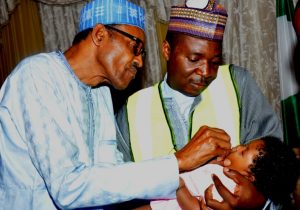
A child’s finger is marked after being vaccinated. Bodinga, Nigeria photo:Christine McNab
Independent polio campaign monitoring is carried out to assess the quality and impact of supplementary immunization activities. It is critical to guiding any necessary mid-course corrections if gaps or problems are found.
The basic elements of monitoring include recording: the number and source of independent monitors, the number of children monitored, the percentage of children whose fingers are marked to prove they were vaccinated (both in house-to-house monitoring and out-of-house) and the proportion of districts monitored.
Real-time, independent monitoring data answers the question, “How many children did we reach with vaccine?” It allows rapid changes to be made to cover missing children and stop polio transmission more quickly.
The results of the independent monitoring are made available internationally within 15 days of each immunization round.
Reports by country are available through the menu on the left.
A woman brings her child to the hujra to be vaccinated with IPV during supplementary vaccination activities in Peshawar, Khyber Pakhtunkhwa, Pakistan. WHO/S.Mugha
In Pakistan, and many other countries around the world, two vaccines – and the committed people delivering them – are working hand in hand to boost immunity in the most vulnerable children and to finish the poliovirus for good.
The vaccines The oral polio vaccine (OPV), which is the vaccine that has been used to interrupt polio around the world, builds immunity in the gut, meaning children who are vaccinated actually spread immunity between them, helping to protect the wider community. The inactivated polio vaccine (IPV) affords blood immunity, building protection for an individual child and is now being used to boost immunity in Pakistan’s most vulnerable children. “OPV and IPV are both safe and effective forms of vaccination against polio. Both confer immunity, but do so in different ways. One way is not better than another; using both forms of vaccine however, is a way of achieving optimal protection against polio,” said Michel Zaffran, Director of Polio Eradication at WHO.
In 2015, Pakistan introduced one dose of IPV into the routine immunization system, in preparation for the global vaccine switch from trivalent OPV to bivalent OPV. The switch, one of the most ambitious projects in the history of vaccines, has been carried out globally as the world gets closer to the worldwide eradication of all strains of poliovirus.
The vaccinators
A local healthcare worker prepares a dose of IPV during the combined OPV/IPV immunization activities in Pakistan. Pakistan is using a combination of both IPV and OPV in campaigns to boost immunity against polio. WHO/S.Mughal
With a second vaccine now being given to children alongside OPV, the role of vaccinators to get vaccines to every child and to answer the questions and concerns of parents is crucial. “Two women from a polio team came to our home and told me that a vaccination team is sitting in one of the hujra (a separate area in many Pakistani homes that is often used for men’s gatherings) nearby to give vaccination to our children, ” said Muhamad Ameen, a 30 year old father from Cantonment area in Peshawar. “I wanted to know why they are giving the same vaccine in syringes now after my children got them in shape of drops few days back. The polio team that came to my home explained to me that it was important for my children’s immunity, and that the two vaccines will protect my children in different ways.”
Unlike OPV campaigns, where the polio teams go door-to-door in Pakistan to reach every child, children can only be vaccinated with IPV by trained vaccinators at specific outreach centers. This means that families have to be informed and able to bring their children to healthcare centres. This can have a huge impact on the number of children that it is possible to reach with the vaccine.
In March, April and May, the parents of more than 2 million of Pakistan’s most vulnerable children lined up at hospitals, health centres, outreach sites and local hujras in parts of the Federally Administered Tribal Areas (FATA), Peshawar, Karachi and Quetta to ensure their children aged between 4 and 24 months received the injection. Amid the regular monthly campaigns, thousands of skilled vaccinators at hundreds of outreach sites vaccinated 2,677,256 children.
The communities
Scorching temperatures, difficult terrain and insecurity are not the only challenges facing vaccinators carrying out their task of delivering the life-saving vaccines. Vaccinators and social mobilisers also battle misconceptions and suspicion about the ongoing immunization campaigns. “Finding a place to vaccinate children is also not easy here because people are suspicious if someone asks to make a vaccination center in his hujra. But I really appreciate work of polio teams working in such harsh conditions,” Muhamad says.
The role of community based social mobilisers during an IPV campaign is critical. It is their job to increase care-givers knowledge of the campaign, to inform them where they can take their child to receive the vaccine, to address any misconceptions and to create an enabling environment where vaccination against vaccine preventable diseases is not only accepted, but expected. “I brought my child when I heard from the team coming to my house that polio injection is provided at the nearby center”, said one mother who did not want her name mentioned. Another father, Gul Hameed from Sufaid Dheri village in Peshawar, says he vaccinated his 12 month old daughter on the first day of the campaign. ”This is important for our children; I do not know why people are resistant to give this vaccine to their children. The polio teams are working very hard in the field. I have deeply observed their work.”
Eradication efforts must continue until we reach every last child in Nigeria WHO/L.Dore
The 24 July marks two years with no case of wild poliovirus in Nigeria – a milestone for the polio eradication programme and an important step toward a polio-free world. Yet there is much still to be done. Nigeria and the African region need to protect the gains made and tackle continuing challenges to eliminate the risk of polio.
A milestone
This month marks the longest Nigeria has ever gone without a case of wild poliovirus, with the country taken off the list of polio-endemic countries in September 2015. Thanks to the hard work of the government, partners, community leaders, health workers and donors, this is the closest the country, and the world, has ever been to ending polio. This important milestone leaves the global community cautiously optimistic that ending polio in Nigeria, and the whole African continent, is within our grasp.
Isa was the final child to contract the wild polio virus in Nigeria. We must leave no stone unturned to ensure that vulnerable children continue to be protected against this devastating virus. (WHO/L.Dore)
Progress in Nigeria
Innovation has underpinned the strong progress seen against polio in Nigeria, including novel strategies and the incredible commitment of tens of thousands of health workers. One hundred and fourteen mobile health teams, developed to access children in the most remote areas, now reach nearly 7,000 settlements across ten states with polio vaccines and other primary health care services. There must be a sustained focus on innovative solutions to issues such as accessibility that continue to leave children in remote areas vulnerable to retransmission of the virus.
A long way to go
While two years with no wild polio in Nigeria is cause for celebration, it must not be a cause for complacency. The recent meeting of the Expert Review Committee (ERC) in Abuja highlighted that there is still a long way to. Polio eradication needs to be kept top of the priority list in Nigeria until the job is done completely and the entire African region certified polio-free. President Muhammadu Buhari called for a reinvigoration of polio eradication efforts whilst receiving WHO representatives earlier this month, emphasizing that ‘‘… we have not recorded any case of polio in the last two years, but we should not be complacent. The breakdown of law and order in the North East has posed challenges to regular immunization.” This vigilance at the highest level is paramount in ensuring that no child is forgotten in the fight against polio in Nigeria.
“We have not recorded any case of polio in the last two years, but we should not be complacent.” President Buhari
The work ahead
Immunization campaigns have helped to secure a polio free future for millions of children across Nigeria but we must continue until we reach every last child (WHO/L.Dore)
Improving the scope of surveillance and immunization activities is vital if Nigeria is to be kept polio-free. At least one more year must pass without a case of wild poliovirus in order for the WHO African region to be certified polio-free. The ERC highlighted the steps that need to be taken to progress towards certification. Investing in strengthening routine immunization must now be the priority of the government and partners in order to sustain the gains of the polio eradication programme and protect children against other vaccine-preventable diseases. It is imperative that these steps are taken in order to make sure that no child is left vulnerable and without adequate immunization
Leaving a lasting legacy
Eradicating polio in Nigeria is already benefitting the health of children across the country more broadly, and has the potential to do even more in the future. The Hard-to-Reach project, operating in high-risk states in Nigeria, exemplifies the wider health benefits that polio eradication efforts bring. The camps are built on the polio infrastructure but offer other services such as antenatal care, routine vaccines, basic medicines, screening for malnutrition and health education, targeting families that lack basic access to healthcare. Find out more about the broader benefits of polio eradication in Nigeria here.
The celebration of two years without a case of wild polio in Nigeria must constitute a call to action to maintain momentum and ensure a polio free Nigeria. This is imperative, with the entire African region drawing closer to possibly being certified polio-free in 2017. Ending polio in Nigeria will be a victory for the country and for children everywhere.
As Nigeria approaches two years with no child paralysed by wild poliovirus, much remains to be done to secure a polio-free world for future generations. WHO/L.Dore
With the two year milestone since the most recent case of wild poliovirus in Nigeria approaching, the Expert Review Committee (ERC) on Polio Eradication and Routine Immunization has emphasised there is no place for complacency to keep the country polio-free.
Meeting in Abuja on 21 – 22 June, the ERC emphasised that the strategy in Nigeria must now shift: from interrupting transmission to staying polio free, sustaining the hard-won gains, strengthening routine immunization and responding to outbreaks of vaccine-derived polioviruses.
Important progress has been made in 2016 with nearly two years having passed since the last case of wild poliovirus was reported in Kano, and the type 2 component of the oral polio vaccine being removed from use in April, as part of a global vaccine switch. Yet the ERC emphasised the need to fill sub-national surveillance gaps, to make significant improvements to routine immunization and to address risks to the programme such as waning political commitment and accountability and the inaccessibility of some populations in the North-East.
Improving immunity and strengthening surveillance
Strengthening surveillance in Nigeria relies on outreach to many members of communities in the most vulnerable areas of the country, including traditional healers. WHO/L.Dore
The ERC assessed that recent supplementary immunization activities in Nigeria have been of good quality, with the number of children missed going down. This has been thanks to programmatic improvements such as activities in between campaigns at religious gatherings, and hit-and-run activities in inaccessible areas to rapidly protect vulnerable children. In newly accessible areas, innovations such as expanded age range campaigns are being considered to rapidly increase immunity in as much of the population as possible.
Overall, the ERC recognised that surveillance in Nigeria is strong, but with sub-national gaps that still need to be addressed. The ERC recommended determining how resources could be optimally used to fill these gaps. Both surveillance for acute flaccid paralysis and environmental surveillance have important roles to play in the coming years. Only once three years have passed in Nigeria with no case of wild poliovirus and strong surveillance systems can the WHO African Region be certified as polio-free, making the strengthening of s
Stopping all polioviruses
As well as keeping Nigeria free from wild polio, the ERC also recognised steps to stop vaccine-derived polioviruses (VDPVs). In April, Nigeria successfully implemented the trivalent to bivalent oral polio vaccine switch, withdrawing the type 2 component of the oral polio vaccine alongside 155 other countries and territories worldwide within a two week period. In the long term, the switch will play an essential role in stopping the emergence of strains of type 2 vaccine-derived poliovirus outbreaks, which can emerge when routine immunization coverage is inadequate. The ERC also commended Nigeria for the successful campaigns that were carried out to make sure that immunity against type 2 was high at the time of the switch across the whole country.
Nigeria has seen one outbreak of circulating VDPV type 2 this year, in Borno state, in a sample taken from the environment on 23 March, before the switch took place. In response, the Director General of WHO approved the release of monovalent oral polio vaccine type 2 for up to three rounds to build immunity and stop the outbreak. The ERC congratulated Nigeria for their rapid response to this outbreak, with innovations and detailed micro-plans ensuring strong coverage and also recommended that Nigeria consider the possibility of using fractional dose inactivated polio vaccine for outbreak response strategies to further build up immunity against all types of poliovirus.
Strengthening Routine Immunization
Mothers gather at a health camp in northern Nigeria to get vaccines against polio and other diseases for their children. WHO/L.Dore
The ERC was encouraged by the efforts of the Government of Nigeria and partners to improve routine immunization services. In particular, they noted the role of the polio eradication Emergency Operation Centers in improving logistics and tracking routine immunization coverage in 56 priority Local Government Areas. Yet with insecurity and insufficient coverage in some northern states, the ERC emphasised that investing in strengthening routine immunization through a comprehensive primary health care strategy must now be the priority of the government and partners in order to sustain the gains of the polio eradication programme and protect children against other vaccine-preventable diseases.
Transition Planning
The ERC also reviewed Nigeria’s progress towards planning for the ramp down of polio eradication funding in the coming years once eradication is achieved, and the potential to transition the polio assets and infrastructure to help meet other health needs. Nigeria is currently mapping the polio funded assets of both partners and the government, and is beginning to document lessons learned from the last few decades of polio eradication efforts in order to share their insights with other health programmes. The ERC recommended that the transition planning process align the redeployment of polio assets with the priorities and gaps of the primary health care system. A plan for transition should be completed by the end of 2016, driven by the government and with input from a broad range of polio and non-polio stakeholders, including donors.
Keeping Nigeria Polio Free
With progress made and challenges ahead, continued efforts in Nigeria are as crucial as ever in the light of two years with no wild poliovirus. With two remaining endemic countries – Pakistan and Afghanistan – no unimmunized child anywhere in the world is free from the threat of polio, especially where routine immunization is weak. Stakeholders of the polio eradication programme in Nigeria must continue full pelt until the continent has been certified free from the virus.
Environmental surveillance officers in Nigeria check a water source for evidence of polio. WHO/L.Dore
In a small health clinic in Tharaka Nithi in Kenya, Amina Ismail pours over a register documenting all of the doctors’ appointments from recent months, a nurse by her side. She is checking every record for symptoms of polio – the sudden onset, floppy arms and legs that signify acute flaccid paralysis (AFP). As they work, she checks that the nurse knows what the symptoms are, and that she knows what she has to do if a child with AFP is brought to the clinic. This detailed surveillance for polio, working hand in hand with those who know their communities best of all, has been the lynchpin of the work of the Global Polio Eradication Initiative (GPEI).
Surveillance officers like Amina work and volunteer around the world with one aim: the eradication of the poliovirus. Networks of health workers, traditional healers, religious leaders, teachers and parents have helped us identify paralysed children; and then by testing their stool samples in laboratories, we can find out if polio was the cause. This information has enabled us to hold vaccination campaigns to rapidly increase immunity in places where the virus is circulating, to protect children against paralysis and ultimately remove any hiding place for the virus so that it dies out. Once we have successfully done this everywhere in the world, polio will be eradicated.
Amina Ismail, right, checks appointment registers for cases of polio – an essential part of surveillance efforts to trace this devastating disease. WHO/L.Dore
We have never been so close to our goal of a polio-free world. There are just two countries left where wild poliovirus is still circulating – Afghanistan and Pakistan. This means that the partners of the GPEI along with country governments, donors, civil society and parents are working harder than ever before to make sure we know exactly where polio is, so that we can respond quickly to stop every strain of the virus.
Surveillance is one of the most important jobs done to eradicate polio. And today, as fewer countries actually have cases to be found through acute flaccid paralysis surveillance, new and innovative approaches are being used to find viruses even before they cause symptoms.
It is five thirty in the morning in Kano in the north of Nigeria. As the sun comes up and people begin to wake and gather at market stalls, in traffic jams and by small fires on street corners, two men stand by an open sewage system. The men put on protective coats and gloves and carefully lower a small bucket down amongst to collect a small amount of the slow-moving water. They package it carefully, take off their gloves, carefully place it in a cool-box and the sample begins its journey to the polio laboratory.
By testing water in the environment for the poliovirus, alarm bells can be sounded ahead of time if children in any area could be at risk. Surveillance officers can be thought of as the doctors who test the world for polio. AFP surveillance helps us to find symptoms that have already surfaced, and environmental surveillance helps us identify even those infections that haven’t shown up yet. Both are essential, in countries across the world – not just where polio remains – to take us across the finishing line.
As Director of Polio Eradication for WHO, I depend on thousands of people, including committed Rotarians, to vaccinate children, research new ways to deliver these vaccines, to plan and advocate and mobilise essential resources. Tracing every last poliovirus through surveillance is a crucial part of these efforts, showing us the symptoms so that we can prevent disease in the first place. Keeping surveillance efforts going in all countries is a huge undertaking requiring skill, vigilance and continued funding if we are to achieve our goal. And what a monumental achievement that will be – all future generations, free from the threat of polio.
The World Health Organization’s Global Polio Eradication Initiative (WHO/POL) is looking for Expressions of Interest from private or public sector vaccine manufacturers in developing countries interested in collaborating with WHO and Intravacc in the development, manufacture and distribution of a safe effective and affordable Sabin Inactivated Polio Vaccine (sIPV), that can be produced securely in developing country settings.
In September 2015, WHO officially removed Nigeria from its list of polio-endemic countries, after the country reported its last wild poliovirus case in July 2014. Many factors led to this historic public health success. The reputable public health publication, Journal of Infectious Diseases, in February 2016 published a supplement on Nigeria’s polio eradication effort. The supplement features a series of topic-specific scientific articles, summarising the various aspects which led to success in Nigeria, such as: innovative ways to improve microplans; improving surveillance; engaging communities, optimising vaccine mix; systematically linking with routine immunization services; and improving overall programme management to ensure greater accountability, direct disbursement mechanisms to vaccination teams and effective oversight of an intensified technical emergency surge capacity project. These tactics are being replicated in the remaining endemic countries, and are already showing great success. The full supplement and its articles can be accessed here.
The polio infrastructure in Nigeria has protected children across the country against polio by interrupting the transmission of the virus, but there is more still to do for the health of the country’s children. WHO/L.Dore
It has been 18 months since Nigeria, once considered one of the biggest challenges to global polio eradication, saw a child paralysed by wild poliovirus. Yet this tremendous achievement, tribute to the hard work of many across the country, is not the end of the road for Nigeria’s polio programme. Now is the time to build resilience against the virus; and also to seize the opportunity to plan for how the polio infrastructure can make a sustainable difference to the health of some of the most vulnerable communities long into the future.
This year, countries with strong polio programmes, including Nigeria, are planning for how to transition the expertise of their human and technical infrastructures to other health programmes, once a polio-free world has become a reality.
“Becoming polio-free gives such a boost of confidence to countries,” explains Dr Hamid Jafari, former Director of the Global Polio Eradication Initiative. “Success in public health breeds more success; this is happening in Nigeria right now.”
In February, Ministers of Health from across Africa will gather at the first Ministerial Conference on Immunization to find solutions to the challenges facing their routine immunization systems. The polio programmes in countries like Nigeria have important lessons to offer routine immunization across the region; from ensuring equitable access to vaccines and engaging communities even in the most remote places, to the role of political leadership and accountability in protecting children against vaccine-preventable diseases.
Political leadership
Planning must begin now so that the polio infrastructure can have a lasting impact on child health long into the future. WHO/L.Dore.
In 2012, 122 children were paralysed by polio in Nigeria. The tide changed when the Government of Nigeria took ownership of the programme, setting up the National Polio Emergency Operations Centre to bring together the expertise of partners, ensure accountability and coordination, and to introduce data-driven, innovative solutions. The impact of this spread far beyond polio, strengthening routine immunization and even helping to coordinate the emergency responses to the Ebola outbreak in 2014 and the current Lassa fever outbreak.
“Becoming polio-free gives such a boost of confidence to countries,” explains Dr Hamid Jafari, former Director of the Global Polio Eradication Initiative. “Success in public health breeds more success; this is happening in Nigeria right now. Everyone at all levels becomes more willing to take on huge challenges because they are riding on momentum of polio eradication.”
Boosting routine immunization coverage
The polio programme is helping to build the capacity of the routine immunization system in Nigeria to protect children against other vaccine preventable diseases. WHO/L.Dore
The polio programme in Nigeria has long worked hand-in-hand with routine immunization, but with low routine immunization coverage in the past, campaigns were necessary to boost immunity to a level that would stop transmission. Yet as the polio programme increased in strength, the relationship between the two meant lessons – on building community support, strengthening logistics and accountability and using data to inform action – had a roll-on impact. Between 2012 and 2015 in Kano, the number of children reached with all necessary doses of the oral polio vaccine increased from 61% to 94%; and the number of children reached with the full set of doses the pentavalent vaccine rose from just 41% to 91%.
The people who make things happen
Volunteer community mobilisers play an essential role in educating parents about the importance of vaccines, and sometimes even bring newborn babies for their first doses. WHO/L.Dore.
The surge in polio capacity resulting from increased government commitment has brought over 12,000 volunteer community mobilisers (VCMs) and field volunteers to engage and inform communities on the importance of polio by visiting every home. Most often women with trusted positions in their villages, such as teachers and traditional birth attendants, VCMs are able to provide mothers with important information that goes beyond polio, such as the importance of routine vaccines, nutrition and hand-washing. Religious leaders engaged through the polio programme played an important role in addressing vaccine hesitancy in the country, and their influence is now helping to encourage families to get their children vaccinated against other diseases, alongside polio.
Health camps provide an opportunity to reach remote communities with polio vaccines alongside other health services such as antenatal care for pregnant women. WHO/L.Dore
Going the extra mile
The Hard-to-Reach project is operational in 10 high-risk states in Nigeria. In Kano state alone, the project brings vaccines against polio and other preventable diseases to 432 remote settlements in Kano that house-to-house polio teams were struggling to access. The camps are built on the polio infrastructure but offer other services such as antenatal care, routine vaccines, basic medicines, screening for malnutrition and health education, which are desperately needed by families with no other access to healthcare.
A unique opportunity
Now is the time to plan for the future of projects like this, where the lessons learned and capacity built over the last three decades through polio eradication are playing an important role in other programmes. Governments have the opportunity to work with civil society, the health sector and donors to integrate polio funded infrastructure into ongoing public health programmes, so that the investments made in polio eradication continue to have an impact long into the future.
“It would be a very sad story if health camps like these were to stop,” said Dr Muhammad Sani Umar, the focal point for routine immunization for WHO in Kano. “However, we are discussing with the state on the sustainability of these projects to develop a plan together. My vision is for us to use the polio infrastructure to strengthen routine immunization, ensuring a better life for our children.”
“It will take a lot of work to sustain the progress we have made against polio in Nigeria, needing quality campaigns and surveillance, and also the improvement of routine immunization,” explained Dr Ado Mohammed, the Executive Director of the National Primary Health Care Development Agency for Nigeria.
As we near global polio eradication, the public health community has a chance to make the most of the experience, lessons, structures and people from the programme who are already doing so much for the health of children in countries across Africa.
Shri J P Nadda, the Union Minister for Health and Family Welfare, launched the injectable Inactivated Polio Vaccine (IPV) in India in November, announcing that “… at this momentous milestone, India remains committed to Global Polio Eradication.”
The Health Minister stated that in a landmark step to provide double protection to our children and securing our gains of polio eradication, the Government of India is introducing one dose of IPV into its routine immunization program alongside the oral polio vaccine. The vaccine will initially be introduced in six states: Assam, Gujarat, Punjab, Bihar, Madhya Pradesh, and Uttar Pradesh. New evidences now clearly show that IPV and OPV together will further strengthen the children’s immune system and will provide double protection against polio, explained the Health Minister.
The South East Asia and Pacific region was declared polio-free in 2014 after three years with no cases in India. Yet with bordering Pakistan still reporting cases of polio, the introduction of IPV into routine immunization programmes will provide an important boost to the immunity of children in India against all types of poliovirus.
By the end of the year, more than 80 % of the global birth cohort will be routinely receiving due to the largest globally synchronised vaccine introduction in history.
“We are utilizing the opportunities to intensify our efforts to ensure full immunization of all children in the country. Every new vaccine introduction gives us the added opportunity of health system strengthening. As part of this introduction we have trained our health officials and frontline health workers”, Shri J P Nadda said.
The Health Minister thanked and congratulated all state governments and the supporting organizations like WHO, UNICEF and Rotary International etc. for partnering in this endeavour. He expressed his gratitude toward the frontline health workers for achieving unique success of polio eradication in the sphere of public health.
Smt. Poonam Khetrapal, Regional Director, SEARO (WHO) stated that launching IPV in India is a historic moment and will further cement India’s achievements on polio to date. She said it is necessary step to eradicate polio virus from the world. She also applauded the Government of India for its commitment to eradicate polio.
Mr. Michael McGovern, International PolioPlus Committee of Rotary International commended India for its success in keeping the country polio-free, and said that Rotary will always support the country’s polio eradication efforts. Rotarians across India played an essential role in stopping polio in India, and are making just as important a contribution to keeping the country polio-free.
Mr. Louis-Georges Arsenault, UNICEF Representative for India commended the strengthening of India’s immunization programme by introduction of IPV and termed this as a “monumental step”. He reiterated commitment and support of UNICEF in India’s immunization endeavors.
The Bill & Melinda Gates Foundation, Norway, and the United Kingdom are generously supporting the introduction of IPV in routine immunisation schedules in 72 Gavi-supported countries, while Canada is supporting its introduction in other lower-middle income countries. The top ten government donors to GPEI include the USA, the UK, Japan, Germany, Canada, the Netherlands, Norway and Australia.
The Global Polio Eradication Initiative (GPEI) is led by national governments and spearheaded by the World Health Organization (WHO), Rotary International, the US Centers for Disease Control and Prevention (CDC), and the United Nations Children’s Fund (UNICEF), with the support of the Bill & Melinda Gates Foundation.
Since its launch at the World Health Assembly in 1988, the GPEI has reduced the global incidence of polio by more than 99%. The GPEI receives financial support from governments of countries affected by polio; private sector foundations, donor governments, multilateral organizations, private individuals, humanitarian and nongovernmental organizations and corporate partners.
The World Health Organization announced today that Nigeria is no longer polio endemic. This is the first time that Nigeria has interrupted transmission of wild poliovirus, bringing the country and the African region closer than ever to being certified polio-free.
The Global Polio Eradication Initiative (GPEI), the public-private partnership leading the effort to eradicate polio, called this a ‘historic achievement’ in global health. Nigeria has not reported a case of wild poliovirus since 24 July 2014, and all laboratory data have confirmed a full 12 months have passed without any new cases.
As recently as 2012, Nigeria accounted for more than half of all polio cases worldwide. Since then, a concerted effort by all levels of government, civil society, religious leaders and tens of thousands of dedicated health workers have resulted in Nigeria successfully stopping polio. More than 200,000 volunteers across the country repeatedly immunized more than 45 million children under the age of five years, to ensure that no child would suffer from this paralysing disease. Innovative approaches, such as increased community involvement and the establishment of Emergency Operations Centres at the national and state level, have also been pivotal to Nigeria’s success.
The interruption of wild poliovirus transmission in Nigeria would have been impossible without the support and commitment of donors and development partners. Their continued support, along with continued domestic funding from Nigeria, will be essential to keep Nigeria and the entire region polio-free.
Polio, which can cause lifelong paralysis, has now been stopped nearly everywhere in the world following a 25-year concerted international effort. Polio remains endemic in only two countries – Pakistan and Afghanistan. The eradication of polio globally now depends primarily on stopping the disease in these countries. As long as polio exists anywhere, it’s a threat to children everywhere.
Nigeria has made remarkable progress against polio, but continued vigilance is needed to protect these gains and ensure that polio does not return. Immunization and surveillance activities must continue to rapidly detect a potential re-introduction or re-emergence of the virus. After three years have passed without a case of wild poliovirus on the continent, official ‘certification’ of polio eradication will be conducted at the regional level in Africa.
Eradicating polio will be one of the greatest achievements in human history, and have a positive impact on global health for generations to come. Nigeria has brought the world one major step closer to achieving this goal and it’s critical that we seize this opportunity to end polio for good and ensure future generations of children are free from this devastating disease.
Dr Arshad Quddus is the coordinator of the Polio Strategy Support and Coordination unit at the World Health Organization (WHO). In August, he took part in the meeting of the Expert Review Committee (ERC) in Nigeria. Here, he speaks about the extraordinary efforts in Nigeria to date, the work still to be done, and what motivates him to eradicate polio.
What was the purpose of the ERC meeting in Nigeria last week?
This ERC meeting in Nigeria reviewed the progress made in Nigeria and identified the ways and means to strengthen the gains of the last few years. Finally, the committee identified the major risks and advised the Nigeria team on how to address them.
Nigeria has recently passed a big unofficial ‘milestone’ with one year of no wild poliovirus cases confirmed. What factors are responsible for this progress?
I think there has been remarkable progress with extraordinary efforts made to achieve it. There have been a number of innovations that the programme has incorporated that can be labelled as game changers. The most important of these was getting political commitment at all levels, with the engagement of the President, religious and traditional leaders, as well as the community networks. By improving accountability frameworks with clearly described roles and responsibilities, establishing health camps in some of the very difficult to reach areas, developing new strategies to vaccinate children, substantial progress was made.
How confident do you feel in the progress seen in Nigeria against wild poliovirus?
The ERC review has increased our level of confidence because it reviewed the situation very critically. It seems like Nigeria’s surveillance system has improved overall because it is showing better indicators, and because no case of WPV or positive environmental sample has been found in the last year. So there is a degree of confidence in this progress that has been made in Nigeria. Having said that, we know that pockets of low immunization coverage remain in some of the high-risk areas. That is why everyone needs to redouble their efforts to fill all the remaining gaps, both in vaccinations and in surveillance.
What are the risks to polio eradication in Nigeria now?
During the ERC everybody agreed that the important thing is to build on the gains, and to do that we need to be aware of the risks. There are expanding areas of insecurity and inaccessibility, particularly in Borno and Yobe in the north east. There are still pockets with low immunization coverage in Kano, Kaduna, Sokoto and Katsina. The programme really has to focus on these areas to improve population immunity and to fill residual surveillance gaps. There is a third big risk that the sense of achievement could lead to complacency that the job is done. There is still a long way to go. Polio needs to be kept top of the priority list until the job is done.
What does the programme have to do to target those areas of insecurity in the north east?
The programme has rich experience in reaching children in insecure and inaccessible areas. For example, permanent transit teams vaccinate any children going in or out of those areas; there are campaigns that seize on windows of opportunity as and when areas open up. We are also scaling up surveillance and immunization activities in camps for the internally displaced populations and enhancing coordination with countries where the population of these conflict-affected areas have moved, such as Cameroon and Niger. In addition we are expanding environmental surveillance, including to key urban areas in Borno.
What are the three key things Nigeria has to do to ensure it becomes polio-free?
Nigeria has to maintain the highest possible level of protection through immunization coverage, and figure out how to reach the children we are currently missing. This is the time for Nigeria to be very vigilant and alert and to redouble its efforts, which means they have to make sure that the surveillance system is strong and gaps are filled. And thirdly, we have to continue to have the highest level of political commitment and to enforce accountability.
Do you think we are close to overcoming the remaining challenges?
I think this recent progress in Nigeria paves the way for Africa to become polio free. It is challenging, but the recent progress that is being made is encouraging. Certainly Nigeria, and Africa, is closer than ever. But even if Africa finishes the job, a lot will depend on how quickly we progress in Pakistan and Afghanistan. We know from past experience how quickly and how far poliovirus can spread. But we are very, very close. We are at the brink of achieving eradication.
What motivated you to work in polio eradication?
I joined this programme in 1999. In those early days, the sense that eradication was achievable if we just improved immunization pulled me in. I spent ten years working in Afghanistan. Vaccinating children in those conflict-affected and difficult to access areas was very challenging. We would work to find additional children to immunize, protecting them not only from polio but also from other vaccine preventable diseases. There was always a sense of achievement and satisfaction in trying to overcome these challenges.
A project to improve access to hard-to-reach (HTR) populations in Nigeria with polio vaccines is having a dramatic impact on the broader health needs of remote communities in Yobe, Nigeria. In July and August, despite escalated insurgency, in addition to over 95,000 doses of trivalent oral polio vaccine the HTR project has delivered over 90,000 doses of vitamin A supplements and over 99,000 deworming tablets to isolated communities in need of medical care. What’s more, over 19,000 pregnant women received Iron Sulfate supplements and over 12,000 received preventative malaria therapy.
The HTR project was set up to access the most marginalised and disadvantaged communities in northern Nigeria with essential vaccines. This July, the Government of Nigeria committed to continuing to fund HTR teams in order to reach pregnant women and children residing in difficult terrains and security-compromised areas. The HTR teams also bring life-saving medicines, child survival and maternal health care services and health education to improve general wellbeing to these communities who are so often underserved.
The HTR scheme’s ability to protect children who were previously being missed on vaccination campaigns has been instrumental in achieving over a year with no reported case of polio in Nigeria, by going to great lengths to get to remote communities every three months. Yobe in Northern Nigeria has a relatively small and dispersed population, many of whom live in rural areas made difficult to access through a challenging terrain of dry desert and regional insecurity. This made vaccination activities both time-consuming and logistically challenging for those working to stop the virus in its tracks.
The world is on the verge of achieving global polio eradication. With nearly three decades of experience as one of the largest ever global health initiatives, the lessons learned and knowledge generated must be shared to contribute to real, sustained changes in other global health programmes.
Projects such as this in Nigeria are a living example of what the polio legacy can achieve to improve health using the programme’s expertise in reaching the most chronically neglected and underserved communities. The polio infrastructure has also played an important role in other projects. The experiences, staff, skills and Emergency Operations Centres of the polio eradication effort in Nigeria were vital for the response to the deadly Ebola outbreak when it spread into the country, and beyond across western Africa.
The eradication of polio will achieve something remarkable, eradicating a disease for only the second time in history and ensuring that future generations never again have to fear polio. But this legacy can reach much further, impacting the health of countless people by strengthening systems and helping services to take extra steps to support underserved communities. This is both an opportunity and an obligation to build a better future.
Find more information and resources on the Global Polio Eradication Initiative’s legacy objective here.
Today marks one year since Nigeria’s last reported case of wild poliovirus paralyzed a child. Final laboratory results on all specimens from acute flaccid paralysis cases and environmental samples for the full 12 month period are expected by September 2015. The Global Polio Eradication Initiative commends the hard work of the Nigerian government, partners, religious and community leaders, and health workers for such strong progress towards stopping polio.
While Nigeria is closer than ever to ending polio, the job is not yet finished. At least two more years must pass without a case of wild poliovirus for Nigeria to be certified polio-free along with the rest of the WHO’s African region. To achieve this goal, Nigeria and all countries in Africa must maintain domestic funding for polio, ensure high-quality surveillance for poliovirus, strengthen vaccination campaigns, particularly in hard-to-reach and insecure areas, and improve routine immunization. At the same time, until polio has been eradicated from all remaining infected areas, all countries must maintain high immunity levels and strong disease surveillance to minimize the risk and consequences of re-infection.
Ending polio in Nigeria will be a victory for the country and for children everywhere and bring the world much closer to being polio-free.
During more than 25 years of operations, the Global Polio Eradication Initiative has mobilized and trained millions of volunteers, social mobilizers, and health workers; accessed households untouched by other health initiatives; mapped and brought health interventions to chronically neglected communities; and established a standardized, real-time global surveillance and response capacity.
As the initiative nears completion, the primary goals of transition planning for the GPEI are both to protect a polio-free world and to ensure that these investments, made to eradicate polio, contribute to future health goals after the completion of polio eradication.
With the introduction of two new vaccines, Bangladesh’s Extended Program on Immunization now protects children against 10 diseases. GAVI
On 21 March, the Extended Program on Immunization (EPI) in Bangladesh launched both the Inactivated Polio Vaccine (IPV) and the Pneumococcal Conjugate Vaccine into their Routine Immunization programme. With polio stopped in 2000 and 94% routine coverage by 2 years of age, Bangladesh has many lessons to share with other countries on how to provide strong protection against vaccine preventable diseases.
IPV Introduction in a Strong Routine Immunization System
EPI in Bangladesh is remarkable for the ownership felt for the program at all levels, from the Government to health workers to parents who actively seek out vaccines. This commitment is evident in the dual introduction for IPV and PCV, which enabled streamlining on training, logistics and the health workforce.
Movement around the country has been limited since January, due to road blockades for political reasons, giving the introduction a challenging backdrop. Innovative transportation techniques, the incredible commitment of staff and the power of the yellow EPI banner which shines out from every vehicle and denotes every EPI clinic made it possible to get the new vaccines to healthcare centres, despite the challenges.
Before any vaccine introduction, a cascade of improvements for the entire EPI system takes place. To accommodate two new vaccines into the system, international partners helped government to assess cold chain capacity, secure vaccine stocks, train all health workers and engage influential leaders. Dr Abdur Rahim, Program Manager of EPI at the Ministry of Public Health, explained: “Every time we introduced a new vaccine in the past few years, we saw an increase in overall coverage.” He hopes that this dual introduction will provide the necessary push to bring coverage to 90%.
With the addition of IPV and PCV, Bangladesh is now protecting children against 10 diseases. “This makes Bangladesh one of the model countries in South Asia, with many lessons to share with the rest of the world,” said Dr Jayantha Liyanage from WHO at the launch on March 21.
Polio’s Contribution to Bangladesh’s EPI System
Bangladesh’s historic success in stopping polio in 2000 set the foundation that enabled this introduction. The capacity of staff, lessons learned over many years of National Immunization Days (NIDs) and high community engagement all contributed to the strength of the system today, which is remarkable in a low income country with such a high birth cohort and many other public health challenges.
Bangladesh is an example of a country where routine immunization and polio eradication have worked in synergy for so long that the former now carries the latter. This process of synergy gained its strength from the way in which partnerships grew between the government, organizations such as WHO, UNICEF and Rotary International, and civil society organisations. The longstanding history of the program means that all stakeholders know their roles well, explains Dr N. Paranietharan, Head of WHO Country Office in Bangladesh. “There may be new challenges; however the public health approaches to respond to them remains the same.”
Bangladesh is an example of a country where routine immunization and polio eradication have worked in synergy for so long that the former now carries the latter.
Years of NIDs established and strengthened channels of communication, building all-important trust between the people and the EPI system. NIDs became festive occasions across the country, with Rotary and UNICEF doing everything they could to engage parents in the campaigns, with elephants, balloons, and music in the streets. “Just a generation or two ago, vaccine preventable diseases caused so many deaths, and now so few. This is incredible, visible change. When people saw vaccinated children staying healthy, it motivated the whole country,” describes Dr Abdur Rahim. “All walks of life have contributed to this program, so they all are committed to ensuring it remains strong and continues to improve.”
Bangladesh now faces the challenge of addressing inequity in coverage. Urban areas prove a particular challenge, where population movements, low levels of sanitation in slums and a less structured infrastructure need to be addressed.
Working for a Stronger Future
While polio has not been seen in the country since the end of the outbreak in 2006, the programme continues to play a role in helping to address the challenges of the entire system. “We are keeping our commitment to polio eradication strong, despite not having seen the disease for so many years. It is important for us to avoid the risk: as long as neighbouring countries are vulnerable to polio, awareness of the threat needs to be maintained,” explains Dr Paranietharan. “But the efforts aren’t just for polio. Polio eradication is so integrated that all the efforts are towards strengthening systems for routine immunization.”
In January 2015, 26 surveillance experts from the National Polio Surveillance Programme (NPSP) in India boarded a plane that would take them to western Africa. Amongst them, Dr Deepak Kumar and Dr Aarti Singh were not only moving to work in a new and challenging country; they were also going to adapt their expertise to a fight a new disease: Ebola.
Knowing how to find a disease
The principles of disease surveillance are the lifeblood of the global polio eradication programme. Networks span entire countries, from remote villages where traditional health workers are taught to identify symptoms to cities where water sources are tested for the poliovirus. It has been this real-time, precise knowledge of the presence and patterns of the poliovirus that has enabled the reduction of polio by 99 per cent globally. India, once seen as the biggest challenge to polio eradication, became polio-free in 2014, three years after the last case in 2011.
By deploying surveillance experts from the team at the heart of this success to Liberia and Sierra Leone, the NPSP is demonstrating the much broader impact that polio staff, expertise and infrastructure can have for other health and development needs.
Applying lessons from polio to Ebola
Dr Deepak Kumar has worked in public health for 14 years, yet has never seen an epidemic that has cost so many lives as the Ebola outbreak in western Africa. Faced with a health system that was unable to deal with the needs of the population to start with, and a surveillance system still in its infancy, his role is to help bring together data collected from district levels to create a cohesive picture of what is happening on the ground so that national plans are well informed. Dr Aarti Singh is working in the Western Area of Sierra Leone to strengthen the data gathering processes that feed into the national picture that Dr Kumar is helping to construct.
Dr Singh, who has worked in public health for the last 16 years, spends her days visiting houses where there have been alerts of possible Ebola infections, to gather the information that a strong surveillance system relies on. She helps to create exhaustive lists of the contacts of infected individuals who must go under quarantine, and by working closely with local staff, can build capacity through hands-on training.
Trust is the most valued commodity for those working both to stop the spread of the virus and to gather accurate data; families must be convinced of the importance of ignoring the social stigma attached to infection that stops so many reporting cases, and of not leaving the house when under quarantine. While the government is trying to supply these households with the food and water they need, they are often in short supply, and many families are hesitant to submit themselves to 21 days without being able to work. Keeping regular contact with families helps to build their faith in health workers, and is also a chance to reinforce the hygiene habits that help to stop transmission.
Data is personal
Data collection at this level is far removed from spread sheets and number crunching. Each case is investigated personally, each person interviewed, informed, reassured, contact lists painstakingly constructed and double-checked. Only then does each case get inserted into a database, feeding up to the country level so that the response plan can be informed by accurate data. This is living surveillance, enmeshed at every turn with the lives of people struggling to recover normality following a year of the virus destabilising everything around them.
Dr Kumar is struggling with gaps where the picture is still not clear enough to inform a strong response. He has found one of the largest challenges to be the segmentation of surveillance into districts, leaving vulnerable populations along borders where the virus has continued to circulate unchecked. Drawing on his experience negotiating between micro-planning and regional overviews in India, he has encouraged neighbouring District Teams to plan in a more coordinated manner.
Building resilience
The innovations that the Indian team can bring from polio will impact more than the Ebola outbreak alone. The experts deployed from India will leave behind the legacy of a strengthened data system that will transform the current response and disease surveillance in the future. By working with health workers on the ground to representatives from the Ministry of Health, they are building capacity and strengthening resilience.
Both Dr Singh and Dr Kumar have also gained insights that they will be taking back to their work on polio in India. Most importantly, both identified the importance of being prepared for outbreaks. While no case of polio has been found in India for 4 years, the continued transmission in neighbouring Pakistan leaves children without immunity against polio vulnerable. This heightened awareness, gathered in the context of the devastation caused by Ebola in western Africa, will spur Dr Deepak Kumar and Dr Aarti Singh to maintain the strength of surveillance systems back home, to ensure that polio does not return to India. Both polio and Ebola are examples of the incredible things that can be achieved to improve health by sharing knowledge and experience across health systems.
Read more on the work of Dr Singh and Dr Kumar here.
The first child in the Federal Capital Territory receives the inactivated polio vaccine WHO/AFRO
This February, Nigeria became the first polio endemic country to introduce the inactivated polio vaccine (IPV) into its routine immunization system. The Minister of Health, Dr Alhassan Khaliru, described this as “… a quantum-leap opportunity for Nigeria in the polio eradication endgame strategy”.
The introduction of IPV into routine immunization systems is part of one of the four major objectives of the Global Polio Eradication Initiative (GPEI). In May 2012, the World Health Assembly called on all countries which were using only the oral polio vaccine (OPV) to introduce at least one dose of IPV into routine immunization schedules by the end of 2015. This is the largest globally coordinated vaccine introduction project in history.
The launch in Nigeria was supported by the partners of the GPEI, including the Nigerian Government, the World Health Organization, UNICEF, Rotary International, the Centers for Disease Control and Prevention and the Gavi Alliance. Speaking at the launch ceremony, the Minister stated that combining OPV and IPV had threefold benefits: acting as risk mitigation in the global plan to phase out the use of OPVs in 2016, boosting immunity against type 1 and 3 wild poliovirus (WPV) and also tackling the risk of circulating vaccine-derived poliovirus (cVDPV).
While OPV is extremely safe and has led the world to the threshold of being polio-free, on very rare occasions its use can lead to vaccine-associated cases. For this reason, the global eradication of polio requires the cessation of all OPV use, once polio has been eradicated. IPV will then be the only option for countries to maintain immunity levels.
IPV will be introduced in phases. This first phase has introduced IPV in 2 northern endemic States, Bauchi and Jigawa, while the second phase will see the vaccine introduced in the remaining states by 16 March 2015.
Nigeria remains one of the last three countries with endemic WPV transmission, and is also struggling with an outbreak of cVDPV. Significant progress has been made in the past year against WPV, with increased government ownership of the programme and innovative approaches in recent years leading to no cases having been reported for seven months. Yet the World Health Organization Country Representative, Dr Rui Gama Vaz, cautioned against complacency in finishing polio in the country as there are still risks of circulation and re-infection.
Eradicating polio depends on reaching every child with vaccines, whether through campaigns or routine immunization systems. Nigeria introduced IPV in mass polio campaigns in 2014 with more than 3 million doses administered to children 14 weeks to 59 months of age in high risk areas. There are significant positive trends in improving routine immunization coverage with the reported OPV3 coverage of 67% in 2013 compared with 54% in 2010. However, this is still well below the goal of reaching at least 80% of children with reliable routine immunization systems.
While the programme has made significant progress against polio in Nigeria, continuing to strengthen routine immunization and health systems will be crucial to maintain and magnify the gains of recent years.
On the 21st and 22nd of January, the Expert Review Committee (ERC) on Polio Eradication and Routine Immunization in Nigeria met in order to discuss progress and challenges against the virus in the last polio endemic country in Africa.
In January, six months passed since the most recent case of wild polio virus was confirmed in Nigeria, with onset of paralysis on the 24 July 2014. This encouraging progress in Nigeria has led to a cautious optimism that the innovations of the programme in the past two years have led to greater protection for children.
This 29th meeting of the ERC concluded that Nigeria has a long way to go before this tentative progress can be taken as evidence that transmission of the virus has stopped. The ERC stressed that Nigeria will remain on the World Health Organization’s list of polio endemic countries until no wild poliovirus has been detected for a period of at least 12 months, dependent on the systems of surveillance being of certification quality. The wider certification of the African region as being polio-free will take at least three years.
With a strong and reliable surveillance system so crucial to the eventual certification of Nigeria and the African region as polio free, the ERC stated the importance of continuing to improve environmental and surveillance and acute flaccid paralysis surveillance.
In preparing to finish polio, the ERC stated that Nigeria must address several threats to the interruption of transmission. Firstly, while the country is in a better position than ever before to end polio for good, it is essential that complacency regarding progress does not lead to a loss of momentum for the national programme. With elections this month in Nigeria, ensuring that political commitment is maintained, that the scheduled introduction of IPV goes ahead and that programmes continue to operate are essential for not letting progress slip.
With the national elections on the 14th February, it is possible that political attention and support will be diverted. With polio still a way off being eradicated in Nigeria, the ERC recommended that an advocacy plan be developed to ensure support in high risk areas and to ensure continued engagement across political parties, traditional and religious leaders, and civil society.
Despite the reduction in the presence of wild poliovirus, Nigeria has seen recent cases of circulating vaccine derived poliovirus type 2 (cVDPV2), with the most recent onset of paralysis in November 2014. It is essential the Nigeria stop every chain of cVDPV transmission if Africa is to reach a polio-free status. Ensuring that inactivated polio vaccine introductions in February go smoothly and preparing for the April 2016 withdrawal of trivalent OPV are crucial steps in ending cVDPV transmission.
Nigeria plays a crucial role for the whole of the African continent in ensuring that the threat of polio is removed for good. Therefore the ERC emphasised the importance of cross-border coordination with Cameroon, Chad and Niger to ensure that populations living on the borders are reached with vaccines, and that surveillance systems support and feed in to one another.
The second threat to eradication in Nigeria identified by the ERC is the challenge of reaching every child with the vaccine, addressing performance gaps in Kano and security issues in Borno and Yobe.
In Kano, levels of immunity must be increased as they are currently below the threshold of 80% coverage for children of 6 to 9 months. With this unacceptably high proportion of children still being missed by campaigns, there is not a strong enough barrier against the virus should it continue to circulate undetected by surveillance systems. The ERC recommended that measures be taken to increase accountability witg vaccinators being directly observed, and that coverage should be increased through health camps and vaccinations in markets.
The ERC marked its appreciation of the valiant efforts made by health workers to protect children in insecure areas. Despite the challenges, 2.5 million doses of OPV were administered between May and December 2014 in Borno and Yobe, despite inaccessible areas in Borno increasing from 17% to 60% of the province during the same time period. To respond to this, the ERC recommended increasing the number of permanent transit vaccination points to reach children as they enter and leave inaccessible areas.
The ERC stated that from this point forward, the detection of a case of wild poliovirus from any source in Nigeria would constitute a National Public Health Emergency. They recommended that a National Emergency Outbreak Response Plan be drafted accordingly, so that immediate, large scale mop-up activities could be rolled out immediately should that eventuality occur.
With these cautions in mind, six months with no cases of polio reported in Nigeria does mark a significant achievement for the programme. Achieving a polio-free Nigeria is more achievable now than it has ever been. The ERC recommended that Nigeria initiate a government –led polio legacy planning process to document lessons learned and plan for the future contribution of this innovative programme to other public health and development goals.
The guarantee of a polio free future is a gift that Nigeria can deliver to children across the African continent if they sustain the hard-won gains and address the risks that threaten interruption of the virus.
2015 marks the year of one of the largest globally-coordinated vaccine introduction projects in history. Inactivated polio vaccine (IPV) will be introduced into more than 120 countries currently using only oral polio vaccine (OPV), in advance of the phased removal of OPVs in 2016. While OPV is extremely safe and has led the world to the threshold of being polio-free, on very rare occasions, its use can lead to vaccine-associated cases. For this reason, the global eradication of polio requires the cessation of all OPV use, once polio has been eradicated. IPV will at that time be the only option for countries to maintain immunity levels.
The global IPV introduction effort got underway in late 2014 – the Philippines, Vietnam and Tunisia just some of the countries introducing IPV, with countries across Asia-Pacific scheduled to follow in the first few months of 2015. The world is closely watching the experiences of introducing this vaccine in the Western Pacific, as this Region has a long history of leadership on polio eradication. The successful strategies first developed, trialled and taken to scale here are helping inform the eradication strategies in the remaining polio-affected countries of the world.
Now, the Region is again showing its leadership, and lessons learned here will help inform countries’ introduction plans elsewhere. The aim is to ensure that all children – no matter where they live – can be protected from lifelong polio paralysis. Because introducing a new vaccine into the routine immunization programme is no easy feat, it’s also about getting vaccines to the right place, at the right time, in the right condition.
The successful introduction of IPV in countries such as Nepal, Philippines and Vietnam, supported by WHO and UNICEF, shows that high level political commitment is a critical factor, filtering through to bolster many aspects of the programme. In all three countries, cold-chain capacity was reviewed and expanded ahead of the introductions, health workers were trained and equipped with updated data collection tools, and communities mobilized.
The introduction of IPV is also being used as an opportunity to evaluate broader routine immunization services in targeted countries, and to identify potential operational gaps which can now be addressed. For example, countries are taking advantage of the focus on IPV introduction to adapt community awareness materials, to update registers and forms comprehensively, and to expand health worker trainings. Such system strengthening efforts are helping to ensure that all children are not only protected by IPV against polio, but indeed will be even more comprehensively reached with all vaccine-preventable diseases.
All of this is part of the comprehensive Polio Endgame Plan, designed to secure a lasting polio-free world by 2018. Implementation of the Endgame Plan would not be possible without the critical and ongoing support of the international development community, including Australia, Japan, Norway, the United Kingdom, the Bill & Melinda Gates Foundation and Rotary International. Without these vital contributions, activities outlined in the Polio Endgame Plan could not be financed, and could not be implemented. It will ensure that no child will ever again be paralysed by polio, and that the world can reap savings upwards of US$50 billion over the next 20 years (mostly in developing countries).
It is a perfect example of aid dollars in action – helping secure a lasting polio-free world, that will be a gift for all future generations to come.
24 January 2015 marks six months with no cases of wild polio reported in Nigeria, the only remaining endemic country in Africa. This milestone marks a major achievement for the global programme, which has faced significant challenges in Nigeria in past years. Through increased political commitment, programmatic innovations and determination from a huge number of stakeholders, Nigeria has taken a significant step forwards. While the need for vigilance remains, the country has never passed six months without a case, leading to a cautious hope for the programme.
Case numbers in Africa decreased by 92% between 2013 and 2014. In 2013, outbreaks in central Africa and the Horn of Africa, plus continued transmission in Nigeria, left children across the continent at risk of polio. However, 2014 saw the outbreaks slow, and no case of wild polio has been reported across the whole continent since August 2014.
Progress in Nigeria is the result of incredible efforts from the national polio eradication programme with support from the partners of the Global Polio Eradication Initiative. For years, Nigeria posed one of the greatest challenges to global eradication, with many children missed during vaccination campaigns in hard to access areas and low levels of campaign quality. More children than ever before are being immunized, with data indicating that as many as more than 90% of children having received more than three doses of oral polio vaccine, including in traditional high-risk areas.
Increased insecurity in northern Nigeria has posed a significant challenge to eradication efforts in recent months. And key challenges remain. In some areas, access remains an issue and strategies focus during and in-between campaigns to enhance immunity, including through special outreach in hard-to-reach communities, focus on internally-displaced persons camps and providing additional health services in health camps.
At the same time, a persistent circulating vaccine-derived poliovirus type 2 outbreak must be stopped. As part of this, vaccine mix is being optimised during upcoming immunization campaigns, including in key areas with inactivated polio vaccine, to ensure immunity levels to both type 1 and type 2 poliovirus can be further raised. And subnational surveillance gaps must be fully filled, to enable the rapid detection (and subsequent response) to any residual virus transmission.
The Expert Review Committee on Polio Eradication and Routine Immunization (ERC), the country’s technical advisory body, is meeting on 21-22 January 2015 to review current epidemiology and put in place an aggressive plan to ensure a polio-free Nigeria can be rapidly achieved in 2015.
Despite the major progress in Nigeria in 2014, focus must be maintained for the critical months ahead. The gains that have been made are delicate. Losing momentum now, when so much has been done to protect children across Africa, would be a major setback for the global programme.
At its October 2014 meeting, the Strategic Advisory Group of Experts on immunization (SAGE) – the independent body advising the World Health Organization (WHO) on immunization – concluded that preparations for oral polio vaccine type 2 (OPV2) withdrawal in early 2016 are on track. This conclusion is critical in achieving objective 2 of the Polio Eradication & Endgame Strategic Plan 2013-2018. With wild poliovirus type 2 already eradicated since 1999, the aim is to remove the risk of new circulating vaccine-derived poliovirus type 2 (cVDPV2) from emerging, by switching from trivalent OPV (containing type 1, 2 and 3 serotypes) to bivalent OPV (containing only type 1 and 3 serotypes) in routine immunization programmes. Over 90% of cVDPV cases are due to the type 2 component contained in trivalent OPV.
But what does it all actually mean?
Well, from an operational point of view, it means impressive logistical accomplishments must be achieved in record time, both at the global, regional and country level.
The polio world is involved in plans to introduce inactivated polio vaccine (IPV) into the routine systems of 119 countries that currently use only OPV by end-2015, one of the largest globally-coordinated vaccine introduction projects in history. But over and beyond this ambitious vaccine introduction project, additional equally-impressive feats need to be implemented to make the trivalent OPV to bivalent OPV switch a success.
All countries will need to switch the vaccines in their routine immunization programmes in April 2016 (the current target date for the switch). During a two-week switch period, each country will elect a National Switch Day. Such global coordination is necessary to minimise the risk of one country continuing to use trivalent OPV and inadvertently re-infecting another country no longer using the vaccine with cVDPV2.
The GPEI is working with countries, regions, partners and manufacturers to ensure vaccine supply for both vaccines is adequately managed, to reduce the number of doses of trivalent OPV stock that will remain to be withdrawn. Regular stock takes of trivalent OPV will begin in 2015 to calculate accurate supply needs of this vaccine through to the switch date, and orders and shipments adjusted accordingly. The aim is to ensure sufficient trivalent OPV stock is available until the very last day, while minimising the stock that is left to be withdrawn subsequently. Countries will need to pre-identify service points to collect the stock and ensure proper disposal. A one-week buffer supply will be calculated and maintained, to ensure no child remains unimmunized inadvertently during the switch window. Manufacturers will stop producing trivalent OPV.
Ahead of this time, the financing and supply of bivalent OPV must be secured by close coordination with manufacturers from around the world.
This switch has potential implications on cold-chain capacity for the vaccines. Although bivalent OPV will have similar cold-chain volume requirements as trivalent OPV, it will not be identical and so countries will ensure that requirements are adequately re-calculated and re-furbished as needed. Health workers from the public and private sector must be trained and communities sensitised to the importance of vaccinating children with the correct vaccine. Even healthcare stationary needs to be re-printed, such as re-labelling trivalent OPV with bivalent OPV on vaccination cards, stock records and tally sheets. Parents and communities at large will be sensitized to the benefits of the new vaccine.
Finally, a global stockpile of 500 million doses of monovalent OPV type 2 (mOPV2) is being secured be secured and maintained, and global consensus on its use and management reached should type 2 poliovirus re-emerge anywhere in the world. Because the last thing the world needs is for some countries to start using this vaccine unless absolutely needed, thereby raising the spectre of further type 2 vaccine-derived polioviruses from emerging.
The operational guidelines for the global switch are expected to be endorsed by Member States at next year’s World Health Assembly. But already, countries are preparing in full force for April 2016. It is yet another example of the global commitment behind the worldwide drive to secure a lasting polio-free world.
This week, 18 countries across western and central Africa have been holding synchronised polio immunization campaigns to reach nearly 94 million children with oral polio vaccine (OPV). This is a monumental coordination effort, incorporating strong governmental commitment, global support from international organisations such as the World Health Organization and UNICEF and the motivation of members of communities themselves to mobilize their friends and neighbours to ensure every child is protected.
National Immunization Days in Angola, Benin, Burkina Faso, Cameroon, Central African Republic, Chad, Cote d’Ivoire, the Democratic Republic of the Congo, Equatorial Guinea, Gabon, Gambia, Ghana, Guinea Bissau, Mauritania, Niger, Nigeria, the Republic of the Congo and Senegal are working to build immunity across western and central Africa. Each child needs at least 3 doses of OPV to build immunity and end the transmission of the virus, making it crucial that campaigns such as this reach every child.
Africa is closer than ever before to achieving eradication, with only 22 cases across the continent to date in 2014 compared to 232 by the same point in 2013. This decrease of over 90% in one year is due to increased commitment from the governments of the last remaining endemic country in Africa, Nigeria, and the sites of current outbreaks in Cameroon, Equatorial Guinea, Somalia and Ethiopia.
Nigeria saw only 6 cases in 2014 compared to 53 in 2013 by this date. This dramatic improvement can be attributed to measures put in place to avoid missing children from campaigns, and to a surge in staff to the country to support Emergency Operations Centres. The international spread of polio, affecting Cameroon, Equatorial Guinea, Somalia and Ethiopia as well as countries in the Middle East, lead to the declaration of polio as a Public Health Emergency of International Concern (PHEIC) in May 2014 by the Director General of the World Health Organization. With temporary recommendations to stop the international spread of polio, the PHEIC is another step towards ensuring a polio-free Africa.
Through these measures – improved surveillance, innovative community engagement strategies and a surge in staff to affected areas – the past year has seen gains in the eradication effort that must be protected. Synchronized campaigns such as this bring us ever closer to the important milestone of ending transmission in Africa.
These synchronised campaigns demonstrate the commitment of the governments of countries across central and western Africa to ending the transmission of polio once and for all, despite the increased focus on Ebola prevention and response in 2014. In some cases, polio resources are being utilized to strengthen the Ebola response, demonstrating the Global Polio Eradication Initiative’s commitment to securing the polio infrastructure for a polio-free world.
Nigeria is on the last lap towards polio eradication with tremendous progress over the past two years but the battle is not yet over.
Intensified efforts are underway in Northern communities to mobilize communities for polio campaigns through varied communications interventions
Women's compound meetings are targeting high risk communities where resistance to oral polio vaccine is strong.
Aminu Ahmad is the President of Kano’s Association for Polio Victims. He runs his own tricycle business where 80% of employees are people with polio.
Aminu is actively involved in community mobilisation efforts in high risk communities to bring about change and acceptance of immunization, both polio and routine.
Traditional leaders play a key role in addressing resistance to immunization thanks to their status and high respect in communities.
During campaign ‘flag offs’ traditional leaders often vaccinate eligible children in the communities including their own children.
Papa Lolos (Village clowns) are actively engaged during campaign flag offs to draw out the crowds while vaccination team waits to capture all eligible children.
Majigi films – locally produced films that include drama and polio facts – are widely used during community dialogue and compound meetings to strengthen the impact of communication.
Majigi films engage their audience and prepare the women for a dialogue with the health educator following the screening.
Aminu does his part in high level advocacy too and was invited to address the Kano Emirate Council.
Certain religious sects still have strong anti-immunization attitudes. With the help of Emirs and religious scholars efforts are underway to overcome them.
Okada bikers (taxis) are used in Zamfara to inform and mobilise communities during the week leading to the campaign.
Nigeria will have to reach every last child in the next six months to be able to stop the transmission of the wild polio virus in Northern Nigeria.
Grand Imam of Al-Azhar receiving Muslim Scholars to discuss children rights to be protected by vaccination WHO/EMRO
Cairo, 7 March 2013 – The Grand Imam of Al-Azhar, Doctor Ahmad Al Tayyeb, today called for the protection of Muslim children against poliovirus transmission by ensuring they receive the required polio vaccine. He stressed the importance of increasing the awareness of the correct Islamic teachings on the subject to combat all deformed and false beliefs, and confirmed that Al-Azhar is ready to continue to exert all efforts to enlighten Muslim individuals and communities about the rights of children to be protected against polio and all other diseases and the obligation of all muslims to ensure that their children are protected. “Crippled children lead to a crippled Muslim Ummah” Dr Al-Tayyeb warned.
This was announced today at a meeting held at Al-Azhar during which the Grand Imam met with Muslim scholars from several countries. The scholars expressed their solidarity with the children of the Islamic world and reaffirmed their resolve to support the people, health workers and governments of the three countries where polio is not yet eradicated, namely Afghanistan, Nigeria and Pakistan.
The Global Polio Eradication Initiative, launched in 1988 by the health ministers of the Member States of the World Health Organization, has been successful in stopping the transmission of this crippling disease in all but these three countries of the world. Except for in Afghanistan, Nigeria and Pakistan, Muslim communities and countries everywhere have eradicated polio, including 54 out of 57 member states of the Organization of Islamic Cooperation (OIC) that have successfully interrupted transmission of wild poliovirus. This has been achieved through the application of proven eradication strategies, the administration of the safe oral polio vaccine and with financial and political support from the Islamic world.
Recognizing with grave concern the ongoing transmission of wild poliovirus in parts of Afghanistan, Nigeria and Pakistan, and the remaining political, cultural, societal and security challenges preventing all children in these areas from being vaccinated against polio, and in particular the tragic and deadly attacks against frontline health workers in parts of Pakistan and Nigeria in the past three months, Islamic scholars from several countries are meeting for two days in Cairo from 6–7 March to discuss the major obstacles preventing these countries from stopping polio transmission and trying to reach a consensus on how the Islamic leadership can help Muslim communities to overcome these barriers and ensure protection for all Muslim children.
12 February 2013 – Following the notification on 3 January 2013 of a wild poliovirus type 1 (WPV1) case in Niger, outbreak response is continuing in the country. A WPV1 case had been detected from Tahoua region, with onset of paralysis on 15 November 2012 (the first case in the country since December 2011). Genetic sequencing confirmed that the virus was a new importation into Niger, most closely related to virus circulating in Kaduna state, Nigeria.
The Government of Niger is continuing to implement a comprehensive response in line with international outbreak response guidelines issued by the World Health Assembly (WHA) in Resolution WHA59.1. Following an initial supplementary immunization activity (SIA) on 15 January 2013 to reach approximately two million children with bivalent oral polio vaccine (OPV), nationwide SIAs were conducted from 2-5 February 2013, targeting more than five million children with trivalent OPV. A second nationwide SIA is planned for 2-5 March with bivalent OPV. Previously, nationwide SIAs had been conducted on 23 November 2012 with bivalent OPV. A joint national and international team of epidemiologists and public health experts has been deployed by the World Health Organization’s (WHO) Regional Office for Africa to assist the Government of Niger in the investigations, help plan response activities and support active searches for additional cases of paralytic polio.
This event confirms the risk of ongoing international spread of a pathogen (WPV) slated for eradication. In May 2012, the completion of polio eradication was declared a programmatic emergency for global public health by the WHA in Resolution WHA65.5. Given the history of international spread of polio from northern Nigeria across west Africa, WHO assesses the risk of further international spread from Nigeria as high. Based on the history of previous importations to Niger and the ongoing response, WHO assesses the risk of further international spread from Niger as moderate to high. This risk is currently magnified by large-scale population movements across the region associated with insecurity in Mali. To minimize this risk, multi-country synchronized SIAs are planned across 13 countries of west Africa in late April and late May, using a combination of bivalent and trivalent OPV.
Due to the persistence of subnational surveillance gaps in some areas of west Africa, undetected further circulation cannot be ruled out at this time. Investigations are ongoing to more clearly identify surveillance gaps in the region, including among mobile, migrant and underserved populations. Measures are being implemented to strengthen sub-national surveillance, to ensure that all groups and areas, particularly high-risk populations, are covered by high-quality surveillance.
As per recommendations outlined in WHO’s International travel and health, travellers to and from Niger, and other polio-affected countries, should be fully protected by vaccination. It is important that all countries, in particular those with frequent travel and contacts with polio-infected countries, strengthen surveillance for cases of acute flaccid paralysis (AFP), in order to rapidly detect any new poliovirus importations and facilitate a rapid response. Countries should also analyse routine immunization coverage data to identify any subnational gaps in population immunity to guide catch-up immunization activities and thereby minimize the consequences of any new virus introduction. Priority should be given to areas at high-risk of importations and where OPV3/DPT3 coverage is <80%.