements have a lot of issues – no water, no electricity. But I tell them that next week you might get water, you might get electricity, but if today your child gets paralyzed from polio, there’s nothing you can do for him next week.”
THE BRICK KILN WORKERS
On the road out of Lakki Marwat, a brick kiln chimney spews black smoke into hazy air. Here, four families are living and working, with five children under 5. At this site, all the workers are local, “but there was a brick kiln over there,” the men say, pointing to a distant chimney, “where all the labourers were from Jamshoro, Sindh. They’ve gone now.” Where? They shrug. “We don’t know.”
At the workers’ house flanking the chimney, the social mobilizer speaks through a door to the women inside. All the men are working, so he can’t go in. In the last campaign, a senior woman’s voice says from inside, they had a ‘guest child’ stay – her daughter and son-in-law visited from Zhob, Balochistan. She says he works in the mines there.
One day later, it is announced that Pakistan’s seventh polio case for 2017 has been detected – in Zhob, Balochistan. The hunt for every last child goes on.














































 The Rehmans are economic nomads, based in Lakki Marwat but moving seasonally to East Punjab, Sindh or D.I. Khan to follow the harvest, work in a brick kiln, labor on a construction site, or attend a relative’s wedding or funeral. They make bangles, sell plastic toys and work as beggars, the women and infant children cloistering at red lights and intersections seeking small change.
The Rehmans are economic nomads, based in Lakki Marwat but moving seasonally to East Punjab, Sindh or D.I. Khan to follow the harvest, work in a brick kiln, labor on a construction site, or attend a relative’s wedding or funeral. They make bangles, sell plastic toys and work as beggars, the women and infant children cloistering at red lights and intersections seeking small change.
 Mohammad Sayed is in his 50s, and has lived in Pakistan for more than 40 years. Once from Gardez, Afghanistan, he’s spent his working life stoking furnaces in brick kilns and doing petty jobs. His family and countryfolk have moved in around him, and now the houses of hundreds of Afghan settlers spread out through the fields.
Mohammad Sayed is in his 50s, and has lived in Pakistan for more than 40 years. Once from Gardez, Afghanistan, he’s spent his working life stoking furnaces in brick kilns and doing petty jobs. His family and countryfolk have moved in around him, and now the houses of hundreds of Afghan settlers spread out through the fields. COMNet social mobilizer Kalim Ullah has tracked every HRMP in his area, but maintains there is no room to rest. “I visit all the brick kilns and nomadic settlements each month, investigate if there are new tents, new arrivals, ask if there are any pregnant women or newborn babies. This field validation is part of our duty. But it is hard to track every tent, every brick kiln.”
COMNet social mobilizer Kalim Ullah has tracked every HRMP in his area, but maintains there is no room to rest. “I visit all the brick kilns and nomadic settlements each month, investigate if there are new tents, new arrivals, ask if there are any pregnant women or newborn babies. This field validation is part of our duty. But it is hard to track every tent, every brick kiln.”